
Abstract
Study Design
Systematic review and Meta-analysis.
Objectives
This study aims to evaluate the efficacy, postoperative outcomes, and potential complications of using expandable cages in cervical spine surgery.
Methods
A comprehensive search was performed across Medline, Scopus, Web of Science, Cochrane, and Embase up to May 22, 2023. Meta-analyses and subgrouping analyses were performed using “OpenMetaAnalyst” and R software to analyze efficacy outcomes and complications. The assessment of heterogeneity utilized the i2 and chi-squared tests, applying the random effect model.
Results
Thirty studies were included, with 22 eligible for meta-analysis. The pooled data showed a significant improvement in the Cobb angle, Nurick’s score and modified Japanese Orthopedic Association (mJOA) score. The pooled stability rate post-surgery was 0.94 based on 7 studies, but the stand-alone cages showed a lower stability rate (0.83). Fusion rate showed high success at 0.94 across 14 studies but also the fusion rate in the stand-alone group was lower (0.89) with substantial heterogeneity (I2 = 91.81%) suggests that stand-alone cages may not consistently achieve the same level of fusion as cages with anterior plating (fusion rate of 0.98, I2 = 0%). Dysphagia was observed in 16% of patients, and hardware-related issues were reported in 9% of cases.
Conclusions
expandable cages offer significant advantages in terms of fusion, stability, and neurological recovery. In particular, stand-alone expandable cages were associated with higher rates of complications, including dysphagia, subsidence, and hardware failure, compared to cages with anterior plating.
Introduction
Cervical myelopathy is a common disorder of the cervical spine caused by a variety of factors that include trauma, degeneration, neoplasm and infection.1,2
Cervical spondylosis is the most common non-traumatic cause for myelopathy, it is a progressive degenerative disorder in which the diameter of the cervical spinal canal diminishes with degeneration of the cervical disc leading to its collapse, osteophytosis within the vertebral body, hypertrophy of the facets and laminal arches and ossification of the posterior longitudinal ligament (OPLL). 3
Surgical intervention is the optimum treatment option so, various techniques were described for decompression such as discectomy and laminectomy, however, anterior cervical corpectomy remains the mainstay of management. 2
The level of corpectomy is done according to the number of the affected segments. It is thought that the higher the number of levels resected, the higher the failure rate, that’s why the optimal approach for multilevel corpectomy is still unclear.2-4
Reconstruction following corpectomy can be done using bone grafts or synthetic materials, bone grafting includes iliac crest autograft, allograft, or fibular strut graft nevertheless, autograft harvesting has its demerits as donor site pain, infection, fracture, and poor bone quality. Allogenous bone may undergo resorption that results in graft collapse or extrusion.4-6
Taking this in consideration, variable fusion cages have gained acceptance including titanium mesh and polyetheretherketone (PEEK) but lately expandable cages has shown superiority because they can be placed into the defect and precisely adjust to the size of the corpectomy. They can act as a load-sharing device and provide maintenance of cervical lordosis, thus help reducing stress at the screw-plate interface avoiding graft related complications.5-7
Expandable cages can be solitary set up as a stand-alone cage yet, for providing further stability additional plating either anterior or posterior maybe added. Moreover, cages with direct fixation wings have been created in order to make the procedure more simple. 6
Studies have also shown that although expandable systems can serve as solid constructs, restoring normal alignment and height of the spine, the rates of complication and re-operation, especially in tumor patients, remain high. 7
In this study, we review using expandable cages for anterior cervical corpectomy and reconstruction regarding their efficacy, post-operative outcomes and possible complications.
Methods
We performed this study in adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 8
Search Strategy and Study Selection
We conducted a systematic search by title and abstract on the following databases: Medline (through PubMed), Scopus, Web of Science, Cochrane and Embase up until 22nd of May 2023. We used the MeSH database to retrieve the synonyms of our search strategy, and the terms were combined using “OR” and “AND” Boolean operators, in accordance with the Cochrane Handbook for Systematic Reviews (Chapter 4.4.4).
9
The terms were as follows: ((“Anterior corpectomy” OR “Anterior cervical discectomy and corpectomy” OR ACDC OR “Cervical corpectomy” OR “Decompressive corpectomy” OR “Anterior decompression and fusion” OR ADF OR “Anterior cervical decompression and fusion with corpectomy” OR ACDF OR “Anterior cervical vertebrectomy” OR “Anterior cervical osteotomy and corpectomy” OR “Anterior cervical resection and fusion” OR ACRF OR “Anterior cervical spine surgery with corpectomy” AND “Myelopathy OR Spondylosis OR Spondylolisthesis OR Spondylolysis OR “Spinal Osteophytoses” OR “Spinal Osteophytosis” OR “Ossification of Posterior Longitudinal Ligament” OR “Intervertebral Disc Degenerations”). Following the removal of duplicates, a team of 7 authors screened the retrieved studies based on our predefined eligibility criteria using titles and abstracts. Additionally, we conducted a manual search by reviewing the references of the included articles, and literature reviews for possible relevant studies. Subsequently, the list of included studies was subjected to further scrutiny by two authors. Studies deemed relevant and any conflicts were subjected to full-text screening. The detailed search process and the selection of studies are elaborated in the accompanying PRISMA diagram (Figure 1). PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases and registers only.
Eligibility Criteria
We incorporated studies that assessed the anterior cervical corpectomy with an expandable cage in individuals with myelopathy. There were no restrictions placed on language or study type. To ensure the quality and relevance of the included studies, we excluded duplicate publications, reviews, letters to editors, book chapters, animal and laboratory studies and in vitro investigations.
Data Extraction
Four authors undertook the task of extracting data from the included studies, entering the collected information into an Excel spreadsheet. To guarantee data accuracy and consistency, fifth author meticulously reviewed the completed extraction sheet, reconciled any discrepancies, and validated the precision of the data.
The data extraction encompassed several key elements, starting with study characteristics such as the first author’s name, publication year, study design and duration of the disease under investigation. Population characteristics, including sample size, gender distribution, age demographics, interventions administered, Indications for surgery, complications (dysphagia, epidural hematoma, neck pain, transient vocal cord paralysis, transient neurological worsening, and hardware-related issues) and efficacy outcomes. Furthermore, when applicable data on the used cage, different scores such as modified Japanese orthopaedic score (mJOA) and stability rate were available we gathered it also.
For the quantitative analysis, the same authors independently extracted related information; the reported pain scales (before, during and after the surgery), Nurick score, mean hospital stay, mean blood loss, mean surgical time, mean kyphosis and cervical lordosis angle, successful fusion percentage, C2–C7 Cobb’s angle pre and post operation and Mean duration of follow-up.
The data of interest were collected in the form of mean and standard deviation or number and total. Data reported using different formats were converted into mean and standard deviation values using the website developed by McGrath et al which is an online tool used to facilitate the estimation of sample mean and standard deviation, ensuring consistency in the data presentation and analysis. 10
Critical Appraisal Tool and Risk of Bias Assessment
Two authors conducted an assessment of the risk of bias in the included studies. The National Institute of Health (NIH) Quality Assessment Tools for Observational Cohort and Cross-sectional Studies and case series studies were employed for this purpose. 11
The assessment involved rating studies on a scale of 0 for poor (0-4 out of 14 questions), i for fair (5-10 out of 14 questions), and ii for good (11-14 out of 14 questions) in case of the first tool while in the second tool it addressed nine questions addressing the study objective or question, population, intervention, outcomes, follow up, statistical method and result reporting. In cases where certain questions were not applicable (NA) or not reported (NR), these designations were used accordingly. For case-control studies, the Newcastle-Ottawa Scale (NOS) was utilized. 12 This scale assigns ratings ranging from 0 to 9, with studies scoring within the range of 0-2 being categorized as poor quality, those scoring 3-5 as fair quality, and those scoring 6-9 as good/high quality. For case-report studies, the Jonna Briggs Institute (JBI) critical appraisal tool, which consists of eight questions that evaluate the methodological quality of a study and determine the extent to which a study has addressed the possibility of bias in its design, conduct, and analysis was used. 13
In instances where differences in assessment arose between the two authors, a third author was involved to mediate and resolve any disagreements, ensuring the integrity and consistency of the risk of bias evaluation process.
Data Analysis
Our meta-analysis was conducted using the “OpenMetaAnalyst” software and meta-package of the R software (R version 4.1.0), encompassing a systematic approach to extract and analyze data from the selected studies. 14 In the initial analysis, we focused on mean values and measures of reported scores such as mJOA and Nurick before and after the treatments at different timing when available. For this analysis, we conducted a pooling of mean values for each score separately. The mean difference also has been calculated for some analysis such as pre and post operation angel changes. Also, pooling for the proportions and risk ratio analysis have been conducted. We assessed the heterogeneity using the I2 and chi-squared tests and applied the random effect model. Heterogeneity was considered substantial when I2 was more than 50% at a P-value <0.05. Funnel plot wasn’t made due to the low number of studies (<10) in each subanalysis.
Results
Search Results
Our search process retrieved 5796 records. We identified and removed 2861 duplicates using EndNote software. 2935 records were screened by title and abstract using preformed excel sheet, 2753 were excluded for not matching our eligibility criteria. We identified and retrieved 182 articles for full text screening, 170 articles were excluded; 162 were considered not relevant, 6 reviews, one editorial and an abstract of an already included study. 12 studies were qualified from the screening process while 18 studies were identified by manually searching the databases and references of the related studies; the net result of the included studies is 30 studies. Figure 1 illustrates the PRISMA flow diagram.
Characteristics of the Included Studies
Summary of the Included Studies.
We used New castle-Ottawa scale (NOS) for observational studies to assess the risk of bias in 8 studies; two studies was scaled good, 5 studies was scaled fair while one study was scaled poor quality (Supplement Table 1). According to Quality Assessment Tool for Case Series Studies (NIH), four of five studies was of good quality while one study was of fair quality (Supplement Table 2). We used Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (NIH) to assess the quality of 16 studies; four studies were of good quality while twelve was of fair quality (Supplement Table 3). In one case report study, we used JBI Critical Appraisal Checklist for Case Reports to assess quality and the study was of good quality (Supplement Table 4).
Efficacy and Safety Outcomes
Cobb Angle
Five studies involving 296 participants indicated statistically significant improvement of Cobb’s angle after cervical corpectomy compared to pre-operative measurement. The mean difference was 5.29°, 95% CI = [2.87, 7.71], with substantial heterogeneity (I2 = 70%). Subgroup analysis showed a statistically significant improvement in Cobb’s angle compared to pre-operative measurement using an expandable cage with anterior plating (MD = 5.95, 95% CI = [2.78, 9.13]), stand-alone expandable cage (MD = 3.52, 95% CI = [1.24, 5.80]) and stand-alone anchored expandable cage or with anterior or posterior plating (MD = 9.20, 95% CI = [2.21, 16.19]), while the group using expandable cage which is either Stand-alone, with anterior plate, with posterior plate or with anterior and posterior plate showed statistically insignificant decrease in the Cobb’s angle (MD = −1.80, 95% CI = [-11.92, 8.32]). The heterogeneity between the studies in the expandable cage with anterior plating group was substantial (i2 = 75%), see Figure 2. Cobb’s angle after cervical corpectomy compared to pre-operative measurement. MD = Mean difference, SD = Standard deviation, CI = Confidence interval, P = P value.
Nurick’s Score
Six studies involving 281 patients indicated improvement of Nuruick’s score -decrease- throughout the follow up. The overall mean dropped from 2.71 (95% CI = [2.41, 3.02]) pre-operative to 2.06 (95% CI = [1.78, 2.34]) at 6 months and 1.78 (95% CI = [1.0, 2.75]) post operatively (at the end of follow up). The heterogeneity between studies was considerable pre and post operatively – (i2 = 85% and 95% respectively) - while it was moderate at 6 months (i2 = 45%). In Seervi et al, 2023 stand-alone expandable cage group showed improvement of the mean Nurick score by 0.42 points while in the group using expandable cage with anterior plate it improved by 0.65 points at 6 months. In Perrini et al, 2016 using extendable cage with anterior plate it improved by one point while in Tarantino et al, 2016 using Winged expandable cage it improved by 1.41 points at 24 months. Auguste et al, 2007 which used stand-alone anchored expandable cage showed improvement by one point post operatively compared to pre-operative measurements, see Figure 3. Nuruick’s score throughout the follow up. SD = Standard deviation, CI = Confidence interval, P = P value, MRAW = Mean raw.
Modified Japanese Orthopaedic Scale (mJOA)
Five studies including 107 patients indicated improvement of mJOA throughout the follow up. The overall mean increased from 11.96 (95% CI = [10.20, 13.71]) preoperatively to 14.53 (95% CI = [12.28, 16.79]) at six months, 15.03 (95% CI = [14.32, 15.73]) at 12 months and 16.04 (95% CI = [15.18, 16.90]) at 24 months. The heterogeneity between the studies were considerable pre-operatively and at 6 months of follow up while it was substantial at 12 months of follow up. In Perrini et al, 2015, Zairi et al, 2012 and Cabraja et al, 2010 which used expandable cage with anterior plate the mean improvement at the end of follow up was 2.1, 3.19 and 2.7 respectively while in Koing et al, 2014 which used winged expandable cage it was 2.5, see Figure 4. Modified Japanese orthopedic scale (mJOA) throughout the follow up. SD = Standard deviation, CI = Confidence interval, P = P value, MRAW = Mean raw.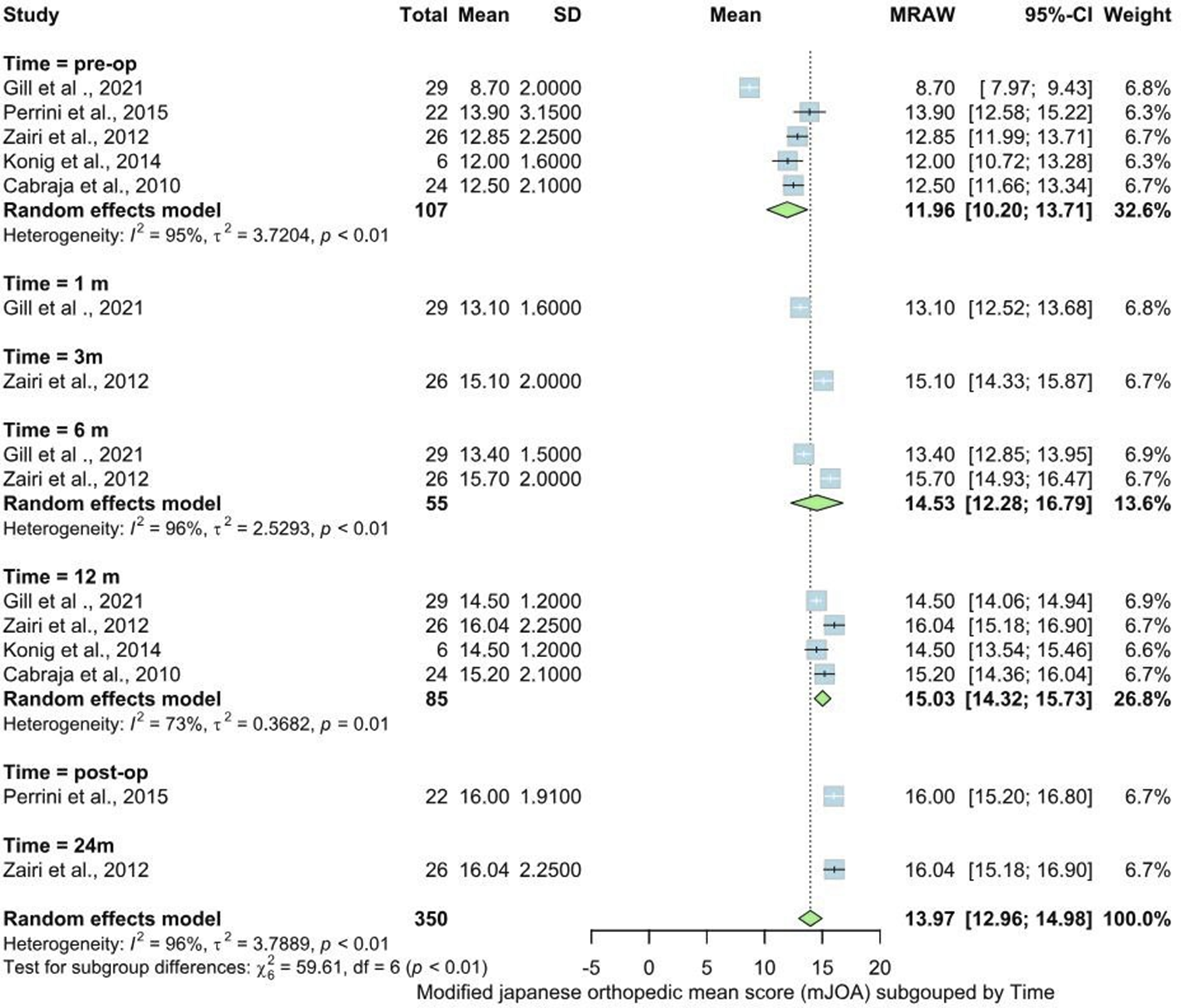
Angels
Five studies including 133 patient showed statistically significant improvement of the angels after cervical corpectomy compared to pre-operative measurements. The mean difference was 5.28°, 95% CI = [3.28, 7.28] with no heterogeneity (i2 = 0%). In the group using stand-alone expandable cage the mean difference was 4°, 95%CI = [0.13, 7.87] while in the group using expandable cage with anterior plate the mean difference was 6.28°, 95%CI = [2.98, 10.65] and in the group using expandable cage with anterior plating with or without posterior plating it was 5.45° 95%CI = [1.19, 9.70] and all showed significant difference compared to pre-operative measurements. The studies in the group using expandable cage with anterior plate were homogenous (i2 = 0%) while in the group using expandable cage with anterior plating with or without posterior plating the heterogeneity was moderate (i2 = 48%) (Supplement Figure 1).
Stability Rate
The outcome was present in 7 studies, the overall stability rate was 0.94, 95%CI = [0.91, 0.98] and the heterogeneity between studies was might not be important (i2 = 8.14%). Sub group analysis showed that the stability rate was 0.95 (95% CI = [0.88, 1.03]) in the group using Expandable cage with anterior plating with or without posterior plating, 0.94 (95% CI [0.86, 1.01]) in the group using expandable cage with anterior plating, 0.91 (95% CI = [0.82, 1.00]) in the group using winged expandable cage and 0.83 (95% CI = [0.41, 1.26]) in the group using stand-alone cage. The heterogeneity between studies in the group using expandable cage with anterior plating was substantial (i2 = 64.67%), while in the groups using winged expandable cage and Expandable cage with anterior plating with or without posterior plating the studies were homogenous (i2 = 0%), see Figure 5. Stability rate after cervical corpectomy. C.I. = Confidence interval, Ev/Trt = Event per treatment, P = P value, NA = Non-applicable.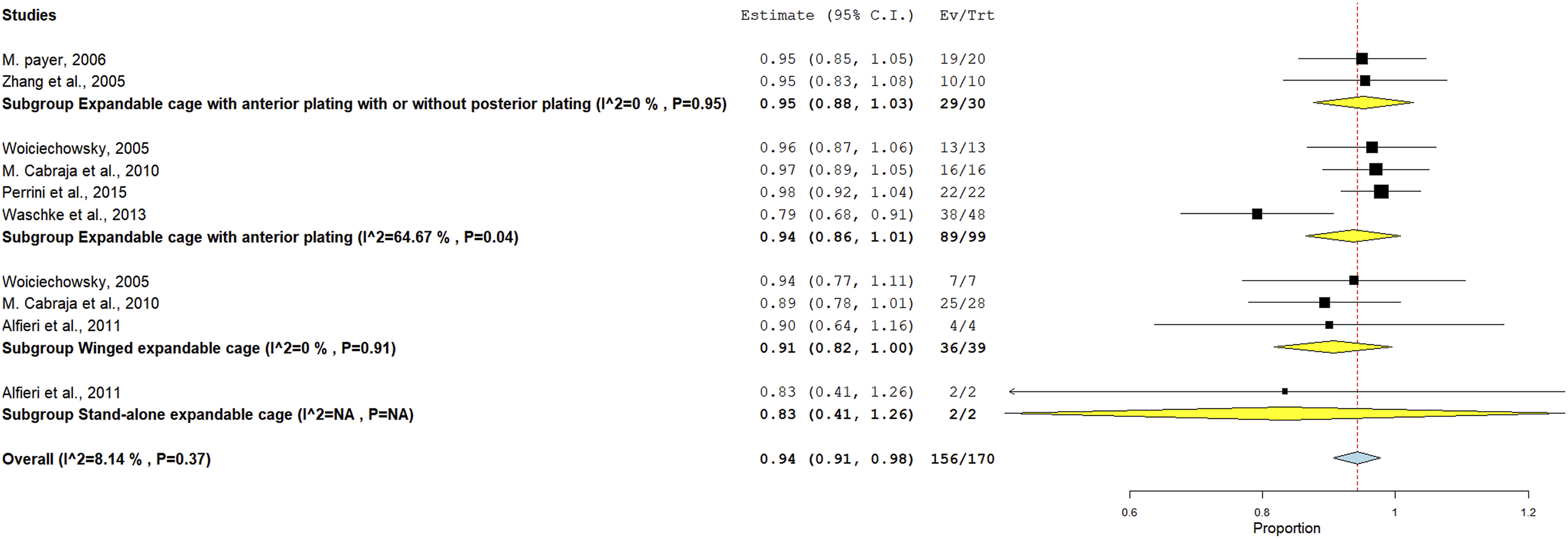
Successful Fusion
This outcome was present in 14 studies, the overall fusion rate was 0.94 with 95% CI = [0.91, 0.97] and the heterogeneity among the studies was moderate (i2 = 54.79%). Subgrouping showed that fusion rate was 0.98 (95% CI = [0.95, 1.01]) in the group using expandable cage with anterior plating with or without posterior plating, 0.94 (95% CI = [0.89, 0.99]) in the group using expandable cage with anterior plating, 0.92 (95% CI = [0.85, 1.00]) in the group using winged expandable cage, 0.78 (95% CI = [0.64, 0.92]) in the group using winged expandable cage with posterior plating, PEEK or iliac bone graft and 0.89 (95% CI = [0.69, 1.09]) in the group using Stand-alone expandable cage. The studies in the group using expandable cage with anterior plating with or without posterior plating and winged expandable cage were homogenous (i2 = 0%), in the group using expandable cage with anterior plating the heterogeneity was not moderate (i2 = 57.36%) while in the group using stand-alone expandable cage it was considerable (i2 = 91.81%), see Figure 6. Successful fusion after cervical corpectomy. C.I. = Confidence interval, Ev/Trt = Event per treatment, P = P value, NA = Non-applicable.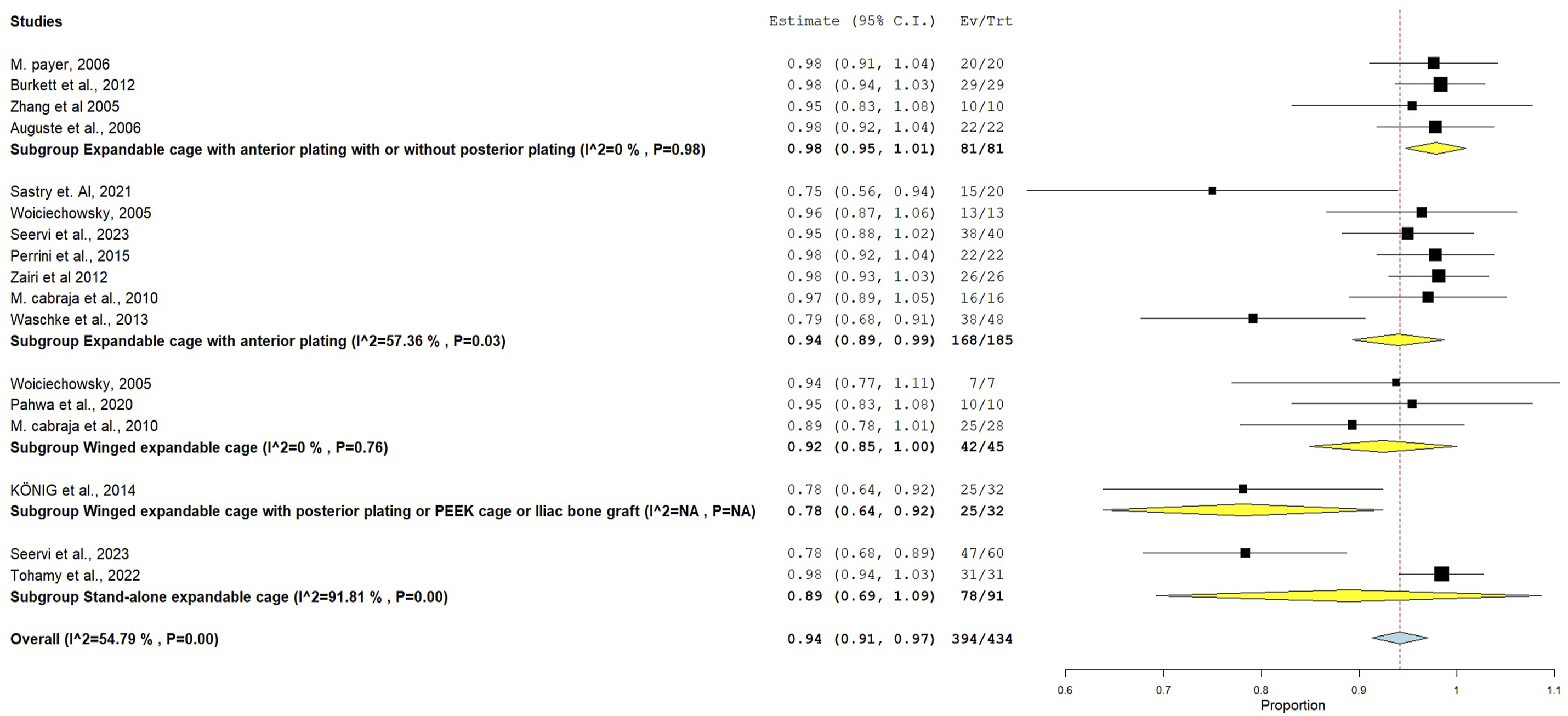
Dysphagia
The outcome was reported in 11 studies, the overall incidence was 0.16 with 95% CI = [0.08, 0.24] and the heterogeneity between the studies was considerable (i2 = 89.4%). Subgroup analysis showed that the incidence was 0.34 (95% CI = [-0.24, 0.93]) in the group using stand-alone expandable cage, 0.20 (95% CI = [0.02, 0.38]) in the group using expandable cage with anterior plating, 0.08 (95% CI = [-0.00, 0.16]) in the group using expandable cage with anterior plating with or without posterior plating, 0.06 (95% CI = [-0.02, 0.14) in the group using winged expandable cage, 0.09 (95% CI = [0.03, 0.15]) in the group using expandable cage which is either Stand-alone, with anterior plate, with posterior plate or with anterior and posterior plate and 0.07 (95% CI = [-0.01, 0.16]) in the group using stand-alone anchored expandable cage or with anterior or posterior plate.
The heterogeneity between studies in the groups using expandable cage with anterior plating and stand-alone cage was considerable (i2 = 93.12% and 97.69% respectively) while the studies in the group using expandable cage with anterior plating with or without posterior plating were homogenous (i2 = 0%) (Supplement Figure 2).
Fractures
The outcome was present in three studies, the overall incidence was 0.06 with 95% CI = [0.01, 0.10] and the heterogeneity between the studies was not important (i2 = 0%). Subgroup analysis showed that the incidence was 0.03 (95% CI = [−0.03, 0.09]) in the group using winged expandable cage, 0.04 (95% CI = [−0.04, 0.11) in the group using expandable cage with anterior plating and 0.10 (95%CI = [0.04, 0.17]) in the group using expandable cage which is either Stand-alone, with anterior plate, with posterior plate or with anterior and posterior plate (Supplement Figure 3).
Hardware Related Issues
The outcome was present in 8 studies, the overall incidence was 0.09 with 95% CI = [0.04, 0.15] and the heterogeneity was substantial (i2 = 65.31%). Subgroup analysis showed that the incidence was 0.12 (95% CI = [−0.04, 0.28]) in the group using expandable cage with anterior plating with or without posterior plating, 0.0.07 (95% CI = [0.02, 0.13]) in the group using expandable cage with anterior plating , 0.03 (95% CI = [-0.03, 0.09]) in the group using winged expandable cage and 0.015 (95% CI = [0.08, 0.23]) in the group using expandable cage which is either Stand-alone, with anterior plate, with posterior plate or with anterior and posterior plate. The studies in the group using expandable cage with anterior plating was homogenous (i2 = 0%), while in the group using expandable cage with anterior plating with or without posterior plating the heterogeneity was substantial (i2 = 86.21%) (Supplement Figure 4).
Transient Neurological Worsening
The outcome was present in 5 studies, the overall incidence was 0.06 with 95% CI = [0.02, 0.11] and the heterogeneity between studies may be moderate (i2 = 43.71%). Subgroup analysis showed that the incidence was 0.05 (95% CI = [−0.03, 0.12]) in the group using Expandable cage with anterior plating with or without posterior plating, 0.04 (95% CI = [−0.04, 0.11]) in the group using expandable cage with anterior plating, 0.03 (95% CI = [-0.03, 0.09]) in the group using winged expandable cage and 0.15 (95% CI = [0.08, 0.23]) in the group using Expandable cage which is either Stand-alone, with anterior plate, with posterior plate or with anterior and posterior plate (Supplement Figure 5).
Hardware Failure Requiring Additional Surgery
The outcome was present in 10 studies, the overall incidence was 0.08 with 95% CI = [0.04, 0.12] and the heterogeneity between the studies was substantial (i2 = 60%). Subgrouping showed that the incidence was 0.05 (95% CI = [0.01, 0.10]) in the group using expandable cage with anterior plating, 0.05 (95% CI = [−0.02, 0.12]) in the group using winged expandable cage, 0.03 (95% CI = [−0.03, 0.09]) in the group using winged expandable cage with posterior plating or PEEK cage or iliac bone graft, 0.17 (95% CI = [0.07, 0.26]) in the group using stand-alone expandable cage, 0.24 (95% CI = [0.12, 0.36]) in the group using expandable cage with anterior plating with or without posterior plating, 0.15 (95% CI = [0.08, 0.23]) in the group using expandable cage which is either stand alone, with anterior plating, posterior plating or with anterior or posterior plating and 0.02 (95% CI = [−0.02, 0.07]) in the group using stand-alone anchored expandable cage or with anterior or posterior plating. The studies in the group using expandable cage with anterior plating was homogenous (i2 = 0%) while in the group using winged expandable cages it was not important (i2 = 29.56%) (Supplement Figure 6).
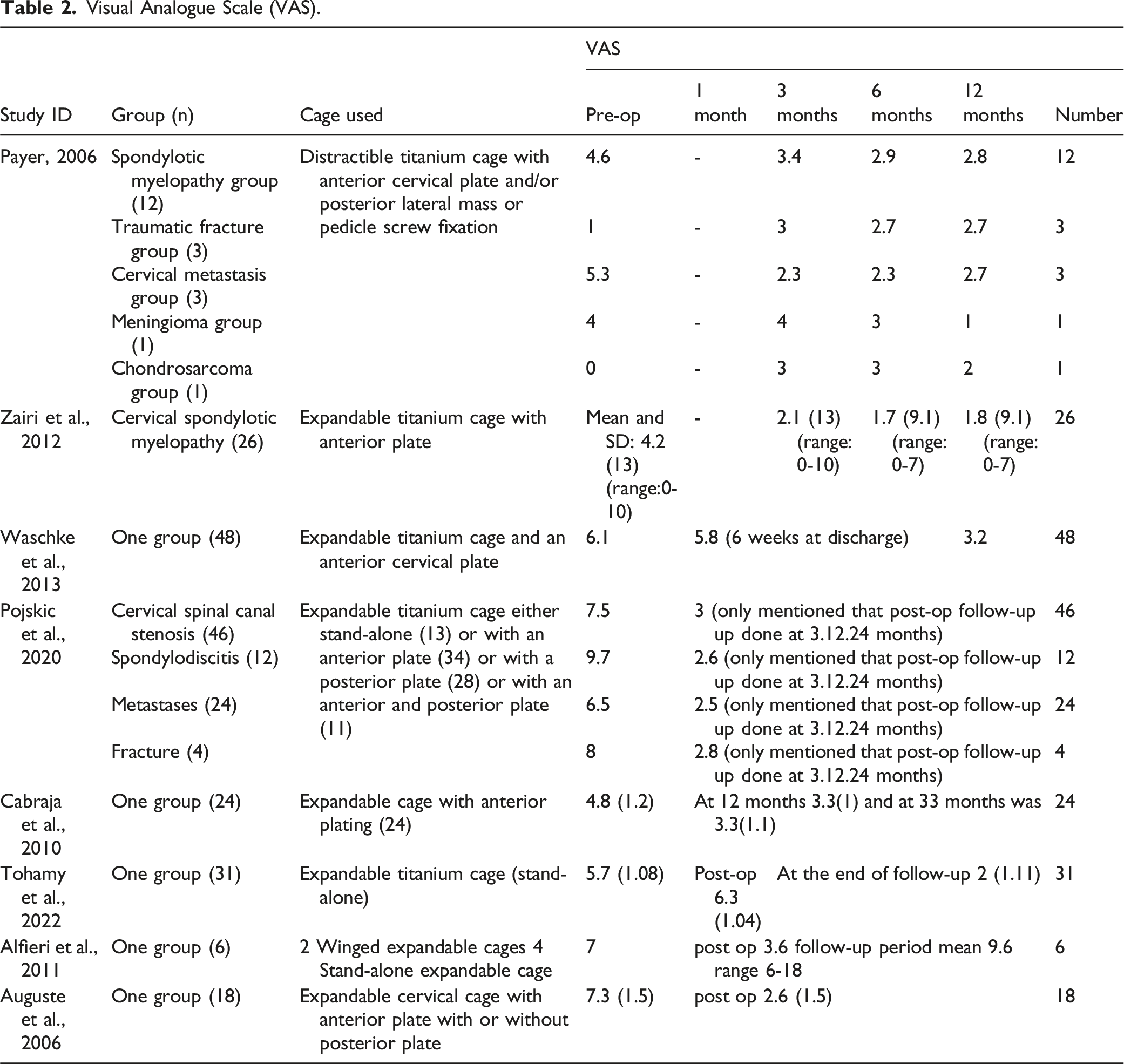
Visual Analogue Scale (VAS)
Visual Analogue Scale (VAS).
The mean duration of follow up was minimally 6 months in Pahwa et al, 2020 and maximally 77.5 in Perrini et al, 2015 (Supplement Table 5) while the mean hospital stay was at least 2.6 in Sastry et al, 2021 and maximally 10.6 in Pojskic et al, 2020 (Supplement Table 6). The mean surgical time was reported in eight of the included studies and it was least in Pahwa et al, 2020 in the group using winged expandable cage while it was most in Burkett et al, 2012 using expandable titanium cage with anterior and/or posterior fixation (Supplement Table 7).
Mean blood loss was reported in 6 of the included studies and it was least in Sastry et al, 2021 using expandable cage with anterior plating while it was most in Payer, 2006 in the group underwent 3 level corpectomy (Supplement Table 8). In four studies which reported epidural hematoma only five patients were involved (Supplement Table 9) while neck pain was reported in 5 studies and involved 22 patients out of 139 patients, 14 of them was in Waschke et al, 2013 (Supplement Table 10).
Subsidence was reported in 11 of the included studies and included 66 out of 454 patients. In Seervi et al, 2023 only 2 patients in the expandable cage with anterior plate group had subsidence while in stand-alone cage group 13 patients had subsidence and in KÖNIG et al, 2014 subsidence didn’t occur in the winged expandable cage group while 6 patients in the PEEK group had subsidence (Supplement Table 11).
Discussion
This meta-analysis synthesized data from 30 studies investigating the clinical outcomes of anterior cervical corpectomy using expandable cages. While the use of expandable cages generally led to favourable outcomes in terms of fusion rates, neurological improvement, and pain reduction, significant variability in outcomes across different cage designs and surgical techniques demands further attention.
Cobb Angle Improvement
The improvement in Cobb’s angle across studies was notable, with an overall mean difference of 5.29°, demonstrating the effectiveness of expandable cages in restoring sagittal alignment. However, the substantial heterogeneity in some subgroups, particularly in the expandable cages without anterior plating (MD = −1.80, 95% CI = [−11.92, 8.32], I2 = 75%), suggests that the lack of additional plating may compromise stability and lead to less favourable outcomes. In contrast, the group using expandable cages with anterior plating showed significant improvement (MD = 5.95, 95% CI = [2.78, 9.13]), highlighting the clinical benefit of anterior plating in maintaining alignment post-operatively.
Given the variability in results, particularly the insignificant change in Cobb’s angle in some subgroups, it is important to consider patient-specific factors and surgical techniques when selecting between stand-alone and plated cages. The substantial heterogeneity suggests that factors such as pre-operative spinal alignment, the extent of corpectomy, and surgical expertise may influence outcomes.
Nurick’s Score Improvement
The improvement in Nurick’s score from 2.71 pre-operatively to 1.78 post-operatively was significant, but the high heterogeneity (I2 = 85% pre-operatively and 95% post-operatively) indicates variability in patient recovery. The subgroup using stand-alone expandable cages showed a smaller improvement (0.42 points), compared to the cages with anterior plating (0.65 points). This suggests that the additional support provided by anterior plating may contribute to better neurological recovery.
The high heterogeneity across studies could be explained by differences in follow-up duration, surgical techniques, or patient characteristics. Addressing these factors in future research will help to refine the use of expandable cages in different clinical scenarios.
Modified Japanese Orthopaedic Association (mJOA) Scores
The mJOA scores improved consistently from 11.96 pre-operatively to 16.04 at 24 months, reinforcing the effectiveness of expandable cages in enhancing neurological function. However, significant heterogeneity was observed pre-operatively and at 6 months of follow-up, reflecting variability in patient response to surgery. The group using expandable cages with anterior plating showed slightly better outcomes (mean improvements ranging from 2.1 to 3.19 points), further supporting the advantage of additional anterior column support.
Given the variability in improvement, clinicians should consider the use of anterior plating, particularly in cases where greater neurological recovery is anticipated. The heterogeneity in outcomes could be due to differences in the extent of myelopathy or surgical technique, warranting further investigation.
Impact of Demographic and Comorbidities
The heterogeneity observed in Nurick’s and mJOA scores across included patient groups subjected to varied demographic factors eg, age, comorbidities, and pre-op myelopathy severity. These two techniques stand-alone and cage plate structures pre-op and post-operative outcomes are differed. Elias et al (2024) also determined in its systematic review and meta-analysis that age of the patient played significant role in choosing between stand-alone or cage-plating. The authors observed better outcomes of stand-alone mostly in old adults than younger or middle age adults. Moreover, cage plating also help to reduce surgical duration, less intraoperative bleed and lower the rates of post-op dysphagia as well as adjacent segment degeneration. 37 Similarly, Tang et al (2023) also explained that the more the severity of myelopathy at pre-op, it may impact on the post op outcomes such as cervical lordosis and disc height that impact on long-term spinal stability and alignment. 38 Moreover, Lambrechts et al (2023) also found that anterior plating is more beneficial among more severe cases of myelopathy but the health-related quality of life may be somehow similar among adults. Stand-alone cages can do better to improve short-term dysphagia and adjacent segment disease, while cage plating increase structural support as well as alignment especially among severe myelopathy cases. 39 Therefore, it is essential to consider patient demographics, comorbidities and pre-operative severity of myelopathy may impact on the selection of technique of cages.
Fusion Rates and Stability
The overall fusion rate of 94% underscores the high success rate of anterior cervical corpectomy with expandable cages. However, the substantial heterogeneity in certain subgroups (I2 = 91.81% in the stand-alone group) suggests that stand-alone cages may not consistently achieve the same level of fusion as cages with anterior plating (fusion rate of 0.94, I2 = 57.36%). The lower fusion rate in the stand-alone group (0.89) highlights the potential limitations of using expandable cages without plating, especially in cases requiring greater biomechanical stability. The literature also reports similar findings, Cohn et al (2024) reported 92.1% fusion rates among patients treated with anterior plating with expandable cages as compared to 75.5% fusion rates in stand-alone. Moreover, the subsidence rate in expandable cages group is also lowered to 46% as compared to stand-alone cage 77.6%. 40 However, the fusion rates also depend upon the involvement of number of spinal segments in surgery. Abdul et al (2024) found that there is no significant difference between both techniques when there is single segment involvement. 41 Similar results were also reported by Elias et al, there is no significant difference of fusion rates among both techniques when there is one spinal segment involvement. 37 However, location of cage especially for stand-alone cage may also impact on the fusion rates eg, cranial placement of stand-alone cage showed better fusion rates as compared to caudal placement. Moreover, the use of expandable cages are reported with better outcomes when it is used with anterior plating, suggesting better clinical outcomes and lower subsidence rates because it improves C2-C7 cobb’s angle and Nurik’s score as compared to stand-alone cage and expandable cage without anterior plating. 24 So it appears that stand-alone cage could be used in single level corpectomy without significant pre operative instability or alignment problems but, this is questionable as it shows major drawbacks compared to expandable cage with anterior plating without evidence of major advantages. Therefore, there is need to consider all these discussed factors while choosing between expandable cages with anterior plating or stand-alone cages, to consider patients characteristics, needs and context of the surgery to optimize patients’ outcomes and reduce the complications.
Similarly, the overall stability rate was high (0.94), but the stand-alone cages showed a lower rate (0.83), reinforcing the clinical importance of anterior plating in enhancing both fusion and stability. The higher heterogeneity observed in the anterior plating group (I2 = 64.67%) suggests that differences in plating techniques, cage designs, or patient factors may influence outcomes.
Complications: Dysphagia and Hardware-related Issues
The incidence of dysphagia was 0.16 overall, with considerable heterogeneity (I2 = 89.4%). Stand-alone cages were associated with a significantly higher rate of dysphagia (0.34), compared to cages with anterior plating (0.08). The variability in dysphagia incidence could be due to the differences in cage design and surgical techniques. The higher incidence of dysphagia in the stand-alone cage group suggests that the lack of additional plating may increase mechanical stress on the oesophagus, leading to post-operative swallowing difficulties. The existing literature also reported varied results on demonstrating the association of dysphagia more in cases of stand-alone cases as compared to anterior plating with cages. However, Tang et al (2023) found that self-locking stand-alone cages incidence rate of dysphagia is lowered as compared to anterior plating cages. 38 On the other hand, Zavras et al (2022) also reported contrasted evidence as the authors reported a higher incidence of dysphagia among cages with anterior plating which showed inconsistency with the results of this study. 42 Moreover, Fayed et al (2021) also found no statistically significant difference of incidence of dysphagia due to cages with anterior plating and stand-alone cages. 43 Therefore, more comprehensive and detailed studies are needed to address this contrasting finding.
Hardware-related issues were present in 0.09 of cases, with substantial heterogeneity (I2 = 65.31%). The group using expandable cages with anterior plating showed a lower incidence of hardware issues (0.07) compared to the group containing the stand-alone cages (0.15). While the heterogeneity in hardware-related issues may be influenced by differences in surgical technique or implant type, the overall lower rate in plated cages suggests that anterior plating contributes to greater implant stability and fewer complications. The similar incidence of hardware failure in expandable cages with anterior plating is also reported by Elias et al (2024). The authors demonstrated that the use of cage plating system in anterior corpectomy help to maintain disc height and cervical lordosis in better way as compared to stand-alone cages. It also explained the lower rates of subsidence and hardware failure issues. 37 Similarly, Tang et al (2023) while comparing both techniques demonstrated that expandable cage provide better height may less likely to cause any hardware failure in future due to its structural construct. 38 Therefore, it is well-document that the expandable cages with anterior plating is more favorable for better clinical outcomes through avoiding hardware failure.
Subsidence and Long-Term Outcomes
Subsidence was reported in 66 out of 454 patients, with a much higher incidence in the stand-alone cage group (13 patients) compared to the anterior plating group (2 patients). Subsidence can significantly impact long-term stability and spinal alignment, potentially leading to recurrence of symptoms or hardware failure. The increased subsidence in the stand-alone cage group highlights the clinical importance of anterior plating in preventing this complication.
Similarly, Jin et al (2021) also explained that there is more chances of symptoms recurrence and lower quality of life due to stand-alone cage subsidence in spinal fusion. It can result sinking into vertebral body that can result into segmental kyphosis, segmental issues and restenosis that results in increase pain and more neurological issues recurrence. 44 Noordhoek et al (2018) also estimated subsidence rates in their systematic review of 83% in stand-alone cage depending upon the surgery. 45 There are some factors which might also be consider to prevent subsidence. In another study, Ran et al (2024) found that there are also association between low bone mineral density, non-modular cylindrical cages, endplate removal after surgery and high subsidence rates as well as poor physical outcomes. 46 However, there are studies which indicate anterior plating with expandable cages not only reduced subsidence rates significantly but also enhanced clinical outcomes due to its stabilizing and supporting function in spinal construct46,47 especially when there is multisegmented surgery. Therefore, these factors may help to comprehend and understand that subsidence can compromise surgical outcomes, particularly in multi-level procedures or patients with pre-existing instability, the use of anterior plating should be strongly considered to reduce the risk of long-term complications.
Visual Analogue Scale (VAS) and Outliers
VAS scores generally decreased across studies, reflecting pain relief after surgery. However, in Payer, 2006, VAS scores increased in both the traumatic fracture group and the chondrosarcoma group. This outlier highlights the potential for different clinical conditions to impact post-operative pain outcomes. The variability in VAS scores across studies underscores the need for careful patient selection and individualized surgical approaches, particularly in complex cases such as traumatic fractures or malignancies.
Hardware Failure Requiring Surgery
The overall incidence of hardware failure requiring surgery was 0.08, with higher rates in the stand-alone group (0.17) compared to the anterior plating group (0.05). This reinforces the importance of anterior plating in reducing the risk of hardware failure. The substantial heterogeneity observed in the hardware failure outcomes (I2 = 60%) suggests that other factors, such as implant design, patient bone quality, or surgical technique, may influence the likelihood of requiring revision surgery.
Comparison to Other Surgical Techniques
Cervical corpectomy with expandable cages showed significant better clinical outcomes and quality of life reported in current literature. Prakash et al (2024) compared expandable with non-expandable cages and observed significant improvement in Nurick grade, pain among patients underwent surgery with expandable cages. 48 In another study, Yusupov et al (2021) used anchored expandable titanium cages which restored physiological sagittal cervical profile, enhanced sagittal alignment, height which remained stable for long duration of time. 31 While Das et al (2023) comparing directly to non-expandable cages, the authors found that the expandable cages showed more improvement in segmental angle and lower the incidence of subsidence while offering higher displacement and re-operation rates. 49 Therefore, clinical outcomes and quality of life significantly improve with anterior corpectomy surgery with expandable cages.
Our Study limitations is the heterogeneity between the studies in the term of, the reconstruction method used, the comparison to which each method compared and the limited number of the studies on each method particularly stand-alone cages which prevents further assessment and decreases the strength of the evidence on each method. Also the heterogeneity in the population characteristics including age, main complaint, specific diagnosis, indication of surgery, baseline neurological state, bone quality, surgical level, technical aspects as cage positioning and others make the evidence synthesis and interpretation very hard. The un availability of primary data regarding the patients’ specific factors or surgical techniques that may affect the outcomes like bone quality, surgical level and cage positioning for each cage type particularly, limits the evidence required to tailor the intervention for each patient. So future research should focus on larger randomized controlled trials to better understand the factors contributing to variability in outcomes, refine surgical techniques and reconstruction methods for optimal patient outcomes.
Conclusion
This meta-analysis provides a comprehensive overview of the clinical outcomes associated with anterior cervical corpectomy using expandable cages. While expandable cages offer significant advantages in terms of fusion, stability, and neurological recovery, the presence of substantial heterogeneity across studies suggests that patient-specific factors, cage design, and surgical technique all play a critical role in determining outcomes.
In particular, stand-alone expandable cages were associated with higher rates of complications, including dysphagia, subsidence, and hardware failure, compared to cages with anterior plating. These findings underscore the importance of considering anterior plating, particularly in cases requiring enhanced stability or where post-operative complications are a concern.
Future research should focus on larger randomized controlled trials to better understand the factors contributing to variability in outcomes and to refine surgical techniques for optimal patient outcomes. Moreover, attention should be given to long-term follow-up to capture late-onset complications such as subsidence and hardware-related issues.
Supplemental Material
Supplemental Material - Safety and Efficacy of Anterior Cervical Corpectomy and Reconstruction With Expandable Cages for Treatment of Cervical Myelopathy-Focusing on Stand-Alone Cages: A Systematic Review and Meta-Analysis
Supplemental Material for Safety and Efficacy of Anterior Cervical Corpectomy and Reconstruction With Expandable Cages for Treatment of Cervical Myelopathy-Focusing on Stand-Alone Cages: A Systematic Review and Meta-Analysis by Ahmed Mahmoud Abouelhamd, Mohamed Marey Hesn, Anas Elgenidy, Omar Alomari, Mohammed Al-mahdi Al-kurdi, Amer Helal, Ayman Abdelaziz Elgharori, Dina Hesham Khattab, Mohamed Gomaa Abdelrahim Farahat, Mahmoud Ragab Zaki Ali and Mohamed Hussein Hassan Tohamy in Global Spine Journal.
Footnotes
Author Contributions
Idea synthesis: MHHT, AA, AE, MMH. Database search: MMH. Screening, Data extraction: MMH, OA, MAMAK, DHK, AAE, MGAF, MRZA. Risk of bias assessment: OA, MAMAK, MMH. Data analysis: AE, MMH. Writing the original draft: AE, MMH, MHHT, AA, AH, OA, MAMAK, DHK, AAE, MGAF, MRZA. Reviewing, Editing and Supervision: MHHT, AA, AH, AE.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statements
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.