
Abstract
Study Design:
Technical report.
Objectives:
Conventional 2-dimensional (2D) video-assisted thoracoscopy (VATS) is a technical procedure mainly performed by experienced surgeons. The technique may, however, come with difficulties in hand-eye coordination and estimation of depth. Three-dimensional thoracoscopy can help overcome these difficulties by providing a stereoscopic 3D view. The objective of this study is to report the first experience and results with 3D thoracoscopy for spine surgery in trauma patients.
Methods:
The first 4 patients treated with anterior stabilization for traumatic spine fractures using 3D thoracoscopy in an academic hospital are described. Baseline characteristics, operative time, and blood loss were retrospectively collected. This data is compared with a cohort of patients treated in the same center with the conventional 2D technique. Additionally, the treating surgeons’ and residents’ experience with the technique is described. Surgical equipment consists of 3D compatible video monitors, a videoscope with 2 cameras, and special glasses to be worn by the personnel.
Results:
Four patients were successfully treated using 3D thoracoscopy. Operative time was comparable to that of the conventional 2D technique and less blood loss occurred. No per- or postoperative complications or problems occurred. Per-operative views were of very high quality and provided improved depth perception. Surgeons and residents deemed the technique helpful, especially during technically demanding aspects of the procedure.
Conclusions:
While a shorter learning curve, decreased surgery time, and blood loss have to be proven in future prospective studies, the first experience with 3D-VATS for spine surgery is positive, and future use in minimally invasive spine surgery seems feasible.
Keywords
Introduction
Severe traumatic thoracolumbar spine fractures that lack anterior stability are indicated for anterior stabilization, generally secondary to posterior fixation. One possible anterior stabilization method is minimally invasive thoracoscopic placement of a distractable cage after partial corpectomy of the fractured vertebra. 1,2 The thoracoscopic approach can, however, be complex and technically demanding. Spatial 3-dimensional (3D) orientation represented on a 2D monitor provides surgical difficulties and lacks depth vision, which could be overcome by 3D visualization during the procedure.
Three-dimensional endoscopy was first applied in laparoscopic abdominal surgery 3,4 and soon followed in thoracoscopic pulmonary surgery. 5 While the first studies in 3D endoscopy did not show superiority over 2D endoscopy, 3,4 the introduction of high-definition imaging and technical improvements led to improved surgical performance in abdominal 6 -9 and pulmonary surgery. The main advantage of 3D video-assisted thoracoscopy (VATS) over 2D-VATS is reported as decreased surgical time. 10 -12 The use of 3D thoracoscopy for the treatment of thoracolumbar fractures or posttraumatic deformities might provide these advantages as well.
The use of 3D thoracoscopy has not yet been reported in spine surgery. We describe the technique, feasibility, experience, and results of the first 4 patients treated with 3D thoracoscopic anterior spine stabilization after thoracolumbar fractures.
Methods
Data Collection
All patients treated with 3D thoracoscopy for traumatic spine fractures in one academic medical center were reviewed. Baseline and per-operative surgical data of the first 4 patients treated with 3D thoracoscopy were collected from the hospital information system. Operative time and blood loss of the 3 patients treated with only anterior stabilization were compared with the mean of the last 10 patients that underwent only anterior stabilization for traumatic spine fractures with conventional 2D thoracoscopy in the same academic medical center. The indication for anterior stabilization in these patients was the same as the indication used for patients treated with the 3D technique and is described in the section “Indications.” Surgeons and residents that performed the surgery were asked for experienced (dis)advantages with the technique and their opinion compared to conventional thoracoscopy. The institutional ethics committee METc VUmc approved this study under number 2017.414.
Operation Room Setup and 3D Image Conception
Operating room setup and positioning of 3D thoracoscopy is the same as traditional 2D thoracoscopy. The standard monitors are replaced by 3D-compatible monitors that can be switched back and forth to normal 2D view per-operative without changing the videoscope. The 3D view is created by 2 video sensors on the videoscope that alternately transmit an image to the high-definition monitors. A videoscope with a flexible camera tip was used. The monitor synchronizes with the respective signals from the video sensors and transmits right and left polarized signals. The surgeons wear special glasses (Figure 1) with respectively a right and left circular polarized lens. The right and left eyes then only receive a right or left image specific signal that are then composed to a stereoscopic 3D image in the brain. Everyone in the room participating or observing the procedure wears the glasses. Although they slightly dim the light intensity, the glasses do not distort normal view and can therefore be worn during the whole procedure, even when the 3D monitors are not used.

Per-operative setting with surgeons wearing 3D glasses.
Surgical Technique
The thoracoscopic surgical technique according to which the procedure was performed was the same as in previously performed 2D thoracoscopy and comparable to the method described in earlier studies. 1,2 As in the 2D surgical technique, the patient is positioned in lateral decubitus position and single lung ventilation is performed. Thoracoscopic partial corpectomy of the fractured vertebra with discectomy is performed with maintenance of the posterior vertebral wall. After this, an expandable titanium cage (Obelisc, Ulrich Medical, Ulm, Germany) is thoracoscopically implanted in the resulting cavity and the adjacent intact vertebrae are connected using anterolateral plating (MACS-TL, Braun, Melsungen, Germany). Finally, the cage is surrounded with corpectomy bone augmented with bone graft from the corpectomy to stimulate bony fusion.
Port placement in 3D thoracoscopy is the same as in 2D thoracoscopy and dependent on fracture level. In the reported patients, 2 types of surgical procedures were performed: “standard” anterior stabilization for fresh spinal fractures and anterior stabilization for posttraumatic kyphosis correction. The anterior thoracoscopic approach was similar for both procedures; however, in posttraumatic kyphosis correction this was combined with posterior instrumentation during the same procedure (which consequently increases operative time and blood loss). Posttraumatic kyphosis correction is a 3-staged procedure; first, thoracoscopic anterior decompression and corpectomy is performed in lateral decubitus position. Then the patient is switched to prone position and dorsal short segment fixation and lordosis are applied. The patient is then switched back to the lateral decubitus position and the expandable cage and anterolateral plate are thoracoscopically implanted. The cell saver is always available during this procedure because of the high risk of large blood loss. The “standard” anterior stabilization for fresh spinal fractures is a 1-stage procedure usually performed 1 to 2 weeks after posterior instrumentation and is therefore without the need of repositioning the patient during the procedure. Lumbar fractures treated with a thoracoscopic approach usually require the crus of the diaphragm to be opened, 2 and this causes 20 to 30 minutes of extra time.
Indications
The patients that were treated with 3D thoracoscopy for acute spinal fractures had an unstable anterior column. This is usually defined by a load sharing classification 13 ≥7. In the acute phase, these patients are first posteriorly stabilized based on an unstable fracture (ligamentous injury; AO type B or C), neurologic injury, or severe deformity (depression >50% or kyphosis >30°). If the anterior column is not deemed stable (usually AO type A2 or A4), often a computed tomography scan is made after 1 week to evaluate the fracture. It is then decided, based on kyphosis, comminution, and fusion, to perform additional anterior stabilization.
Results
Patients
Four patients were operated on using 3D thoracoscopy between September 2016 and May 2017; all were female with a mean age of 46 years. Traumatic spine fractures were located at T10, T11, and L1. Three patients underwent a solely anterior approach, 2 shortly after primary posterior fixation due to an anterior column deficiency and 1 primary anterior treatment without posterior fixation in a pincer AO type A2 fracture. Three patients had a load sharing classification (LSC) of ≥7 and AO fracture types A4. One patient had a LSC of 5 but suffered a pincer AO type A2 fracture with large comminution, which created an unstable anterior column. One patient underwent a (3-staged) posttraumatic kyphosis correction due to pain and a severe preoperative kyphosis (33.4°). Further patient details are described in Tables 1 and 2. The control group consisted of the last 10 patients treated with anterior stabilization for fresh traumatic spine fractures. The group consisted of 6 males and 4 females with a mean age of 40 ± 16 years; there were 6 T12 fractures and 4 L1 fractures.
Patient Characteristics.
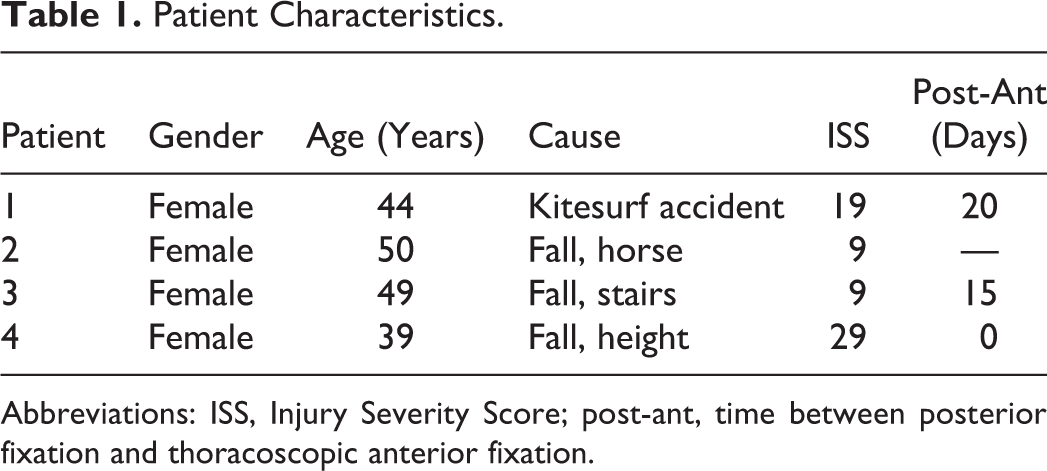
Abbreviations: ISS, Injury Severity Score; post-ant, time between posterior fixation and thoracoscopic anterior fixation.
Fracture and Surgery Characteristics.
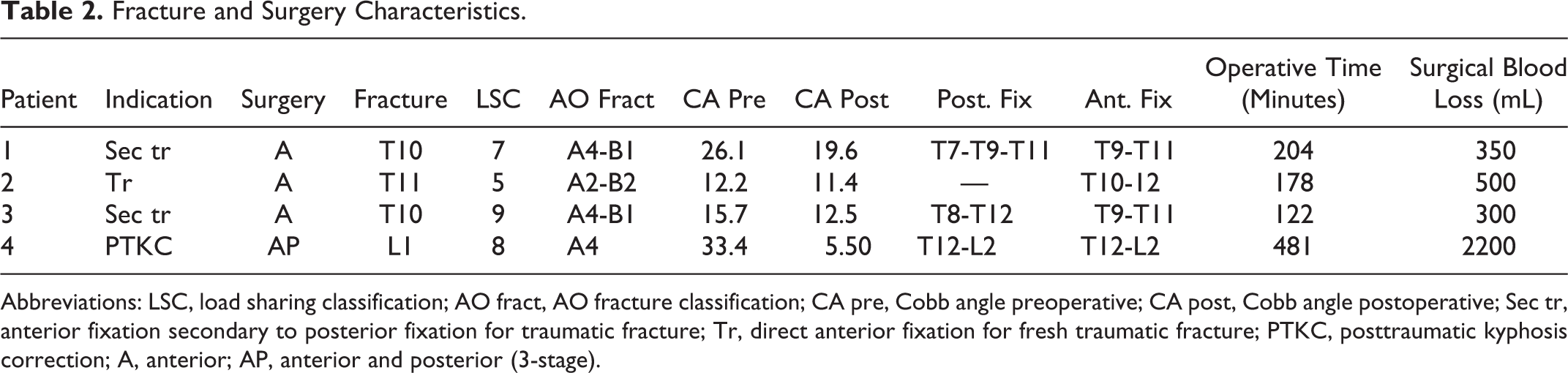
Abbreviations: LSC, load sharing classification; AO fract, AO fracture classification; CA pre, Cobb angle preoperative; CA post, Cobb angle postoperative; Sec tr, anterior fixation secondary to posterior fixation for traumatic fracture; Tr, direct anterior fixation for fresh traumatic fracture; PTKC, posttraumatic kyphosis correction; A, anterior; AP, anterior and posterior (3-stage).
Surgery
All patients underwent anterior 2-segment (one vertebra below and above the fractured vertebra) stabilization. Mean operative time for the 3D standard anterior-only stabilization (patients 1-3; Tables 1 and 2) was 168 ± 42 minutes, which was comparable to the mean of 170 ± 52 minutes for the last 10 patients treated with conventional 2D thoracoscopy. Blood loss was considerably less for 3D thoracoscopy, with a mean of 383 ± 104 mL, compared to a mean of 704 ± 595 mL for conventional thoracoscopy. The 3-staged procedure (posttraumatic kyphosis correction), applied in one patient, took 481 minutes (including repositioning twice) and resulted in 2200 mL blood loss. These results were comparable to previous 3-stage procedures using conventional techniques. The radiographic results of the patients (Figure 2) were comparable to those of patients treated with the conventional technique. No per- or postoperative complications occurred in all patients.
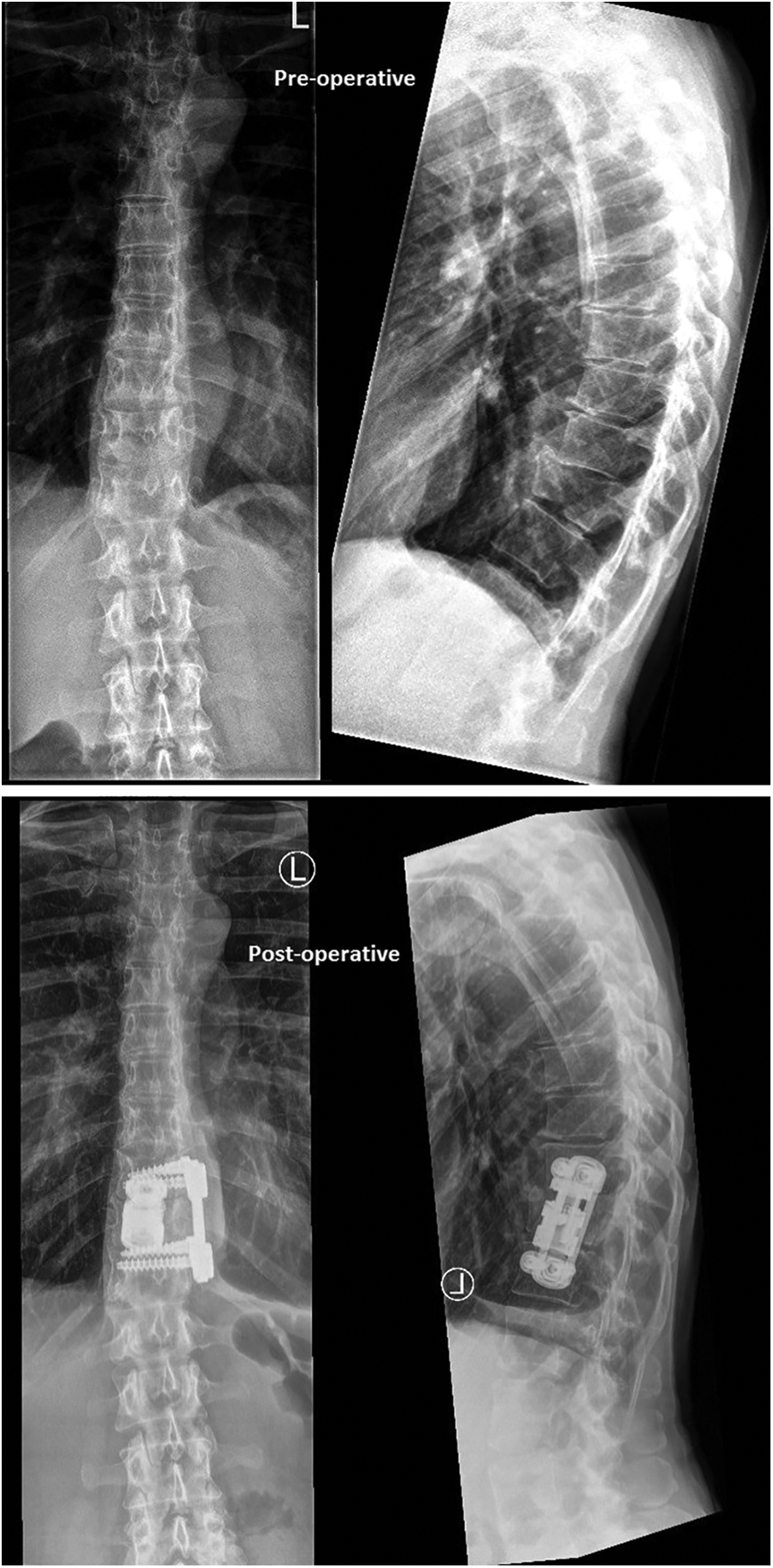
Radiographic result of a patient treated using 3D thoracoscopy, with lateral and anteroposterior X-ray preoperatively and 1 month postoperatively.
Surgeon’s Experience
The treating surgeons (FB and JD) are experienced in the surgical treatment of traumatic spine fractures and very familiar with the thoracoscopic anterior approach as this is the only center in the country where this surgical technique is performed. They were very satisfied with the 3D image quality and stereoscopic views. The 3D view facilitated a fluent surgery process. The main advantage was improved depth estimation compared with 2D thoracoscopy, which especially facilitated identification of vital structures and the partial corpectomy. If one of the cameras of the video portal gets blurred due to, for example, blood spots, and one is looking through the glasses at the monitor, this will only show 2D vison. Cleaning the video portal solves this problem, and this is not different from the 2D thoracoscopy procedure where there is no vision if one lens is blurred.
Residents that participated in the procedures also reported improved depth estimation, which especially aided in connecting instrumentation such as screws, bolts, and plates that have to be attached. Because this procedure is not frequently performed and residents rotate between hospitals, they could not compare 3D thoracoscopy to the conventional 2D technique. Although the residents were not familiar with 3D thoracoscopy nor laparoscopy, no side effects such as nausea, dizziness, or eye strain due to the stereoscopic view occurred.
Discussion
While the use of 3D endoscopy is already implemented and increasingly used for lung surgery 5,10 -12 and abdominal surgery, 3,4 there is no literature on the use of this technique in spine surgery. Studies on 3D thoracoscopy for lung surgery have mainly shown improvement in operative time. 10 -12 The results of and experience with the treatment of our first 4 patients showed benefits of the 3D images over conventional 2D images in spinal surgery. It provided better depth estimation and a safer procedure due to clear visibility of vital structures that surround the surgical area (aorta and segmental vessels, spinal cord, exiting nerve roots). Presumably, this resulted in less blood loss compared with previous operations with conventional 2D thoracoscopy. Blood loss was also less compared to the average blood loss (650 mL) of 150 patients treated in a center with high expertise. 1 It has to be noted though that blood loss is very dependent on individual patient characteristics such as anticoagulative medication, fracture complexity, and anatomic variations.
Based on the first 4 patients we are therefore cautious to draw definitive conclusions on improved blood loss, but the results show potential.
Operative time of the first four 3D procedures was comparable to that of the conventional 2D procedure in this center. However, as reported for 3D-VATS, 3D thoracoscopy for anterior spinal stabilization has the potential to improve operative time, especially due to a faster and more precise corpectomy. Furthermore, residents reported to have better understanding of the surgical procedure, which might enhance a steeper learning curve. While results are promising, definitive conclusions can obviously only be drawn with results of more patients that are treated using this 3D technique. Additionally, the current results have to be interpreted in light of the retrospective design and consequent possible selection bias. We expect that 3D thoracoscopy provides benefits comparable to those of 3D-VATS and 3D laparoscopy. 8,9
In our university hospital center, 3D equipment was already available as being used for lung and abdominal surgery and could directly be used by our spine surgeons to perform a 3D thoracoscopic spine procedure. No additional training for the treating surgeons for 3D compared to 2D was needed. The surgeons had not used 3D thoracoscopy before, which proves that the concept can be easily adapted by surgeons already familiar with the conventional thoracoscopy technique. Higher costs due to the 3D technique are inevitable when using this expensive technique. However, especially in an academic teaching hospital the costs might provide good value because the technique is associated with steeper learning curves. 14,15 Residents might learn faster and perform with less complications. The residents involved in this study had not seen the procedure before but were able to assist successfully. Beside residents, the technique might also be beneficial to junior surgeons not familiar with conventional thoracoscopy, due to improved spatial orientation, which might shorten the learning curve. 14,15 However, this has still to be proven for spine surgery. If future studies demonstrate advantages such as shorter operative times, less blood loss, and possibly less complications, the technique might be worth the additional costs.
Because the incision for the working and video portal are made in direct alignment with the designated vertebra, a rigid (20°) camera is probably sufficient to visualize the work area. However, a flexible camera tip is available if needed, and has its main advantage in providing a complete overview of the working area with its surrounding vital structures.
The described technique is not intended to replace previous techniques such as image-guided navigation 16 but merely to aid in precisely estimating and placing fixation material. Furthermore, 3D thoracoscopy could possibly be combined with image-guided navigation for pedicle screw insertion to have the advantages of both techniques. Other developments might also be combined with 3D thoracoscopy for spine surgery, such as uniportal 3D thoracoscopy to even further minimize surgical damage. 17 -19 In addition, glasses-free 3D thoracoscopy is readily available and provides even more ease of use; however, this comes at a much higher cost.
Conclusion
We have shown feasibility and a positive first experience with 3D thoracoscopy for spine surgery mainly due to improved depth estimation. Experienced thoracoscopic spine surgeons with access to 3D compatible instrumentation can readily experience the advantages of the technique without additional training. Operative and patient-specific advantages such as reduced operative time and blood loss are promising but have to be proven in future studies comparing conventional and 3D thoracoscopy for spine surgery.
Footnotes
Authors’ Note
All authors have made substantial contributions to the concept and design of the study, data analysis, and revision of the article for intellectual content. All authors have fully read and approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.