
Abstract
Study design:
The present study is a prospectively randomized study.
Objective:
The objective of the study was to evaluate the impact of posterior epidural adipose tissue (PAT) on postoperative outcome following lumbar decompression surgery for lumbar spinal stenosis (LSS) by whether PAT was removed or preserved during the surgical procedure.
Summary of background data:
In posterior decompression surgery for LSS, PAT is routinely removed without knowledge of its role and significance. However, considering adipose tissue has regenerative properties of damaged neighboring tissues or itself, PAT, which is adipose tissue located at peridural space, might also have a potential to regenerate the neighboring damaged tissue, including dura and nerve root in the lumbar spine, but this has not been thoroughly studied.
Methods:
Of the 185 eligible patients screened for the current study, 181 patients were enrolled and randomly allocated into either group A (PAT removal, n = 90) or group B (PAT retention, n = 91). The primary outcome measure was pain intensity on the lower back and lower extremity. The secondary outcome measures were functional outcome based on the Oswestry disability index (ODI) and walking distance, complications during the surgical procedure, and surgical outcomes.
Results:
Postoperative pain intensity on the lower back and lower extremity was greater in group A than in group B. Functional status on ODI and walking distance was also worse in group B than in group A (64.9% in group A and 66.2% in group B). The number of patients with aggravated pain intensity and deteriorated functional status in postoperative follow-up times was significantly greater in group A than in group B. There were no significant differences in surgical outcome and complications between the groups.
Conclusion:
Preserving epidural fat may be favorable in postoperative outcomes of posterior decompression surgery for LSS compared to removing epidural fat.
Introduction
Lumbar spinal stenosis (LSS) is typically managed surgically if not improved with proper conservative treatment. 1 The surgical approach for LSS has been posterior in most cases because the stenosis is mainly caused by dural infingement of posterior elements such as the ligamentum flavum (LF) and posterior osteophytes. 2 –4 Posterior decompression for LSS has been routinely performed with laminotomy or partial or total laminectomy according to the patient’s disease status, resection of LF and osteophytes, and removal of posterior epidural adipose tissue (PAT), which leads to sufficient decompression of dura and nerve root. 4
The function and significant of PAT have not been thoroughly studied. PAT is considered a simple space-filling adipose tissue with a semifluid property. 5,6 It is situated in the posterior triangle limited by the lamina, the LF, and the posterior surface of the thecal sac and is covered by a thin membrane of connective tissue. A few of clinical articles stated that PAT removal might be associated with postoperative epidural fibrosis, chronic lower back pain, recurrent radiating pain of the lower extremities, and deterioration of functional status, which has been termed post lumbar surgery syndrome. 7 –13 Consequently, some synthetic biomaterials and autologous materials for replacing PAT after surgical decompression have been introduced for ameliorating the problems related to its removal. 13 –19 However, studies analyzing PAT function are rare. We thought that PAT might have unknown functions beyond those described above. In general, each tissue has inherited features and significance: as such, PAT also may have a specific role. To date, human adipose tissue has been a focus because of its regenerative properties, such as adipose-derived mesenchymal stem cells (ADSCs). 20 Further, some articles have demonstrated that ADSCs have the unique function of regenerating neighboring damaged tissue. 6,20 –24 Based on the knowledge that adipose tissue has an impact on the regeneration of neighboring damaged tissues, PAT may aid in regenerating neighboring damaged dura, nerve root, and peridural connective tissue in the lumbar spine. In particular, PAT’s potential role in regeneration may relate to improve a postoperative outcome and prevent postoperative epidural fibrosis and PLSS, but no studies have addressed these possibilities.
With this knowledge, we initiated experimental and clinical studies focusing on PAT. This is the first report of our studies in which we evaluate the postoperative role of PAT based on whether the PAT was retained or removed during posterior decompression surgery. We hypothesized that PAT removal would be associated with aggravated postoperative pain and deteriorated functional status.
Methods
Participants
This study was approved by the institutional review board of the corresponding author’s hospital and was published in the ClinicalTrials.gov database (NCT02127008). To evaluate the role of PAT, we planned to perform experimental and clinical studies regarding PAT function in January 2012. To prospectively analyze the impact of PAT removal or retention on postoperative outcomes following posterior decompression in lumbar spine, we started the current study in April 2012. All data were collected prospectively and evaluated.
Inclusion criteria were as follows. First, patients had to have LSS as diagnosed using lumbar spine radiographs and magnetic resonance images (MRIs) that corresponded to clinical manifestations and physical examinations. The severity of spinal stenosis was assessed using qualitative measurements performed by an orthopedic spine surgeon (LGW), according to the general guideline (Suri) classification. 25 According to the classification, LSS was divided into four levels (grade 0, no narrowing; grade 1, mild: narrowing of less than one-third of the normal area; grade 2, moderate: narrowing of one-third to two-thirds of the normal area; and grade 3, severe: narrowing of greater than two-thirds of the normal area). Second, patients had to show no improvement in clinical symptoms despite several conservative treatments (including medication, physical therapy, and injection treatment) over a period of 6 months or more. Third, patients had to have undergone posterior decompression in the lumbar spine. Fourth, patients had to be between 40 years and 60 years of age. Fifth, patients had to have volunteered for this study and provided written consent. Finally, patients had to undergo at least 1 year of follow-up.
Exclusion criteria were as follows: fractures, infection, or tumors in the lumbar spine; previous surgery in the lumbar spine; other stenotic pathologies such as achondroplasia; hemorrhagic disorders such as hemophilia and thrombocythemia; follow-up period less than 1 year; patient inability to accurately record results of preoperative and postoperative questionnaires due to problems such as a history of stroke or dementia; and patient lack-of-suitability for this study, as judged by the corresponding author.
Sample size estimation and randomization
The sample size calculation for this trial was performed with a non-inferiority design as a pilot study due to the lack of competing articles regarding PAT. Taking a significant level of 10% as the non-inferiority margin, and successful outcome of 91%, 2 a type 1 error of 2.5%, a power of 80%, and a dropout rate of 10%, with 90 patients in each group were required (Figure 1).

Flow diagram of patient enrollment.
Patients were randomly assigned into group A for which PAT was removed or group B for which PAT was not removed. Randomization was conducted by a computer-generated allocation program (nQquery Advisor® PPS 6.01, Saugus, Massachusetts, USA), which assigns numbers in strict chronological sequences and enters regular sequences for each study group. Randomization was stratified via three variables: (1) age (40s vs. 50s), (2) smoking status (smoker vs. nonsmoker), and (3) surgical level (L4–L5 vs. L5–S1). Each study participant was allocated a unique randomization number upon screening completion (Figure 1).
Surgical procedure and postoperative protocol
All surgeries were performed by a single orthopedic surgeon who used the same operative technique in every case. After a midline skin incision at the affected level, bilateral paraspinal musculature was detached from the posterior bony arch with no violation of the facet joint. Posterior decompression with partial laminectomy was routinely performed using a burr and Kerrison rongeur. LF was exposed and excised carefully with no violation of PAT using the Kerrison rongeur. To avoid loss of PAT during decompressive procedure, we always performed the following surgical steps. First, we osteotomized upper and lower lamina with surgical osteotome for laminotomy or partial laminectomy. Next, LF was detached from bony structures using curve-shaped curette. Finally, en bloc resection of L4 and L5 laminotomy site including LF would be done, without the use of a Kerrison punch. According to the patient’s allocated group, PAT was removed or retained (Figure 2). Additional procedures, such as foraminotomy, were performed when necessary. After the decompressive procedure, saline irrigation was routinely performed. Especially in patients with retained PAT (group B), irrigation was performed after placing gauze on the PAT to prevent the tissue from being washed out.

Intraoperative photographs at both groups. (a) In group A, PAT was removed during posterior decompression surgery. (b) In group B, PAT was retained during posterior decompression surgery.
Patients in both groups were admitted to the same wards following the operation and treated with the same postoperative protocols. All patients were allowed to ambulate the first day after surgery, and the majority of patients were discharged from the hospital on the third postoperative day. Patients were not permitted to sit for long periods of time during the first month after surgery. After three postsurgical months, patients were allowed to resume normal activities, including heavy lifting.
Outcome measures
The primary postsurgical study end point was pain intensity. Pain intensity was recorded using a visual analog scale (VAS) and evaluated separately for the two regions of the low back and lower extremity. Patients were instructed to make a mark on a horizontally oriented, 10-point VAS which was labeled “no pain” at the far left and “greatest pain” at the far right. Patients were not allowed to review their previous scores.
There were several secondary end points, including functional status based on the Oswestry disability index (ODI) and walking distance, surgical outcome based on surgical time, estimated blood loss, hospital stay, complications during the procedure such as dural tear, and additional outcomes including infection rate. These data were collected prospectively by a research coordinator, both preoperatively and at each of a series of regular follow-up visits. The questionnaires, chart data, and clinical records were analyzed by one surgeon who was not otherwise involved in this study.
Statistical analysis
The independent Student’s t-test or the analysis of variance test was used for continuous variables. SPSS software version 19.0 (SPSS, Chicago, Illinois, USA) was used for all analyses, and a two-sided p value <0.05 was considered statistically significant.
Results
Population
One hundred eighty-five eligible patients were screened for the current study, but four patients were excluded for several reasons. A total of 181 patients were enrolled and randomly assigned to either group A (PAT removal, 90 patients) or group B (PAT retention, 91 patients), all of whom fully complied with the inclusion and exclusion criteria (Figure 1). No patient was lost to follow-up. Patients were similar between groups with respect to demographic characteristics such as age, gender, smoking status, LSS severity, height, weight, and BMI (Table 1). The decompression level was also similar between the two groups (Table 2).
Demographic data.a
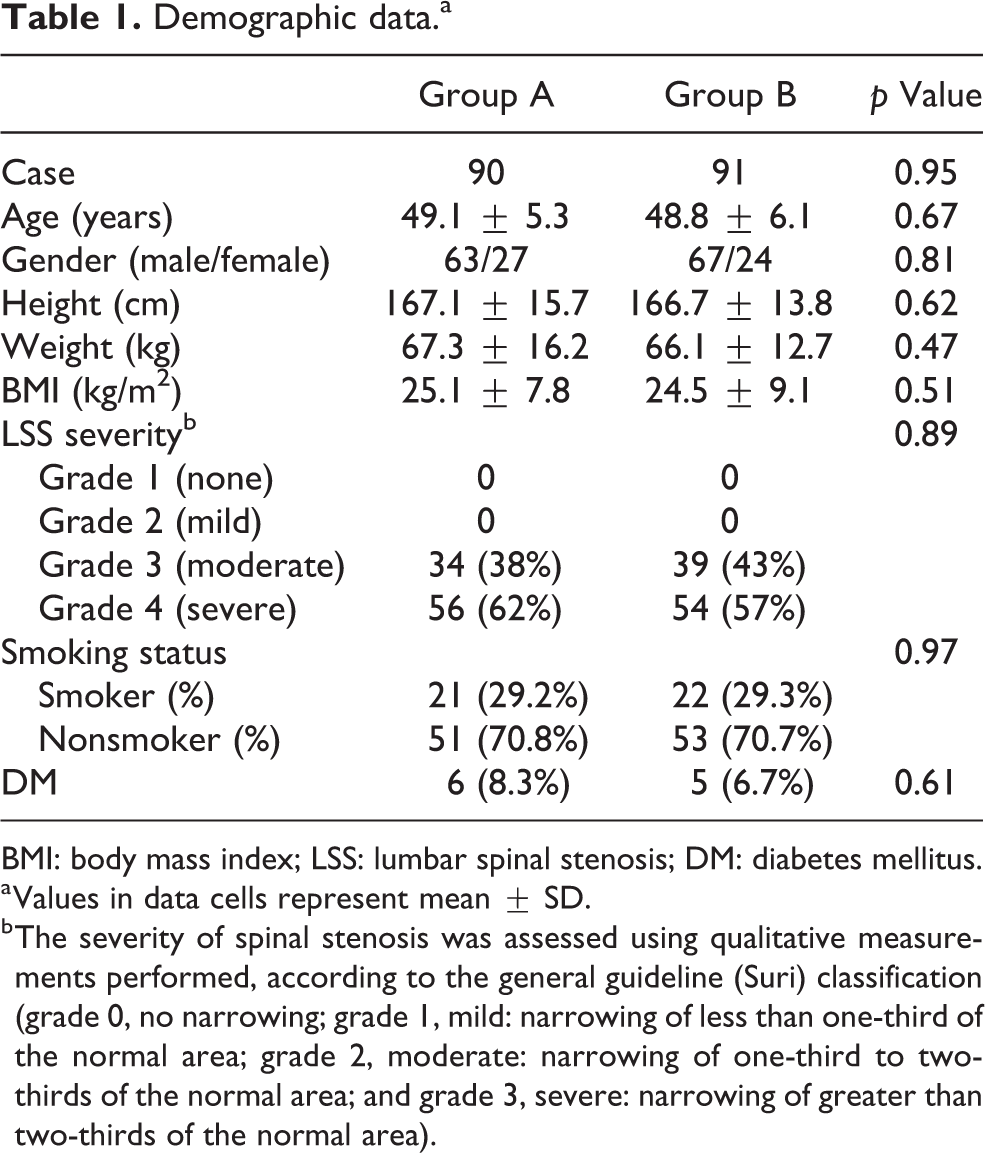
BMI: body mass index; LSS: lumbar spinal stenosis; DM: diabetes mellitus.
a Values in data cells represent mean ± SD.
b The severity of spinal stenosis was assessed using qualitative measurements performed, according to the general guideline (Suri) classification (grade 0, no narrowing; grade 1, mild: narrowing of less than one-third of the normal area; grade 2, moderate: narrowing of one-third to two-thirds of the normal area; and grade 3, severe: narrowing of greater than two-thirds of the normal area).
Decompression level.a

a Values in data cells represent number of cases (%).
Primary outcome measure (pain intensity)
Mean VAS scores for lower back pain indicated that 1-year postoperative pain level was significantly lower than preoperative level for both groups, with mean scores decreasing from 8.3 ± 2.3 preoperatively to 1.8 ± 1.3 at postoperative 1 year in group A and from 8.5 ± 2.5 to 1.5 ± 0.8 in group B; the improvement was greater in group B than group A, with a significant difference between the groups (p = 0.05) (Table 3). VAS scores for radiating pain also improved significantly in both groups, with mean scores decreasing from 5.7 ± 1.1 preoperatively to 1.9 ± 1.1 at postoperative 1 year in group A and from 5.2 ± 1.3 to 1.4 ± 0.9 in group B; the improvement was also greater in group B than group A, although there was no significant difference between the groups (p = 0.08) (Table 3). And, the numbers of patients with significantly aggravated pain intensity in the lower back and lower extremities during postoperative follow-up were significantly different in the two groups; there were 11 of 90 (12.2%) and 6 of 91 (6.6%) with aggravated pain in groups A and B, respectively (p = 0.02).
Primary end points (pain intensity).
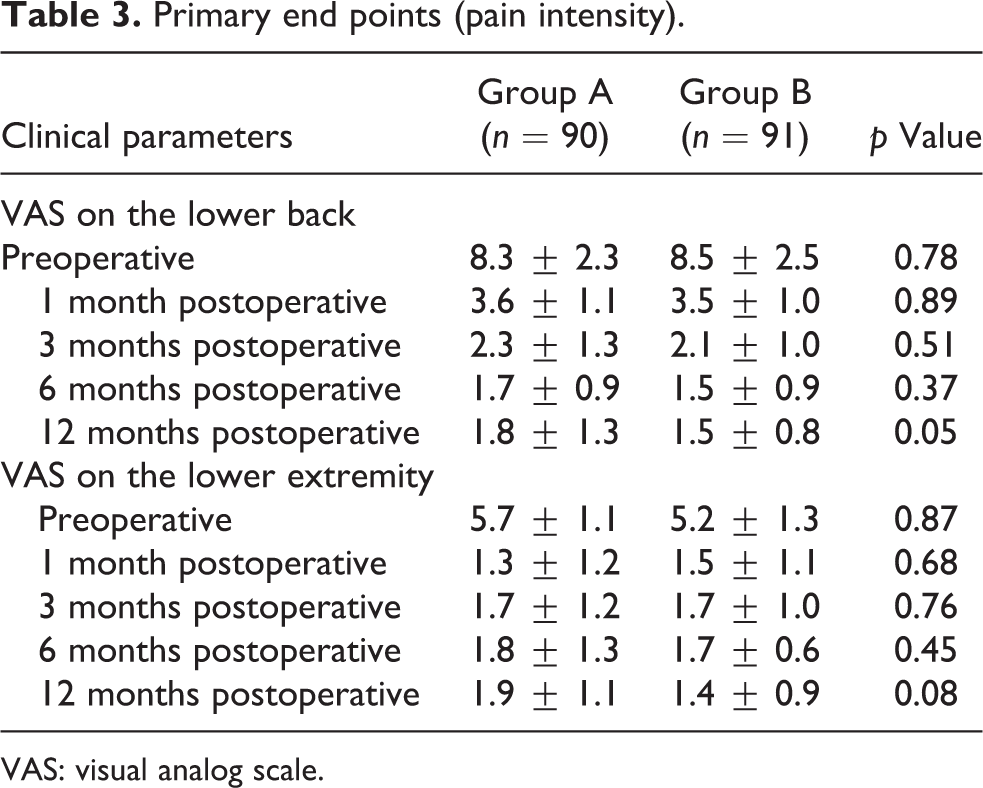
VAS: visual analog scale.
Secondary outcome measures
Mean ODI score also improved from 43.6 ± 11.3 preoperatively to 15.3 ± 9.1 at 1 year after surgery in group A and from 42.3 ± 10.7 preoperatively to 14.3 ± 7.8 at 1 year after surgery in group B; there was no statistically significant difference between the groups (p = 0.25) (Table 4). However, the number of patients with a remarkably deteriorated functional score during postoperative follow-up was significantly different; there were 14 of 90 (15.6%) and 7 of 91 (7.7%) such patients in groups A and B, respectively (p = 0.04).
Secondary end points.
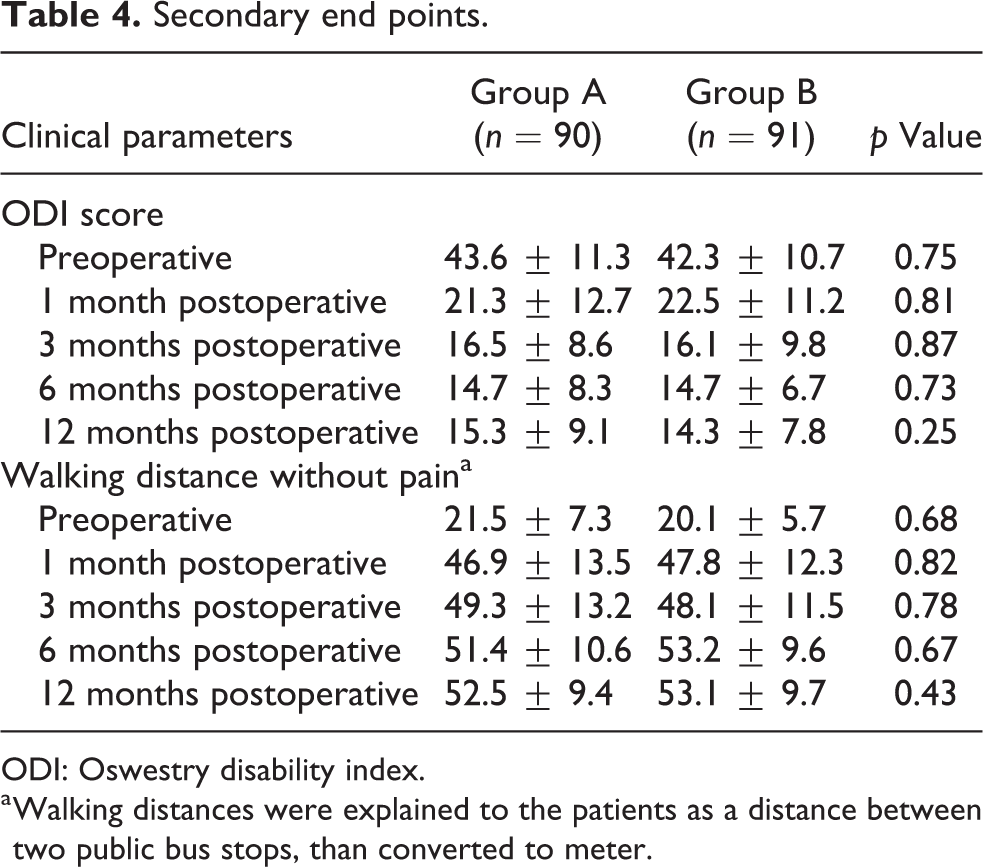
ODI: Oswestry disability index.
a Walking distances were explained to the patients as a distance between two public bus stops, than converted to meter.
The outcome of walking distance was also similar in both groups: the distance was improved from 21.5 ± 7.3 m preoperatively to 52.5 ± 9.4 m at 1 year after surgery in group A and from 20.1 ± 5.7 m preoperatively to 53.1 ± 9.7 m at 1 year after surgery in group B. There was no statistically significant difference between the groups (p = 0.43) (Table 4).
In surgery, one patient in group B had a dural tear during posterior decompression with PAT removal. The torn dura was repaired using 4-0 silk suture, and it was confirmed that there was no cerebrospinal fluid leakage using intraoperative Valsalva maneuver after dural repair. The patient had no neurological symptom related to dural tear. No other complication occurred during the procedure in any patient in either group.
Surgical outcomes, including estimated blood loss, operation time, hospital stay, and incision length, are described in Table 5, and there was no significant difference between the groups. There were also no complications such as fever, swelling, or deep infection for any patient during the follow-up period; however, there was one patient in group B with a sign of local superficial infection at the surgical site. The infection sign was resolved with antibiotics (intravenous third-generation cephalosporin and oral gentamycin) and did not require an additional procedure such as debridement.
Surgical outcome.a
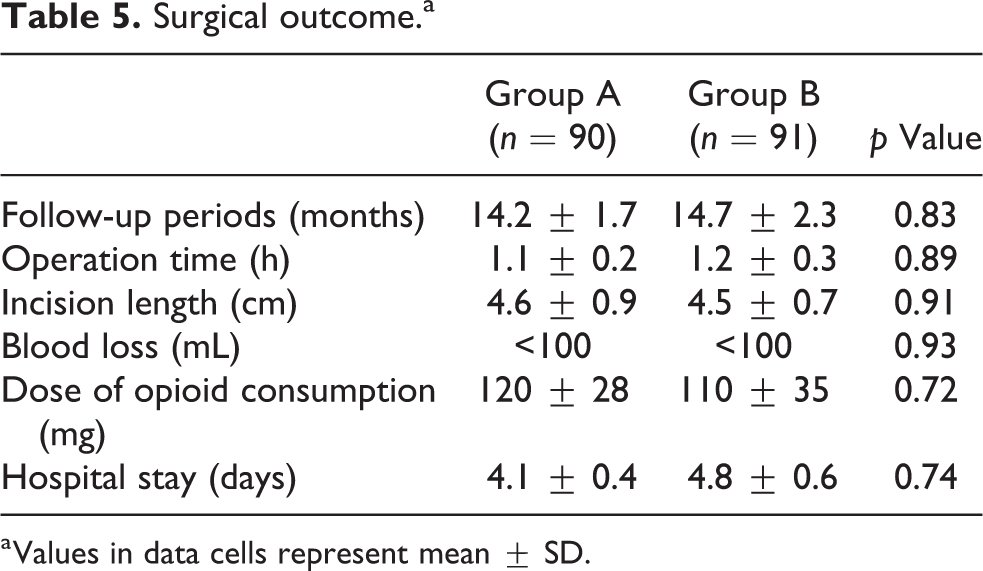
a Values in data cells represent mean ± SD.
Discussion
LSS is associated with aging and has an incidence of approximately 50% or more in populations older than 60 years. 2,5 Most LSS can be managed conservatively with medication, physical therapy, and injections. 4 However, some eventually require surgical management despite proper conservative treatment. The surgical approach is almost always posterior because most compressing lesions, such as LF and osteophytes, are located behind the dura and nerve root, and critical obstacles, such as huge vessels and intra-abdominal organs, can be confronted during an anterior procedure. During posterior decompression surgery for LSS the following items were routinely removed: some part of the lamina, LF, and affected PAT.
Actually, except in rare cases, such as spinal epidural lipomatosis, PAT does not serve as a compression lesion to cause symptoms of lower back and radiating pain in the lower extremities. However, because PAT’s role and significance have not been defined fully and surgeons feel self-satisfaction in obtaining sufficient decompression through directly visualizing the dura by removing PAT, PAT has been recognized as a removable element during decompression. In general, each tissue has inherited features and function. Therefore, PAT also may have specific functions as yet unknown. Adipose tissue recently has been a focus because of its inherited regenerative properties: ADSC cultured from abdominal or eyelid adipose tissue has a self-renewal property, as well as regenerate damaged or malfunctioning neighboring tissues, such as extracellular matrix, insulin-secreting pancreatic β-cells, bone-forming cells, and neuron-like cells. 20 –24 In addition, studies regarding the role of ADSC in neurodegenerative disorders and acute cord or peripheral nerve injury have been widely conducted. 21,22,24 However, widely utilized ADSC at present are cultured mostly from abdominal or eyelid adipose tissue because of easy harvest and collection at these sites. 20 Based on the knowledge that adipose tissue has an impact on the regeneration of neighboring damaged tissues, damaged or malfunctioning dura or nerve roots in the lumbar spine may be regenerated by ADSC of nearby adipose tissue such as PAT. Although PAT is among the neighboring adipose tissues that may be participating in regeneration, studies using ADSC collected from PAT have not been reported.
It has not been thoroughly evaluated why PAT exists in the epidural space. Only a few articles have reported on PAT’s anatomical and histological features, identifying that it was a simple space-filling tissue with a semi-fluid property and that is covered by a thin membrane. 5,6 Some articles have stated that PAT might be associated with postoperative epidural fibrosis and PLSS: as such, some synthetic or autologous biomaterials for replacing PAT were introduced. 9,11 –14,16 –19 We posited that PAT should be retained during surgical procedures if it has specific functions for regenerating damaged nerve tissue and peridural connective tissue occurring during surgical procedure, it should be remained during surgery. These were the motivations for the current study.
In reviewing the literature, we could not find any report on PAT’s role during decompression or in postoperative outcome. Therefore, we evaluated PAT’s role in postoperative pain, functional status, and complications after posterior decompression surgery for LSS by comparing patients with PAT removal with patients with PAT retention in a prospective randomized study design. The pain intensity, which was primary end point, was significantly different between the two groups. For example, the pain intensity in the lower back at postoperative 1 year was 1.8 ± 1.3 in group A (with a removal of PAT) and 1.5 ± 0.8 in group B (with a retention of PAT) (p = 0.05), and pain intensity in the lower extremities at postoperative 1 year was 1.9 ± 1.1 and 1.4 ± 0.9 in groups A and B, respectively (p = 0.08). Surprisingly, however, the number of patients with aggravated pain intensity during postoperative follow-up was significantly greater in group A (11 of 90, 12.2%) than in group B (6 of 91, 6.6%) (p = 0.02). Functional status by ODI showed similarities with pain intensity; there was no significant difference between the groups with regard to improvement in functional outcome (64.9% in group A and 66.2% in group B, p = 0.61). However, as of back pain aggravation, the number of patients with deteriorated functional status during postoperative follow-up was significantly greater in group A (14 of 90, 15.6) than in group B (7 of 91, 7.7%) (p = 0.02). In addition, some patients (three in group A and one in group B) with no aggravated pain intensity demonstrated deteriorated functional outcomes. These patients experienced unexplained discomfort, as dissimilar with pain, which we thought it was caused by postoperative epidural fibrosis and tethered dura and nerve root. Based on the outcomes from the study, we suggested that retention of PAT during surgery may be associated with greater postoperative clinical outcomes, especially for back pain and functional state, than its removal.
As mentioned earlier, we have performed several studies to evaluate the role and significance of PAT using multidirectional approaches. Fundamentally, we performed an experimental study for confirming the presence of mesenchymal stem cell (MSC) from epidural fat. From an experimental study, we found the existence of MSC within the epidural fat, and we called that as EF-MSC, the outcome of which was published at an international peer-reviewed journal. 26 Moreover, we confirmed that EF-MSC differed markedly from MSC from other fat tissues, in terms of cell isolation and proliferation, characterization, differentiation potential, and especially expression of neuronal markers and neurogenic differentiation, results of which will be presented soon.
The current study had some limitations. First, it was a prospective comparative study with a relatively small sample size and short follow-up period. To better establish the role of PAT in treatment outcome for LSS patients, more studies should be performed that use a larger sample size, an extended follow-up period, and a prospective study design. Second, this study was conducted with patients who had received posterior decompression only. In other words, results from this study cannot be applied to subjects in other situations, including lumbar fusion surgery or involvement of other spinal segments. Additional studies regarding these conditions are needed. Third, we did not explore MRI findings at 1 year after surgery to compare imaging studies for detecting conditions such as epidural fibrosis. MRI may aid in the detection of postoperative epidural fibrosis, but some articles have demonstrated that it has a relatively lower detection rate, approximately 10–15% of postoperative epidural fibrosis and is time-consuming and involves radiation exposure. Additional studies to compare the presence of epidural fibrosis in postoperative MRI and physical examination are necessary.
Despite these limitations, the current study has some unique strengths. First, this is the first study to focus on the role and significance of PAT in postoperative outcomes of lumbar decompression surgery. Overall, due to the lack of competing articles regarding PAT, this study can be considered a cornerstone for further research on PAT. Study results included 181 patients who underwent decompression surgery for LSS and remained for follow-up. Because our hospital is an armed forces hospital, regular follow-up visits were possible for all enrolled patients. In addition, the data in the current study were obtained from a homogenous population with respect to age, gender, and sports and physical activity, based on the population of the armed forces hospital. Specifically, by randomized allocation into each group, all patients were 40–60 years old and had a similar proportion of gender between groups and similar degrees of physical activity. Such population homogeneity reduces the risk of confounding factors on outcome variables.
Conclusion
This is the first report to evaluate PAT’s role through PAT removal or retention during posterior decompression surgery in the lumbar spine, with 1-year follow-up and a prospectively randomized controlled design. There was a significant difference between groups in terms of pain improvement in the lower back, which was the primary end point, and the number of patients with aggravated pain in the postoperative follow-up period was significantly greater in group A (with a removal of PAT) than in group B (with a retention of PAT). In addition, functional status based on ODI score was also worse in group A than in group B, and the number of patients with an aggravated functional outcome was significantly greater in group A than in group B. There were no significant differences in other secondary endpoints such as surgical outcome and complications. Based on the results, preserving epidural fat may be favorable in postoperative outcomes of posterior decompression surgery for LSS compared to removing epidural fat.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by 2018 Yeungnam University Research Grant. The funder had no role in the study design, data collection and analysis, and study progression. This study was also approved by the Institutional Review Board (IRB) of Yeungnam University Medical Center.