
Abstract
Objective
To investigate the clinical efficacy of selective versus dual-segment fusion in the treatment of bi-segmental lumbar spinal stenosis with segmental instability using spinal endoscopy.
Methods
A retrospective analysis was conducted on 49 patients with bi-segmental degenerative lumbar disease who underwent endoscopic spinal surgery at our institution between October 2022 and June 2025. In the selective fusion group (n = 27), fusion was performed on the unstable segment and decompression was performed on the other segment. Both segments underwent fusion in the dual-segment fusion group (n = 22). Surgical time, intraoperative blood loss, hospital stay, Visual Analog Scale (VAS) score, Oswestry Disability Index (ODI) fusion rate, and functional improvement were compared.
Results
The selective fusion group had a significantly shorter operative time and lesser blood loss than the dual-fusion group (p < 0.05). Postoperative hospital stay did not differ significantly between groups. Both groups demonstrated significant postoperative improvements in VAS and ODI scores (p < 0.001), with no intergroup differences. At 12 months, Bridwell Grade I–II fusion rates were comparable between the two groups (93.3% vs 90.9%, p > 0.05). The fusion rates and functional outcomes were comparable.
Conclusion
In patients with bi-segmental lumbar stenosis and single-segment instability, Selective fusion under endoscopic guidance provides comparable clinical and radiological outcomes to dual-segment fusion, with reduced operative trauma and faster recovery. This minimally invasive strategy effectively balances surgical stability with functional preservation and warrants broader clinical application.
Keywords
Introduction
With the acceleration of population aging, the incidence of degenerative lumbar spine diseases is increasing annually, making it one of the most common conditions that adversely affects the quality of life in middle-aged and elderly populations. 1 Traditional treatment often involves multilevel decompression and fusion surgery in patients with multilevel lumbar spinal stenoses. Although this technique has proven effective in relieving neural compression symptoms, it is also associated with an extended operative time, increased intraoperative blood loss, accelerated adjacent segment degeneration, and prolonged postoperative recovery.2,3
In recent years, with the advancement of minimally invasive concepts and endoscopic technology, endoscopic lumbar decompression has gained widespread clinical application owing to its advantages of reduced surgical trauma and faster recovery.4,5 However, whether decompression and fusion should be performed at all stenotic levels in patients with multilevel degenerative lumbar spinal stenosis remains controversial. Some studies have advocated fusion at all stenotic levels to prevent postoperative instability and the need for revision surgery. 6 In contrast, other studies suggest that fusing non-unstable segments may unnecessarily increase surgical trauma, delay recovery, and potentially lead to accelerated adjacent segment degeneration or functional loss at fused levels.7,8 Therefore, the concept of selective fusion—fusing only dynamically or structurally unstable segments while preserving motion and performing decompression alone at stable stenotic segments—has become a focal point of recent research and debate.
This study aimed to compare the clinical efficacy and complication rates of selective fusion (fusion of only the unstable segment with decompression of the remaining segment) versus full-segment fusion under endoscopic spine surgery. This study aimed to explore the feasibility of reducing surgical burden while maintaining clinical outcomes, and to provide a more optimized and individualized surgical strategy for multilevel lumbar disease.
Materials and methods
Patients and grouping
This single-center retrospective-controlled study was conducted at the Minimally Invasive Spine Center of Yichang Central People’s Hospital in Hubei Province, China. A total of 49 patients with degenerative lumbar spine disease who underwent endoscopic spinal surgery between October 2022 and June 2025 were included.
All enrolled patients underwent preoperative imaging evaluations including magnetic resonance imaging (MRI), computed tomography (CT), and dynamic X-ray imaging involving two segments. Both stenotic segments were consistent with the patients’ clinical symptoms and neurological signs and were determined to be the pathological levels requiring surgical intervention.
Each case had one segment with clear instability (e.g., spondylolisthesis or hypermobility) treated with endoscopic fusion. The other stenotic but stable segment was treated with either fusion or decompression depending on the preoperative assessment and patient preference, dividing patients into the Selective Fusion Group (n = 27): fusion of the unstable segment and decompression of the stable segment.
Dual-Segment Fusion Group (n = 22): fusion of both segments.
Segmental instability was defined as >3 mm of sagittal translation or >10° of angular motion between flexion and extension on dynamic lateral radiographs. Segments showing only Grade I–II spondylolisthesis without abnormal motion were considered radiographically stable.
Inclusion and exclusion criteria
The inclusion criteria were (1) stenosis in two segments with clinical symptoms, (2) instability in only one segment, (3) ineffective conservative treatment, and (4) complete imaging data.
The exclusion criteria were as follows: (1) one or more of the following: (2) severe spondylolisthesis (Grade III/IV); (3) tumors, infections, or fractures; (4) severe comorbidities; and (5) inability to complete follow-up.
Sample size consideration
This was a retrospective study; therefore, no prior sample size calculation was performed. All consecutive eligible patients during the study period (n = 49) were included to minimize selection bias.
Surgical procedures
All surgeries were performed under general anesthesia using a posterior endoscopic approach. In the selective fusion group, only the unstable segment was fused, whereas in the dual-segment fusion group, both levels underwent fusion. The procedures were conducted using the
Surgical procedure details
Selective fusion group procedure (Figure 1, L4/5 fusion + L5/S1 decompression)
Under general anesthesia, the patient was placed in the prone position. C-arm fluoroscopy was performed to localize the responsible segment. A 1.2 cm longitudinal incision was made at the lateral border of the L4/5 pedicle on the affected side. After stepwise dilation, the endoscopic working channel was established and the target disc space was confirmed under direct vision. A trephine, pituitary rongeur, and high-speed burr were used to remove part of the L4 inferior articular process and L5 superior articular process, followed by resection of the hypertrophic ligamentum flavum to expose and decompress the L5 nerve root. The dura and nerve roots were verified to be free of compression. Transforaminal endoscopic lumbar interbody fusion combined with posterior endoscopic lumbar decompression. (a): Sagittal MRI showing L4/5 and L5/S1 disc herniation with spinal canal stenosis. (b): Axial MRI at the L4/5 level showing a left paracentral disc protrusion causing ipsilateral central canal and left lateral recess stenosis, with nerve root compression and displacement. (c): Axial MRI at the L5/S1 level demonstrating significant narrowing of the left lateral recess. (d): Dynamic lateral X-ray showing >3 mm translation at L4/5 during flexion-extension, indicating dynamic instability; L5/S1 is stable. (e): Axial CT at L4/5 showing posterior disc protrusion compressing the anterior dural sac. (f): Axial CT at L5/S1 showing bony narrowing of the left lateral recess, with facet hypertrophy and ligamentum flavum thickening narrowing the nerve root canal. (g): Preoperative surface marking schematic showing incisions at the lateral edge of the L4/5 pedicle and paramedian site at L5/S1. (h): Intraoperative endoscopic view after L4/5 decompression, with a centrally placed interbody cage and adequate decompression achieved. (i): Intraoperative endoscopic view showing decompressed and relaxed S1 nerve root after L5/S1 decompression. (j): Postoperative CT at L4/5 showing adequate decompression, ideal cage positioning, and widened spinal canal and lateral recess. (k): Postoperative CT at L5/S1 showing complete decompression and significantly expanded left lateral recess with no nerve root compression. (l): Postoperative AP and lateral lumbar X-rays showing good screw placement, maintained disc height at L4/5, and normal alignment at L5/S1.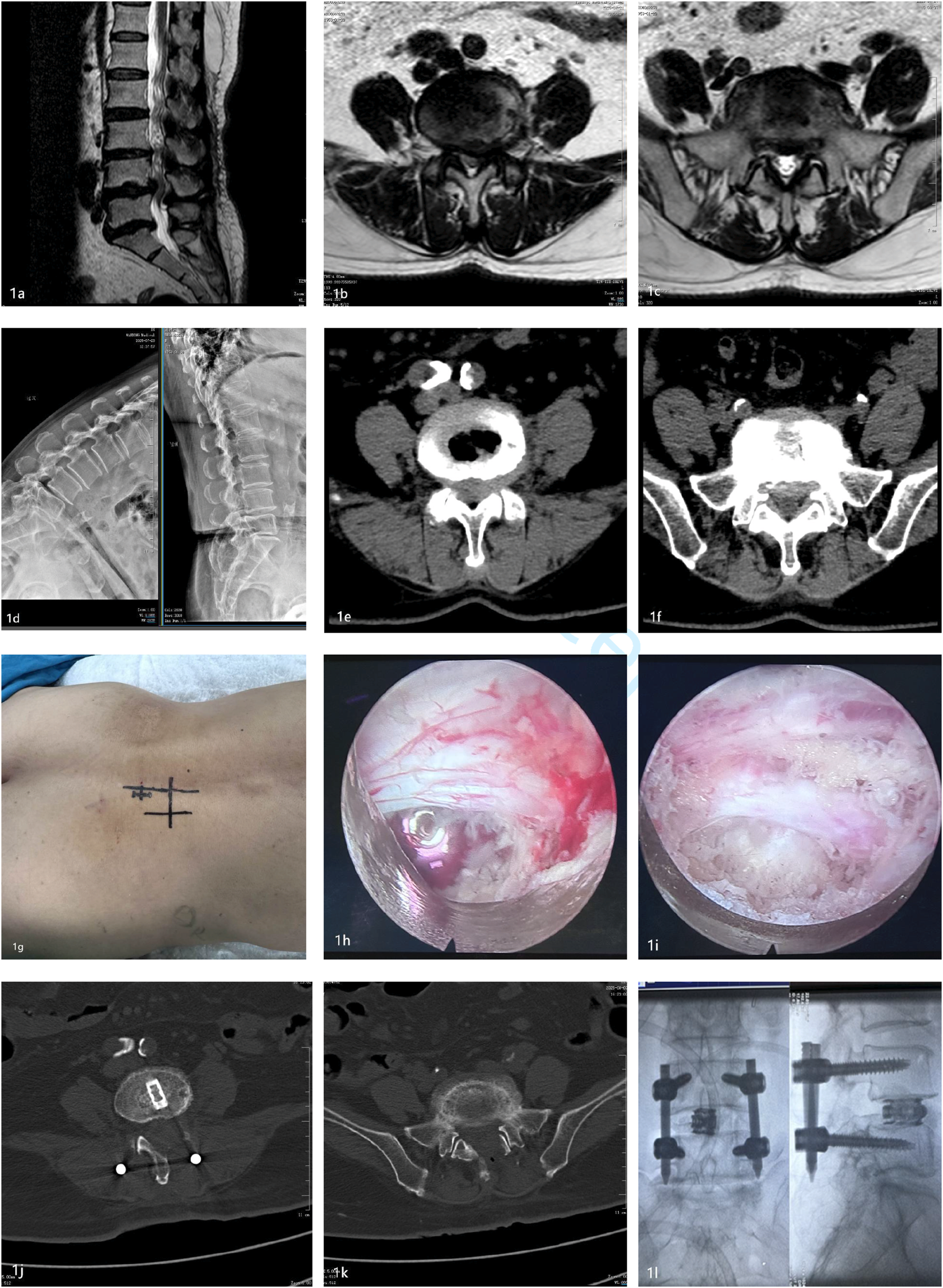
The degenerated nucleus pulposus was removed and the cartilaginous endplate was curetted until bleeding of the subchondral bone was exposed. An autologous bone graft was inserted, followed by the implantation of an expandable cage to restore the disc height. The cage position and nerve root relaxation were confirmed, and no active bleeding was observed. A drainage tube was then placed.
Next, a second 1.2 cm longitudinal incision was made adjacent to the spinous process on the symptomatic side at L5/S1. After dilation and establishment of the endoscopic channel, a portion of the L5 inferior articular process was removed using a pituitary rongeur and a burr. The hypertrophic ligamentum flavum was resected to expose and decompress the S1 nerve root. After confirming adequate decompression, a drain was placed and the incision was closed.
Finally, bilateral L4 and L5 pedicle screws were percutaneously inserted under fluoroscopic guidance and a connecting rod was placed. The correct positioning of the implants was confirmed prior to closure.
Dual-segment fusion group procedure (L4/5 + L5/S1 fusion)
Under general anesthesia, the patient was positioned prone. Levels were confirmed using fluoroscopy. Sequential endoscopic channels were established at L4/5 and L5/S1 on the symptomatic side. According to the standard endoscopic lumbar fusion procedures, decompression, endplate preparation, and cage insertion were performed at both levels. An autologous bone graft was used, and expandable cages were inserted to restore disc height.
Under fluoroscopic guidance, percutaneous pedicle screws were inserted at L4, L5, and S1 followed by rod placement and fixation. Drains were placed and the incisions were closed.
Postoperative care
Postoperatively, the patients were monitored for neurological function, pain relief, and drainage volume. Antibiotics were given for 24–48 h. Drainage was removed when the volume was <50 mL. Imaging findings were reviewed on postoperative days 3–5. The patients began mobilization with brace assistance and were discharged if no complications occurred.
Outcome measures
Surgical parameters
The following perioperative data were recorded: operative time, estimated intraoperative blood loss (PBV), and postoperative length of hospital stay. Intraoperative blood loss (PBV) was calculated using the hematocrit dilution method proposed by Gross in 1983
9
:

Clinical outcome evaluation
The visual analog scale (VAS)
Oswestry disability index (ODI)
Functional status was assessed preoperatively and at 1, 3, and 6 months postoperatively.
MacNab criteria
Used to assess patient satisfaction at 3 and 6 months postoperatively.
Bridwell interbody fusion grading system 11
Used to evaluate the spinal fusion status at 1, 3, and 12 months postoperatively.
Statistical analysis
Statistical analyses were performed using
Results
Baseline characteristics
There were no significant differences between the two groups regarding sex, age, height, or weight (P > 0.05), ensuring comparability.
The severity of lumbar spinal canal stenosis in the stable segment was evaluated using the four-grade qualitative MRI classification system proposed by Lee et al. 12 in 2011. This system is applicable for assessing the degree of central canal and lateral recess stenosis based on the extent of cerebrospinal fluid (CSF) space obliteration observed on axial T2-weighted images.
Preoperatively, in the selective fusion group, lateral recess stenosis was Grade I in 6 cases, Grade II in 16 cases, and Grade III in 5 cases; in the dual-segment fusion group, it was Grade I in 9 cases, Grade II in 10 cases, and Grade III in 3 cases. The distribution of stenosis severity in the stable segment was comparable between the two groups. Statistical analysis using the Fisher’s exact test (Fisher–Freeman–Halton extension) showed no significant difference (p = 0.436), indicating that the two groups were comparable in baseline radiological severity.
Quantitative postoperative assessment using the Lee grading system was not performed because local edema and scar formation at the surgical site could interfere with the accuracy of early postoperative evaluation.
Surgical parameters
Surgical parameters.

Clinical outcomes
At the time of analysis, some patients had not yet reached the 6- or 12-months follow-up, resulting in reduced case numbers at later follow-ups.
VAS and ODI scores pre- and post-operatively.
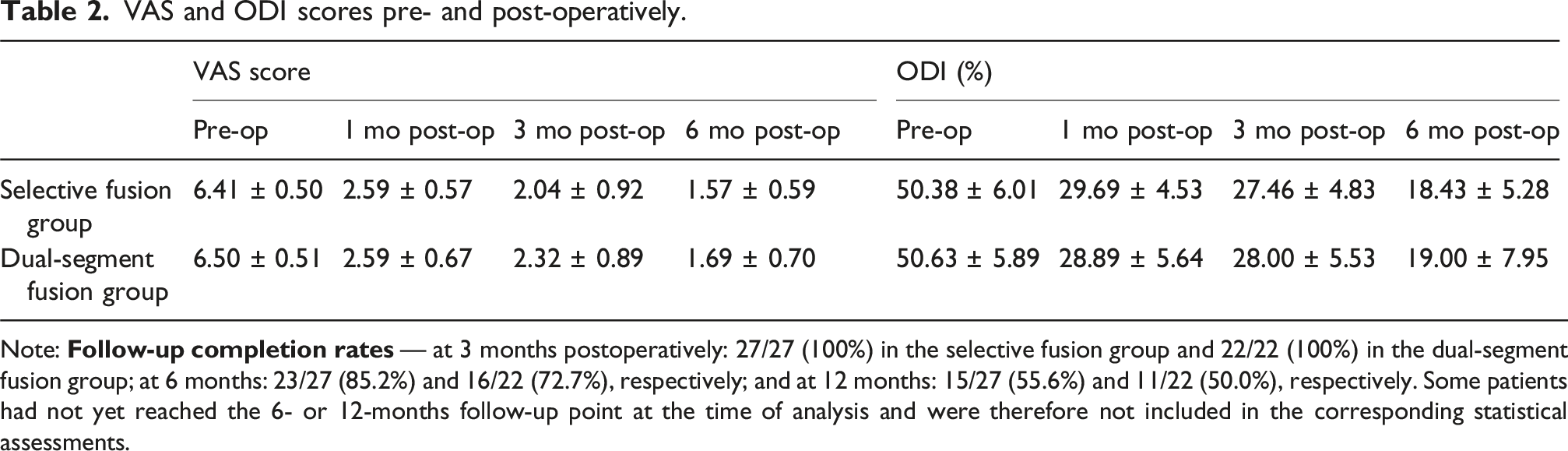
Note:
Distribution of fusion grades and functional outcomes
At 3 months postoperatively, the excellent-to-good rate according to the MacNab criteria was 96.3% (26/27) in the selective fusion group and 90.9% (20/22) in the dual-segment fusion group, with no statistically significant difference between the two groups (p = 0.581). At 6 months postoperatively, the excellent-to-good rates were 91.3% (21/23) and 87.5% (14/16), respectively, also showing no significant difference (p = 0.72). These findings indicate that both surgical strategies achieve comparable short- and mid-term clinical satisfaction.
Bridwell fusion grades and MacNab criteria.

Complications and degeneration
Postoperative complications and degeneration.

Discussion
The results of this study demonstrated that in patients with bi-segmental lumbar spinal stenosis combined with single-segment instability, the selective fusion group exhibited significantly better surgical parameters, such as reduced operative time and less blood loss, compared to the dual-segment fusion group. However, there were no statistically significant differences in the postoperative VAS scores, ODI indices, or fusion rates between the groups. These findings suggest that selective fusion can achieve comparable clinical efficacy while minimizing surgical trauma and enhancing recovery efficiency, which is consistent with previously published reports. 13
Although the overall complication rates were not significantly different between the two groups, selective fusion offers several distinct advantages. By preserving the stable motion segment, this technique minimizes unnecessary instrumentation, reduces muscle and ligament disruption, and helps maintain physiological lumbar mobility. These biomechanical benefits may contribute to lowering the risk of long-term adjacent segment degeneration. In our study, MRI follow-up at 1 year showed no progression of degeneration in the unfused stable segments among patients in the selective fusion group, whereas one case of adjacent segment degeneration was observed in the dual-segment fusion group. This finding suggests that in dual-segment fusion strategies, the increased biomechanical burden on the adjacent segments due to extended fixation may elevate the risk of degeneration. 3 This finding supports the rationale that fusion may not be necessary for biomechanically stable segments.
Traditionally, open fusion surgery in cases of multilevel lumbar degeneration has favored the fusion of all involved segments to maximize spinal stability.3,14 However, the principle of minimally invasive spine surgery emphasizes “the least necessary intervention,” and selective fusion precisely aligns with this approach.15,16 Compared with conventional open fusion, endoscopic-assisted fusion minimizes paraspinal muscle injury, preserves posterior ligamentous structures, and reduces postoperative pain, thereby promoting faster rehabilitation. This study utilized endoscopic spinal surgery with precise decompression and fusion, which minimizes muscle disruption and postoperative scarring, and promotes faster recovery.
In recent years, multiple studies have supported the effectiveness of limited-segment fixation for multilevel degenerative spine diseases. For example, Okuda et al. reported that in patients with mild spondylolisthesis (Grade I), selective fusion, while preserving mobility at the unfused segment, led to significant long-term functional improvement without worsening adjacent segment degeneration. 17 Similarly, Park et al. showed that preserving slightly unstable segments helps maintain lumbar mobility, improves pain scores, and enhances patient satisfaction. 18 which further validates our results.
Furthermore, this study has practical clinical relevance. As a regional minimally invasive spine center, our institution advocates the principle of “minimized intervention”. 19 The selective fusion strategy adopted in this study aims to preserve segmental motion and reduce trauma, while ensuring neurological recovery and adequate fusion. This approach is particularly suitable for elderly patients or those with compromised general health status.20,21
Although the postoperative hospital stay did not differ significantly between the two groups, the operative time and intraoperative blood loss were markedly reduced, thereby lowering surgical risks. This finding indicates that selective fusion can effectively reduce intraoperative trauma without prolonging recovery, supporting its role as a safe and efficient minimally invasive strategy.
This study has several limitations. First, it was a single-center retrospective analysis, which may introduce selection and information biases. Second, the sample size was limited, and some patients had not completed the 6- or 12-months follow-up, potentially affecting the statistical power of certain results. Third, lumbar lordosis was not systematically measured, which may limit the evaluation of postoperative sagittal balance. Finally, the overall follow-up duration remains relatively short, making it difficult to fully assess long-term stability and the risk of adjacent segment degeneration (ASD). In this study, some patients have been followed up for 12 months, allowing a more comprehensive assessment of fusion status and clinical outcomes; however, at least 2 years of follow-up will be required to confirm long-term outcomes. A prospective extension of this cohort with a minimum follow-up of 24 months is currently ongoing. In future follow-up, particular attention will be paid to changes at more cranial adjacent levels (e.g., L3–4) to assess the risk of stenosis recurrence or degeneration above the index levels.
Despite these limitations, this study provides valuable early evidence supporting the feasibility and clinical value of selective fusion in bi-segmental lumbar spinal stenosis with segmental instability. Furthermore, the absence of a conventional open-surgery control group limits the ability to directly compare the advantages of endoscopic-assisted fusion, such as reduced paraspinal muscle trauma and preservation of posterior ligamentous structures. Future studies are planned to include an open-surgery cohort and to extend the follow-up to at least 2 years to provide more definitive evidence.
In conclusion, for patients with bi-segmental lumbar spinal stenosis and single-segment instability, selective fusion offers similar short-term efficacy to dual-segment fusion, while reducing surgical trauma and hospitalization burden. This approach reflects the clinical value of minimally invasive spine surgery that emphasizes “targeted precision and functional preservation and warrants further promotion in clinical practice.”
Footnotes
Ethical considerations
This retrospective study was reviewed by the ethics committee of Yichang Central People’s Hospital (Approval number: [2025-234-01]) following the Declaration of Helsinki. Informed consent was taken from all patients for their participation in the study.
Consent-for-publication
All published medical histories and photographs have been signed with informed consent from patients.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.