
Abstract
Study Design
Multicenter, prospective observational cohort study.
Objectives
109 patients with lumbar spine stenosis (LSS) undergoing minimally invasive decompression in 6 different centers (Germany, Italy, USA).
Methods
The demographic, surgical and clinical data was collected. Patients were examined preoperatively, immediately postoperatively, at 6 and 12 months after surgery with regard to pain (back and legs) and functional outcomes (ODI, SF-36, EQ5D).
Results
The mean age of the cohort was 67 ± 11 years, with a BMI of 31.8 ± 6.6 kg/m². Most patients (93%) underwent single-level decompression, and postoperative adverse events occurred in 17% of cases. Significant initial reductions in back (6.0 ± 2.8 to 2.4 ± 2.1) and leg pain (6.4 ± 2.1 to 2.1 ± 2.5) were observed (P < 0.001). However, pain levels increased significantly by the 12-month period, reaching 3.9 ± 2.7 for back pain and 3.9 ± 2.4 for leg pain (P < 0.001). Functional scores (ODI) improved from 43 ± 18 at baseline to 36 ± 18 post-treatment but showed no further significant change (P = 0.509) by 12 months. Health status (EQ5D index) improved from 0.53 ± 0.33 to 0.82 ± 0.16 immediately post-treatment but declined to 0.75 ± 0.21 by 12 months (P = 0.011). SF36 physical scores also showed initial improvement but plateaued at follow-ups. Notably, high BMI and prior spine surgery were associated with worse outcomes.
Conclusion
Although minimally invasive decompression without fusion initially led to a significant improvement in patients with LSS, the results deteriorated significantly over the course of the observation period. Future studies should focus on strategies to ensure sustained improvement in symptoms in patients with lumbar stenosis undergoing decompression procedure.
Keywords
Introduction
Lumbar spinal stenosis (LSS) is a common degenerative disease of the spine that occurs particularly in older adults. This disease leads to a narrowing of the spinal canal, compressing nerve roots and the spinal cord. This can lead to considerable pain, sensory deficits and motor impairments that severely affect the quality of life.1,2
Minimally invasive decompression has been established as an effective treatment method for alleviating the symptoms of LSS.3-5 However, there is a debate whether decompression alone or in combination with fusion should be performed. Despite the assumption that fusion may help stabilize the spine, numerous studies have shown that there are no significant differences in functional or pain outcomes between decompression alone and combined decompression with fusion.5-8 In addition, no differences in reoperation rate was reported, but the risk of sustaining major complications was 1.4 times higher in the decompression plus fusion group. 8 Reoperation rates of 17% and 16% for decompression without fusion and decompression with fusion after 5 years show no superiority of 1 of the 2 procedures.9,10 Ulrich et al. were unable to show superiority of 1 of the 2 surgical techniques, decompression without or with fusion, at 11% and 14%. 11 A national study with 1400 analyzed patients also showed no evidence of different reoperation rates after up to 10 years for after anterior fusion, posterior fusion, and decompression for the treatment of LSS. 12
Minimally invasive decompressions have reported a lower risk of revision compared to the open technique. 13
In a multi-center study Ulrich et al reported that patients in both fusion with decompression and decompression alone groups, presented strong improvement of symptoms after 6 months and that remained during the observation period of 3 years.5,14,15
The aim of the current study was to investigate the longitudinal change in post-operative functional outcomes in patients with LSS after minimally invasive decompression without fusion.
Methods
Data were collected in a prospective multicenter observational study in 6 spine centers (AO Spine Knowledge Forum Degenerative, DegenPRO, Clinical trials identifier: NCT02802033), focusing on the treatment of degenerative spinal conditions. The study was registered and evaluated by each participating center at the local ethics committee and institutional review board (Halle, Germany: 59/16; Murnau, Germany: mb20055, Bologna, Italy: 12944, Los Angeles, USA: 17-23094, New York (NYL), USA: IRB-AAAR6291, New York (NYM), USA: IRB-18-00012). Each patient signed a patient consent form after being informed about the study.
In the current study patients with spinal stenosis and surgical decompression without fusion at 1 or 2 levels were included. The diagnosis of lumbar spinal stenosis (LSS) was primarily based on a clinical assessment of characteristic symptoms, including activity-dependent neurogenic claudication with limited walking distance, and, in some cases, neurological deficits such as paresthesia or limb weakness. The decision regarding diagnosis and treatment was therefore primarily guided by the patient’s reported level of discomfort and functional impairment, rather than relying solely on imaging-based grading of stenosis severity. Only patients with lumbar spinal stenosis who were ambulatory prior to surgery and exhibited clinical symptoms consistent with stenosis were included in this study. Patients with instability or structural abnormalities that required stabilization via fusion were excluded to minimize the potential impact of coexisting pathologies on the study outcomes.
Additional exclusion criteria: Patients who underwent any fusion surgery; Recent history of substance abuse (ie, recreational drugs and alcohol) that would preclude reliable assessment; Pregnancy or women planning to conceive within the registry period.
Patients with spine deformity in the thoracic or lumbar spine that require long fusion (>4 levels); Patients having surgery for traumatic spine injuries (patients with previous unrelated spine trauma will not be excluded); Patients with spine infection or malignancy; Patients who didn’t received surgical treatment.
Patient’s demographics, symptom’s severity and their duration, pre-operative spine treatments were assessed. Smoking status, the Charlson Comorbidity Index (CCI) and the work status were collected. 16
Patients were evaluated at 4 time points: pre-operatively (baseline), after surgery during the hospital stay (treatment) and 6- and 12-month (FU1, FU2) after surgery. Intra- and post-surgical side adverse events, non-surgical side adverse events, surgery time and length of hospital stay were recorded. If AE required treatment, the treatment and the impact on patients’ health was categorized in the following 6 categories: I. no treatment required, no long-term effect II. Minor non-invasive treatment needed, no long-term effect III. Invasive/complex treatment (eg, surgery, ICU), likely temporary (<6 months) effect IV. Invasive/complex treatment (eg, surgery, ICU), likely prolonged (>6 months) adverse effect V. Significant neural injury or serious life/limb-threatening event VI. Adverse event resulting in death
As primary outcome variables the patients’ back pain (NRS-BP) and leg pain (NRS-LP) were used. Pain was evaluated using numeric rating scales from 0 to 10 for pain.
As secondary outcome variables the following patient related outcome measures were used: pain related functional disability using the Oswestry-disability Index (ODI), health status and subjective health status (EQ5D index value and EQ5D-VAS) and the mental and the physical scales of the SF36 (SF36-MSC, SF36-PSC).17-19
The surgical approach relieving the spinal compression consists primarily of an interlaminar fenestration. A paraspinous cut is set above the involved level(s), the muscles are retracted along the fiber structure to minimize the trauma and post-operative pain. The laminotomy or laminectomy is then performed. Using a microscope, the ligamentum flavum and bony attachments (osteophytes) were removed. When addressing more than 1 degenerated level surgically, the slalom technique was used in order to distribute the damage and reduce possible instabilities: the consecutive operated segments are reached from opposite paraspinous sides. 20 Finally, the spinal canal is checked for sufficient decompression and the soft tissues and skin layers are closed in layers.
The institutional research ethics board of each participating center approved the study protocol. All patients provided written informed consent for study participation. This study is approved by the Ethics Committee (reference number 59/16) and patient data acquisition and management is strictly according to the German data protection law. Furthermore, the statute of good clinical, declaration of Helsinki and scientific practice was followed.
Statistical Analysis
Multivariate linear mixed models (GLMM) were used to detect changes during the observation period in the primary and secondary outcome measures. The P-values and confidence limits for pairwise comparisons are calculated. In addition to P-values, the effect size (Cohen’s d) were calculated to describe the strength of change and to be able to compare the strength of change between the outcome measures. 21
The impact of confounding variables (gender, BMI, smoking status, single- or two-level decompression, prior spine treatment, CCI, and work status) was assessed by incorporating them as covariates in the GLMM. For better understanding, the direction of the impact of the significant covariates, Cohen’s d is given with as positive or negative values. Negative values indicate a worsening in the outcome values, positive values indicate an improvement in the outcome values.
The variance clarification of NRS-LP and NRS-BP regarding the secondary outcome variables are evaluated using bivariate correlation to calculate r2. The bivariate correlation between NRS and the secondary outcome variables was performed separate for each observation time point. Statistical analyses were performed in corporation with the AO Innovation and Translation Center (AO ITC) at the AO Foundation using the software SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
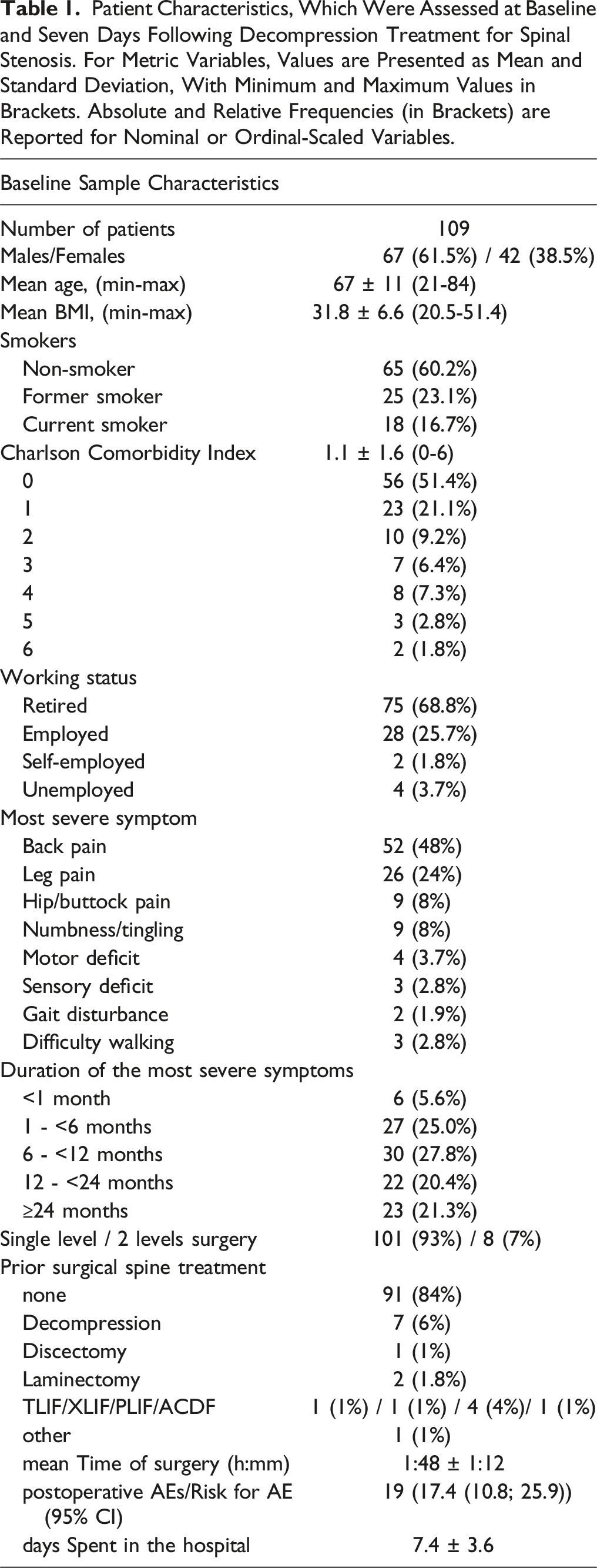
Patient Characteristics, Which Were Assessed at Baseline and Seven Days Following Decompression Treatment for Spinal Stenosis. For Metric Variables, Values are Presented as Mean and Standard Deviation, With Minimum and Maximum Values in Brackets. Absolute and Relative Frequencies (in Brackets) are Reported for Nominal or Ordinal-Scaled Variables.
In terms of primary and secondary outcome, data of up to 93 (baseline), 47 (treatment), 73 (6 months FU) and 62 patients (12 months FU) were available for analysis.
Mean observation time was 6 ± 9 days (median 4 days, Q1: 1, Q3: 7 days) for the time point “treatment” after the baseline, 6 ± 1 months for the 6-month follow-up visit and 12±1months for the 12 months follow up.
Sixty-six (70%) of the patients had persistent symptoms for more than 6 months. Ninety-one patients (84%) had no previous spine treatment/surgery. 22% did not receive any treatment before participating in the current study, 3% had received epidural corticosteroid injections and 71% were taking pain medication.
The surgical time was 1:48 ± 1:12 hours. Most of the cases (93%) received single level decompression. In 8 cases (7%) 2 level decompression were performed in slalom technique. None of the patients showed intraoperative adverse events.
Overview of Adverse Events of Patients after Decompression Surgery of Spinal Stenosis Without Surgical Fusion.
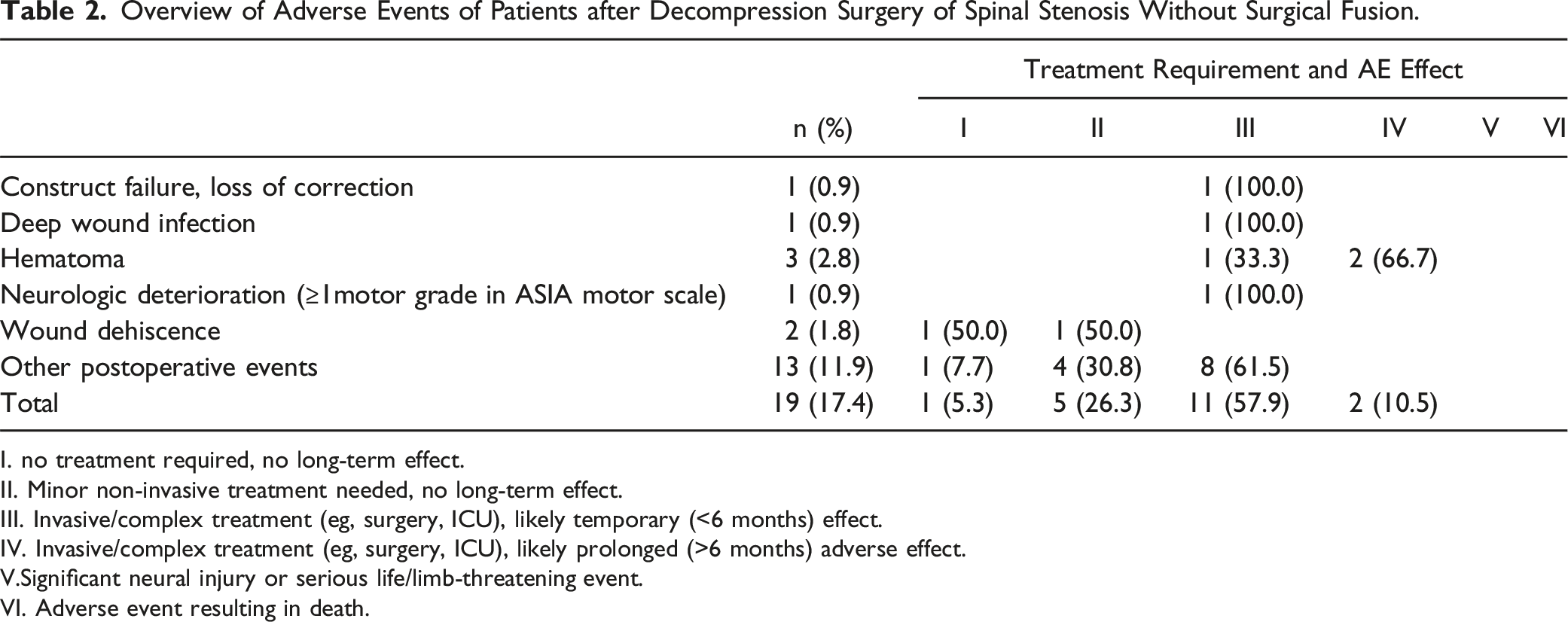
I. no treatment required, no long-term effect.
II. Minor non-invasive treatment needed, no long-term effect.
III. Invasive/complex treatment (eg, surgery, ICU), likely temporary (<6 months) effect.
IV. Invasive/complex treatment (eg, surgery, ICU), likely prolonged (>6 months) adverse effect.
V.Significant neural injury or serious life/limb-threatening event.
VI. Adverse event resulting in death.
Back Pain (NS-BP) and Leg Pain (NRS-LP)
A significant initial reduction in pain from 6.0 ± 2.8 (baseline) to 2.4 ± 2.1 (time of treatment) was observed (P < 0.001, Figure 1). While at 2nd FU (12 months), patients reported less pain compared to the baseline (3.9 ± 2.7, P < 0.001) the back pain levels increased by 1.6 ± 3.4 points (P = 0.002) from surgery to 12 months. This increasing pain underlies a medium to strong effect with Cohen’s d of 0.65. Outcome after decompression surgery of spinal stenosis for: (A) Back pain (NRS-BP), (B) leg pain (NRS-LP), (C) Oswestry Disability Index (ODI), (D) health status (EQ5D index value), (E) subjective health status (EQ5D-VAS), (F) the physical and G) mental health scale of the SF36 (SF36-PCS, SF36-MCS). Results are given as mean and its 95% confidence interval (CI) as error bars. P-values for significant differences are given in the figure.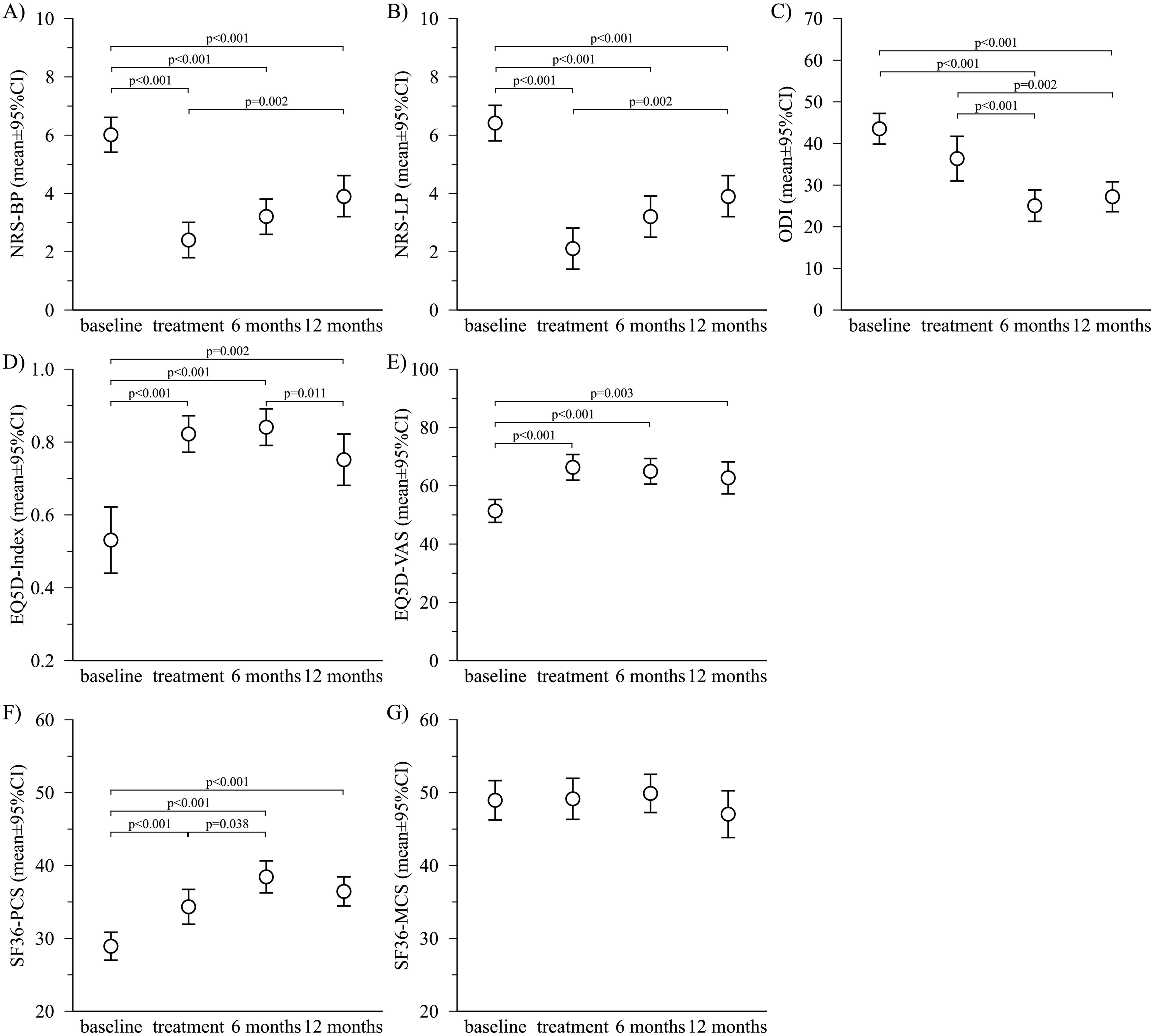
There was no change in pain after treatment within the 6-month follow-up (P = 0.124) and also no sig. Change from the 6 to 12-month FU (P = 0.054). The strongest effect size are therefore recorded immediately after treatment, but this effect size is reduced over the observation period. After 12 months, there is still reduced pain, compared to the baseline, but the patients report significant more severe pain after 12 months than after treatment.
A very similar change is apparent for leg pain (NRS-LP, Figure 1). After an initial strong reduction in leg pain from 6.4 ± 2.8 (baseline) to 2.1 ± 2.5 (treatment, P < 0.001), leg pain was 3.9 ± 2.4 after 12 months. From treatment to 12 months pain increased by 1.9 ± 3.7 points (P = 0.002) indicating a strong effect with Cohen’s d of 0.76. In NRS-LP points, the pain reported after 12 months is approximately twice as severe, compared to pain after treatment.
There was no change in pain after treatment within the 6-month follow-up (P = 0.115) and also no sig. change from the 6 to 12-month FU (P = 0.153).
ODI, EQ5D and SF-36
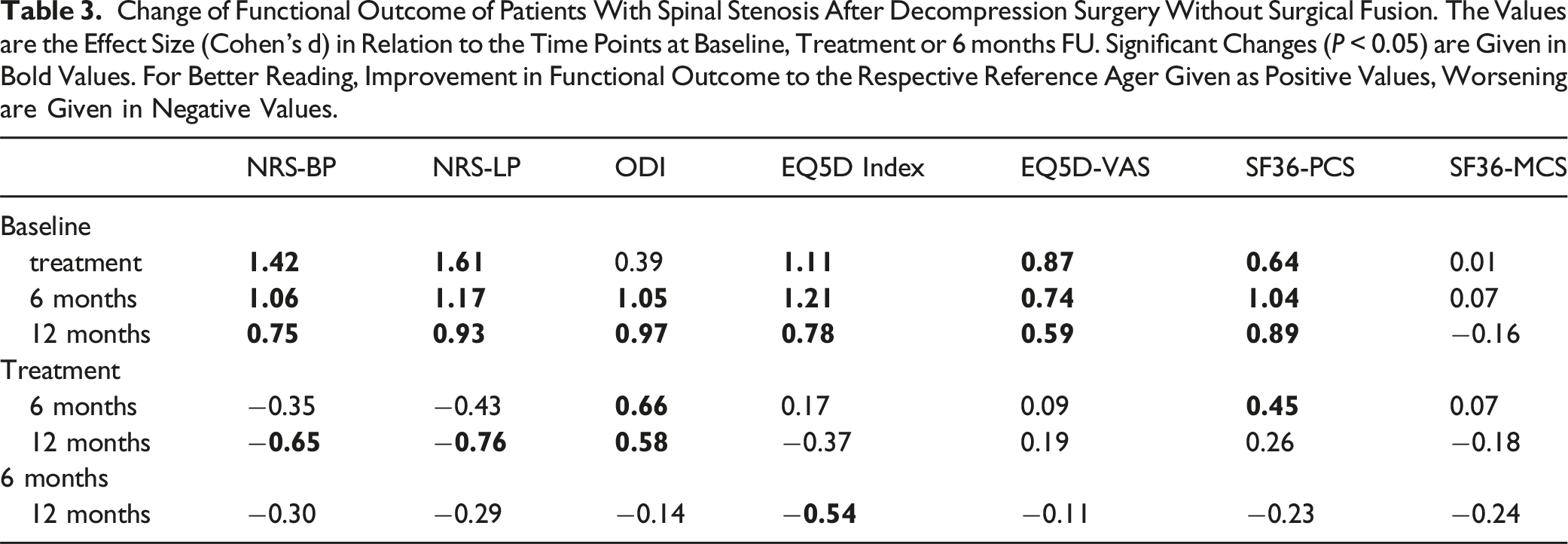
Change of Functional Outcome of Patients With Spinal Stenosis After Decompression Surgery Without Surgical Fusion. The Values are the Effect Size (Cohen’s d) in Relation to the Time Points at Baseline, Treatment or 6 months FU. Significant Changes (P < 0.05) are Given in Bold Values. For Better Reading, Improvement in Functional Outcome to the Respective Reference Ager Given as Positive Values, Worsening are Given in Negative Values.
The patients’ health status (EQ5D index value) improved directly after treatment (baseline 0.53 ± 0.33, treatment 0.82 ± 0.16, P < 0.001, Cohen’s d = 1.11). Twelve months after decompression surgery the patients’ health status deteriorated over time. At 12 month the EQ5D index value was 0.75 ± 0.21, which was significantly decreased by 0.10 points from 0.84 ± 0.14 after the 6 months (P = 0.011).
The subjective health status (EQ5D-VAS) also showed a strong improvement (Cohen’s d = 0.87) after the treatment (baseline 51 ± 18%, treatment 66 ± 15%, P < 0.001). During the observation period between treatment and the 12 months follow up, no significant change in subjective health status was found (P > 0.676, Table 3).
The physical sum scale of the SF36 (SF36-PCS) improved between baseline (28.9 ± 8.8) and treatment (34.3 ± 8.0, P < 0.001, Cohen’s d = 0.64). Six months after surgery the SF36-PCS showed further improvement (38.4 ± 9.4, P < 0.001, Cohen’s d = 0.45). There was no significant change in the SF36-PCS from 6 to 12 months (36.4 ± 7.7, P = 0.123).
For the mental sum scale (SF36-MCS), no significant changes were found from baseline to the 12-month follow-up (P > 0.654).
In the last 6 months of the observation period (6- and 12-month follow-ups), the effect sizes show small to moderate trend for deteriorations, though not all changes showed significance (Table 3).
Among the covariates, BMI was found to have impact on NRS-LP, ODI, EQ5D index, EQ5D-VAS and both SF36 scores (P < 0.001). The higher the BMI, the worse the outcome. The negative influence here varies between low (NRS-LP regression coefficient = 0.09) and very strong (ODI regression coefficient = 0.94).
The smoking status showed a strong effect on NRS-LP with a regression coefficient of 2.08 (P < 0.001). Smoking led to higher NRS-LP compared to non-smoker.
Prior surgical treatments showed an impact on the ODI (regression coefficient = 12.44), EQ5D-VAS (regression coefficient = −10.99) and SF36-PCS (regression coefficient = −4.61). Patients with prior surgery showed worse outcomes, compared to patients without prior spine surgery.
The bivariate correlations of both pain scales (NRS-BP and NRS-LP) with the other outcome variables (ODI, EQ5D index value, EQ5D-VAS, SF36-PCS and SF36-MCS) show significance with P < 0.01 for all pairings. Back pain (NRS-BP) shows the highest correlations with the EQ5D-VAS of r = −0.69 (r2 = 0.47) on average over all observations. The average r for NRS-LP was −0.40 (r2 = 0.16). For NRS-LP, the highest mean correlations with r = 0.64 (r2 = 0.40) can be found with the ODI and with r = −0.65 (r2 = 0.42) for the EQ5D Index Value. The mean values for the NRS-BP are lower here (ODI r = 0.49, r2 = 0.242; EQ5D-Index Value r = −0.42, r2 = 0.18).
Discussion
The aim of the current study was to evaluate functional outcomes and their change over time in patients undergoing standalone minimally invasive decompression for lumbar spinal stenosis (LSS). The results showed significant initial improvements in both back pain (NRS-BP) and leg pain (NRS-LP), which were maintained at the 12-month follow-up, although the intensity of reported pain nearly doubled during the follow-up. Despite this increase, pain remained significantly below the preoperative values. Even though the treatment did not relief pain free at any time. A similar trend was found for the functional outcome parameters. The ODI and SF36-PCS were the only ones to improve even up to the 6-month follow-up. Mental health (SF36-MCS) showed no significant changes during the entire study period.
The observed reduction in back and leg pain immediately after decompression surgery underscores the effectiveness of this surgical approach in rapidly relieving the symptoms of LSS and is in line with the literature.5,8,22
The sustained improvement in pain scores and functional outcomes at 12 months, despite some increase in pain over time, suggests that the benefits of decompression without fusion may persist for at least 1 year postoperatively. This is consistent with previous studies suggesting that decompression alone can effectively treat LSS symptoms without the need for fusion, which is associated with higher risks (subsequent degeneration and loss of motion in the segment) and costs.23-27
However, statistically increase in pain during the postoperative period highlights a potential recurrence of symptoms due to ongoing degenerative processes or other factors such as physical activity and adherence to postoperative care. Austevoll et al showed higher reoperation rate for patients after decompression without fusion, compared to decompression with fusion, 3 but other studies showed no significant association between decompression alone or fusion and the need for revision surgery after 3 years. 11
This and our results are in contrast to the single center study of Huang et al and the Sunderland et al, which each show constant reduction in pain, functional improvements and patients’ satisfying during the whole observation period of up to 1 and 2 years.28,29
Decompression only addresses symptoms localized to the affected region and does not influence the progression of degeneration. Postoperative compliance of patients regarding conservative therapies and rehabilitation was not systematically recorded. Therefore, no statements can be made in this regard and represent an additional limitation of the study results, especially since no comparison or control group was included and thus no randomization of a further form of therapy (eg, decompression with fusion).
A systematic review and meta-analysis in 2018 showed better outcome in the ODI, leg and back pain for decompression compared to decompression with fusion. 30 The authors did not consider the period between treatment and outcome in the literature used. Based on our data, we show that this period is important with regard to the outcome and also depends on it. However, whether both techniques change comparably over time remains an open question.
Karlsson et al. (2024) showed that the ODI showed no improvement at 5 years after decompression and fusion following spinal stenosis surgery with or without spondylolisthesis, which was consistent with their 2-year interim results. 31 Extrapolating from our data may lead similar results. In the subgroup of patients without spondylolisthesis, significantly more patients showed pain reduction (80%) after decompression alone compared to patients after decompression and fusion (58%). The risk of reoperation was comparable (22% for decompression alone, 24% for decompression with fusion) and concluded that decompression alone should be the preferred method for spinal stenosis surgery.
Risk factors for poorer outcomes include higher preoperative pain, greater disability, smoking, obesity, prior surgery, and surgical complications.32-34 Smoking, in particular, was associated with leg pain in our study, likely due to arterial circulation disorders. Evidence on nicotine’s role is mixed, with studies indicating both analgesic effects and chronic pain hypersensitivity.35,36 Behavioral interventions to address smoking and other risk factors may improve outcomes, as confirmed by previous studies.37,38
The inclusion of a comprehensive set of widely used outcome measures, including pain scores, indices of functional disability and health status assessments, allows a robust assessment of the impact of decompression surgery on patients’ quality of life and comparison with other studies. However, our study also has limitations. While the follow-up period of 12 months is sufficient to observe medium-term outcomes, it may not capture the long-term durability of the surgical benefits. In addition, while the sample size is sufficient to detect significant changes, it may limit the generalizability of the results to all populations, particularly those with more severe comorbidities or other demographic characteristics. Future research should therefore not only focus on long-term outcomes of decompression surgery without fusion to better understand the durability of symptom relief and functional improvement, but also differentiate between patients who improve or deteriorate particularly strongly. Older age, obesity, greater pre-operative pain and disability and lower quality of life are associated with risk of poor walking ability post-operatively. 37 Greater pre-operative walking and higher education are associated with reduced risk of poor walking ability post-operatively. 38 Patients should be informed about their risk of poor outcomes and considered for rehabilitation to enhance walking ability and optimize surgical results. 16
In summary, minimally invasive decompression for lumbar spinal stenosis without fusion provides significant and lasting relief of back and leg pain, improves functional outcomes and enhances overall health. The benefits are detectable up to 12 months after surgery, although an increase in pain over time indicates the need for continued patient care. The results of microsurgical decompression in terms of adverse events are positive, as less than 1/5 of the patients had an adverse event after treatment, while of the patients with adverse events; there was no long-term effect of these adverse events anywhere.
The recommendations from our findings are limited by our study design, so we would only recommend alternative therapies for patients with higher BMI, smoking habits or previous surgery. Behavioral changes are advisable for these patients and surgeons may want to consider alternative therapies. For future studies on degenerative diseases, we recommend longer follow-up periods and, if possible, early pre-screening. To reduce selection bias, we recommend treatment randomization and the conduction of objective post-therapy assessments, including activity monitoring. Further consideration of patient-physician communication and treatment expectations could improve follow-up.
These results suggest that minimally invasive decompression can greatly alleviate the symptoms of LSS in the short term and effectively in the medium term, leading to a gain in physical function, maybe due to significantly reduced pain.
Supplemental Material
Supplemental Material - Pain and Functional Outcome After Microsurgical Decompression of Lumbar Spinal Stenosis: Very Short- and Long-Term Postoperative Analysis
Supplemental Material for Pain and Functional Outcome After Microsurgical Decompression of Lumbar Spinal Stenosis: Very Short- and Long-Term Postoperative Analysis by Carolin Graebsch, Zorica Buser, Sophie Leroy, Jeffrey C. Wang, Tim Yoon, Stefan Bone, Hans Jörg Meisel, Philipp Schenk, AO Spine Knowledge Forum Degenerative in Global Spine Journal.
Footnotes
Acknowledgments
AO Spine is a clinical division of the AO Foundation which is an independent medically-guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department and AO’s Clinical Investigation and Documentation unit. Special thanks go to Esther Herrmann and Yvonne Minkus, whose support in data collection and training regarding the registry was essential for this work, and to Dimitri Hauri, who performed the statistical analyses. Last but not least, we would like to thank all patients for their contribution to the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine experts.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.