
Abstract
Purpose:
To describe the reduction technique of thoracolumbar burst fracture using percutaneous monoaxial screws and its radiological outcomes compared to polyaxial screws.
Methods:
All surgeries were performed by minimally invasive technique with either percutaneous monoaxial or percutaneous polyaxial screws inserted at adjacent fracture levels perpendicular to both superior end plates. Fracture reduction is achieved with adequate rod contouring and distraction maneuver. Radiological parameters were measured during preoperation, postoperation, and follow-up.
Results:
A total of 21 patients were included. Eleven patients were performed with monoaxial pedicle screws and 10 patients performed with polyaxial pedicle screws. Based on AO thoracolumbar classification system, 10 patients in the monoaxial group had A3 fracture type and 1 had A4. In the polyaxial group, six patients had A3 and four patients had A4. Total correction of anterior vertebral height (AVH) ratio was 0.30 ± 0.10 and 0.08 ± 0.07 in monoaxial and polyaxial groups, respectively (p < 0.001). Total correction of posterior vertebral height (PVH) ratio was 0.11 ± 0.05 and 0.02 ± 0.02 in monoaxial and polyaxial groups, respectively (p < 0.001). Monoaxial group achieved more correction of 13° (62.6%) in local kyphotic angle compared to 8.2° (48.0%) in polyaxial group. Similarly, in regional kyphotic angle, 16.5° (103.1%) in the monoaxial group and 8.1° (76.4%) in the polyaxial group were achieved.
Conclusions:
Monoaxial percutaneous pedicle screws inserted at adjacent fracture levels provided significantly better fracture reduction compared to polyaxial screws in thoracolumbar fractures.
Keywords
Introduction
Seventy percent of all spinal fractures occur at the thoracolumbar junction and burst fractures constitute about 14% of these fractures. 1 Thoracolumbar burst fractures can be divided into stable and unstable fractures. Surgery may be indicated for unstable burst fractures. 2 Surgical approaches for treatment of burst fracture can be from anterior, posterior, or combined anterior–posterior. 3 Anterior approach surgeries can achieve good radiological and clinical outcomes but it may be technically more difficult leading to profuse bleeding, prolonged surgery, deep infection, and organ injuries. 4 –7 Several studies had shown that similar clinical and radiological outcomes can be achieved with posterior approach surgeries. 8,9 The load sharing classification had outlined some guidelines on which approach to be recommended to prevent failure of fixation. 10
The usage of minimally invasive spine surgery utilizing percutaneous pedicle screws (PPS) had been more widely accepted because it can potentially reduce the operative time and hospitalization, reduce intraoperative bleeding, achieve earlier functional recovery, and minimize trauma to the paraspinal muscles. 11 –14 The safety of minimally invasive PPS had been reported to be safe in both cadaveric and clinical studies. 15 –17 There were studies that showed the radiological outcomes of minimally invasive fracture stabilization were comparable to open method in kyphotic angle correction and vertebra height restoration. 18 –25 However, the technique of using the monoaxial PPS for fracture reduction in unstable thoracolumbar burst fractures had not been widely reported. Blondel et al. 26 reported the use of monoaxial PPS in the treatment of burst fractures. They compared the outcomes of 7 patients using short segment monoaxial PPS reduction prior to cemented balloon kyphoplasty with 22 patients with reduction using cemented balloon kyphoplasty prior to stabilization with polyaxial PPS.
Based on the English literature review, there were no studies that describe the technique of fracture reduction using monoaxial PPS for thoracolumbar fractures without anterior augmentation. Therefore, this study aimed to compare between monoaxial PPS reduction technique and polyaxial PPS stabilization technique for thoracolumbar fractures.
Materials and methods
Study design
This was a retrospective review of prospectively collected data of patients with thoracolumbar burst fractures treated with minimally invasive stabilization (MISt) in a tertiary academic institution from September 2013 to June 2017. In our early practice, polyaxial PPS screws were used in all instrumented levels. Monoaxial PPS screws were only utilized since May 2015. Inclusion criteria were patients, who had thoracolumbar burst fractures secondary to trauma, treated with MISt at our center. Patients who underwent open posterior stabilization surgery or anterior surgery, patients with pathological fractures secondary to malignancy, osteoporosis or infection, and patients with incomplete medical records were excluded. Ethical approval was obtained. Informed consents were taken from patients. All patients underwent routine preoperative imaging: anteroposterior (AP) and lateral plain radiograph and computed tomography (CT) of the spine. All patients had instrumentation two levels above and two levels below the fracture.
Patient population
Patients were divided into two groups: (1) monoaxial PPS group and (2) polyaxial PPS group. In the monoaxial PPS group, monoaxial PPS were inserted to the adjacent vertebrae above and below the fractured vertebra, parallel to the superior end plate of the corresponding vertebra. Polyaxial PPS were inserted to the distant levels. In the polyaxial PPS group, polyaxial PPS was used in all instrumented levels.
Data collection
Clinical data collected were age, gender, mechanism of injury, fracture level, load sharing classification score, AO spine thoracolumbar spine injury classification, duration of follow-up, preoperative, and postoperative neurological status based on ASIA impairment scale, operative time, and intraoperative blood loss.
Preoperative and postoperative radiological parameters (Figure 1) collected and calculated were:
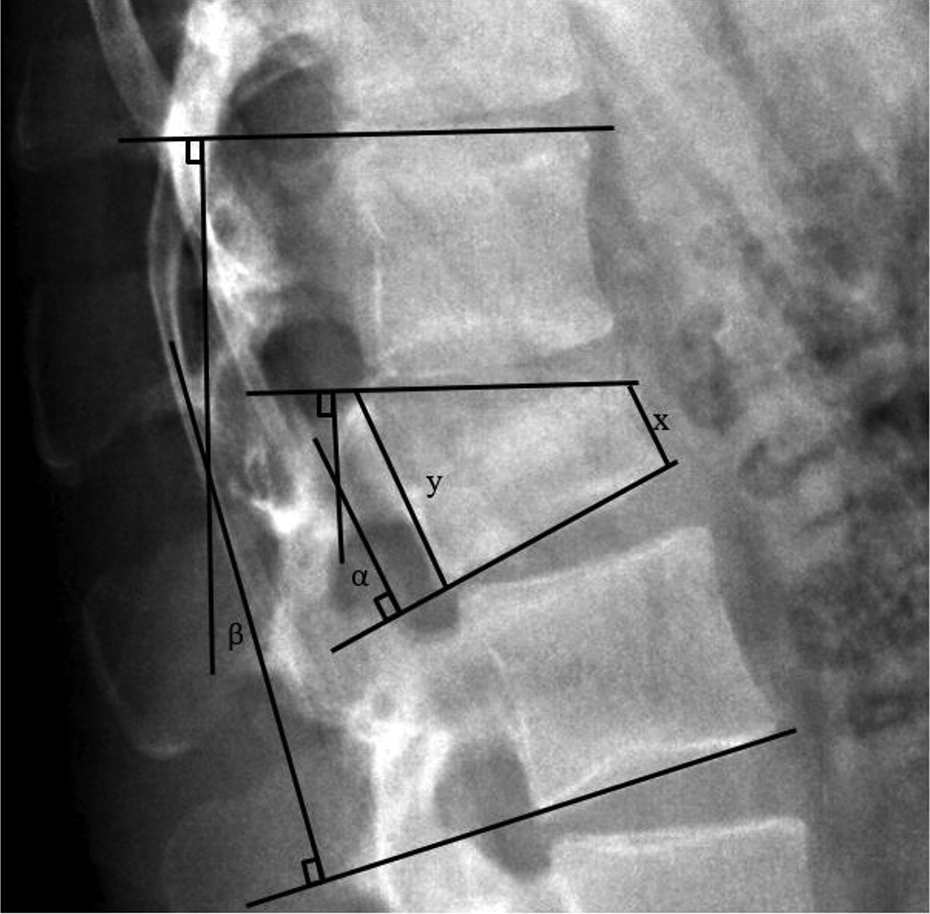
Measurements of radiographic parameters. α: LKA; β:RKA; x: AVH; y: PVH. LKA: local kyphotic angle; RKA: regional kyphotic angle; AVH: anterior vertebral height; PVH: posterior vertebral height.
Local kyphotic angle (LKA) (°): Angle subtended by a line drawn along the superior end plate and the inferior end plate of the fractured vertebra.
Regional kyphotic angle (RKA) (°): Angle subtended by a line drawn along the superior end plate of the vertebra above and the inferior end plate of the vertebra below the fracture.
Anterior vertebral height (AVH) (mm): Distance measured between the anterosuperior end plate and anteroinferior end plate of the fractured vertebra.
AVH ratio: AVH of the fractured vertebra divided by the AVH of the normal vertebra below.
Posterior vertebral height (PVH) (mm): Distance measured between the posterosuperior end plate and posteroinferior end plate of the fractured vertebra.
PVH ratio: PVH of the fractured vertebra divided by the PVH of the normal vertebra below.
Sagittal compression (SC) ratio: Narrowest sagittal width of the spinal canal of the fractured vertebra divided by the sagittal canal width of the normal vertebra below (on CT scan).
Total correction of each parameter: Difference between the postoperative and preoperative value.
Loss of correction of LKA or RKA: Difference between LKA or RKA at the final follow-up and postoperative period.
Surgical techniques
Positioning
Patients were positioned prone on a four-post frame on a Jackson table to allow good fluoroscopic visualization of the vertebral anatomy. Positioning of the patient with four posts applied under the chest and anterosuperior iliac spine with slight hip extension allowed some passive reduction of the spinal fracture.
PPS insertion
PPS were inserted simultaneously on both sides by two surgeons to reduce operative time and radiation exposure. A true AP view of the corresponding vertebra was initially obtained, in which both superior and inferior end plates were parallel and both pedicles were equidistant from the spinous process. A skin incision of 1.5 cm was made lateral to the lateral edge of the pedicle. The fascia was separated, and the muscles were split parallel to its fibers. Two 11G trocars were placed at the lateral edge of the pedicle (3 o’clock on the right side and 9 o’clock on the left side). The trocar was then advanced medially parallel to the superior end plate. When the tip of the trocar approached the medial wall of the pedicle on AP view, a lateral view was obtained. The tip of the trocar on lateral view should be at or slightly deeper than the posterior vertebral border. The trocar was advanced until the middle of the vertebral body. A guidewire was inserted. The screw length was measured. The screw was inserted along the direction of the guidewire, avoiding inadvertent guidewire advancement. Similar steps were repeated for other planned instrumentation vertebrae. In monoaxial PPS group, the monoaxial PPS screws must be inserted “parallel” to the superior end plate of the adjacent vertebrae. Polyaxial PPS screws were inserted at the distant vertebrae (Figure 2).
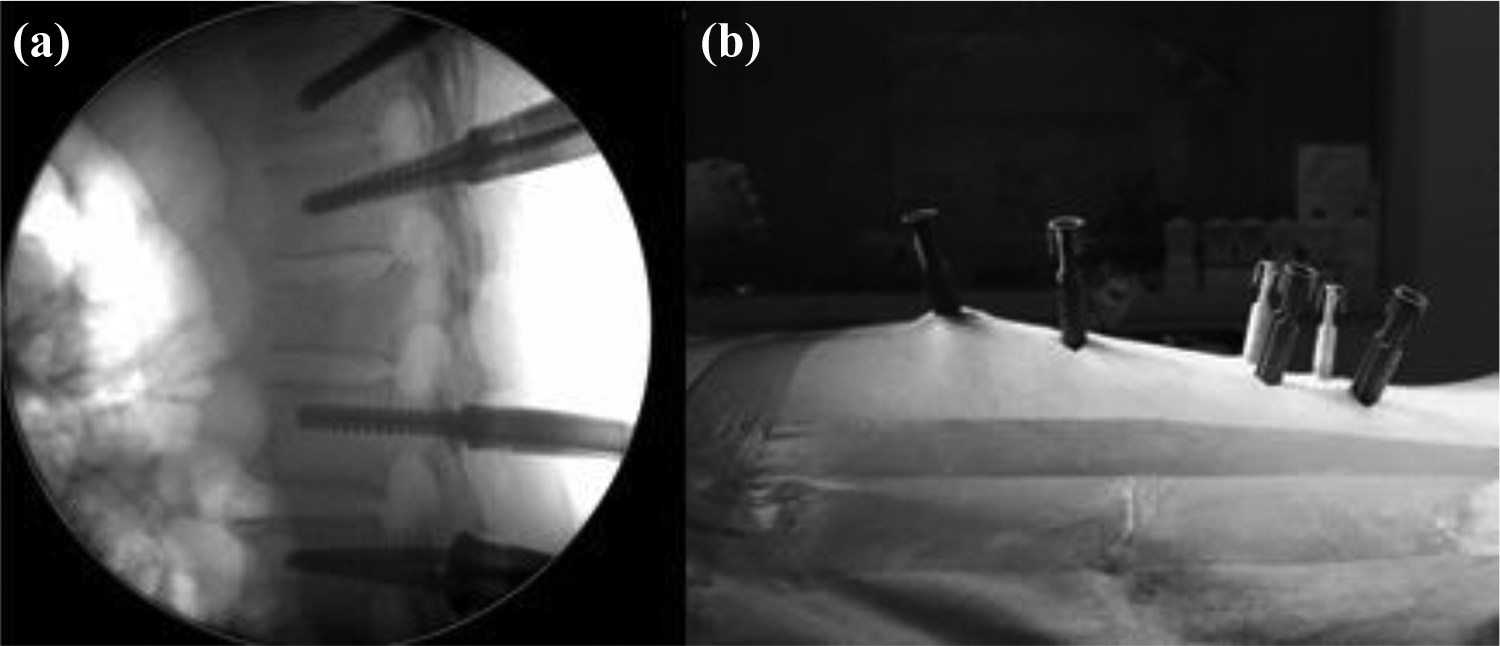
(a and b) Monoaxial screws were inserted parallel to the superior end plates of the vertebrae adjacent to the fractured vertebra.
Rod contouring
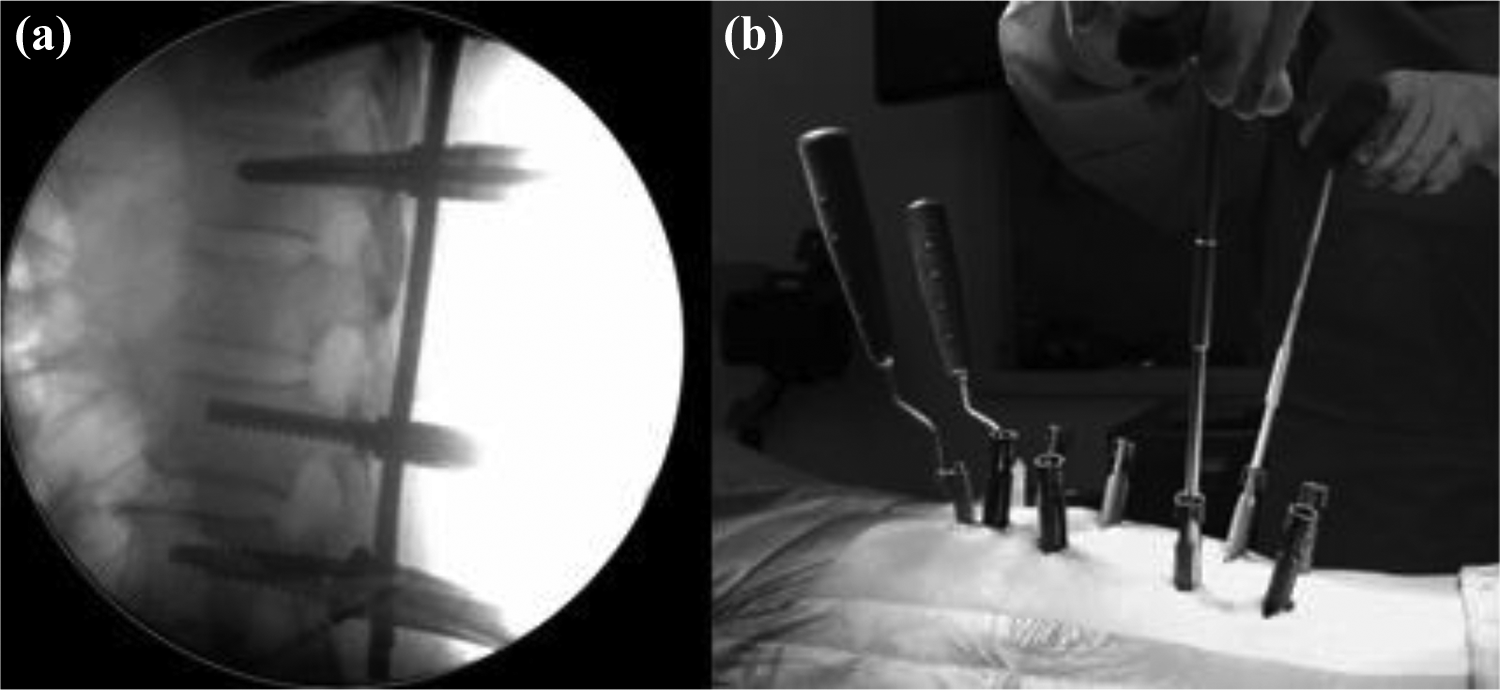
An extension of the screw sleeve was used to mimic the final position of the rod when seated in the screw head. The rod was contoured to mimicked the normal sagittal spinal alignment of the affected region with the help of the screw sleeves and extensions. Rods were inserted from a cephalad to caudal direction (Figure 3).

(a and b) Rods were precontoured according to the normal sagittal alignment of the spine.
Reduction techniques
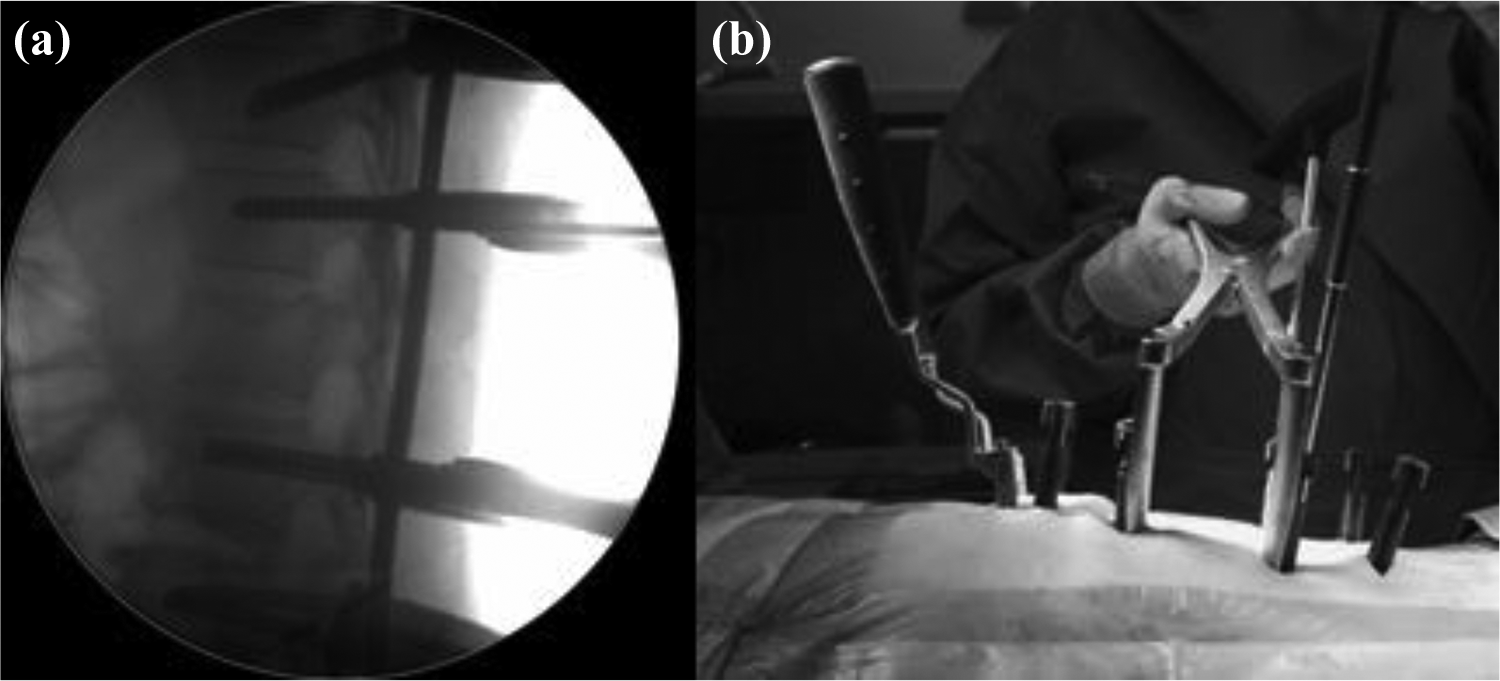
In the monoaxial PPS group, tightening of the screw nuts with contoured rods on monoaxial pedicle screws which were inserted parallel to the superior end plate formed a 90°–90° screw-rod construct. This allowed correction of the AVH and kyphotic angle (both RKA and LKA) of the fractured vertebra (Figure 4). For correction of the PVH, a distraction maneuver was performed using a distractor device, which was applied to the monoaxial screw sleeves at the adjacent levels above and below the fracture (Figures 5 and 6). Final tightening of the whole construct was performed. Deep fascia and skin were closed.
(a and b) Tightening of the screw nuts with the precontoured rods formed a 90–90 screw-rod construct. This enabled the correction of the AVH of the fractured vertebra. AVH: anterior vertebral height.

(a and b) Predistraction stage. A distractor device was inserted on the screw extension sleeves of the monoaxial screws inserted at the adjacent vertebrae.
(a and b) Application of distraction maneuver using the distractor device at the adjacent vertebrae with monoaxial screws increased the PVH of the fractured vertebra. PVH: posterior vertebral height.
The schematic diagrams to illustrate how percutaneous monoaxial PPS screws can be used to achieve fracture reduction were shown in Figure 7.

(a) Schematic diagram to illustrate the tightening of screw nuts with the rod onto the monoaxial screws adjacent to the fractured vertebra forms a 90–90 screw-rod construct, which enables correction of the AVH. (b) Schematic diagram to illustrate the correction of PVH with a distraction maneuver using a distractor device applied onto the monoaxial screws adjacent to the fractured vertebra. AVH: anterior vertebral height; PVH: posterior vertebral height.
Statistical analysis
Student’s t-test was used for comparison of continuous variables, whereas χ 2 tests were used for categorical variables. Analyses were performed with IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA) with statistical significance, p value <0.05.
Results
A total of 21 patients were recruited, 11 patients in the monoaxial PPS group, whereas 10 in the polyaxial PPS group. Demographic and perioperative data are illustrated in Table 1. Although the differences in follow-up and mechanism of injury between monoaxial and polyaxial PPS groups were significant, the difference in fracture morphology was not significant. The timing from trauma to surgery between both groups was not significant (4.6 ± 1.4 days and 2.5 ± 0.9 days in monoaxial and polyaxial groups, respectively, p = 0.309). There were no significant differences when comparing other demographic parameters between both groups. There were also no significant differences in operative time and intraoperative blood loss in both groups. No patient required blood transfusion. One patient had superficial surgical site infection, which was treated successfully with antibiotics and dressing. There was no implant failure.
Demographic and perioperative data comparing between monoaxial and polyaxial PPS groups.
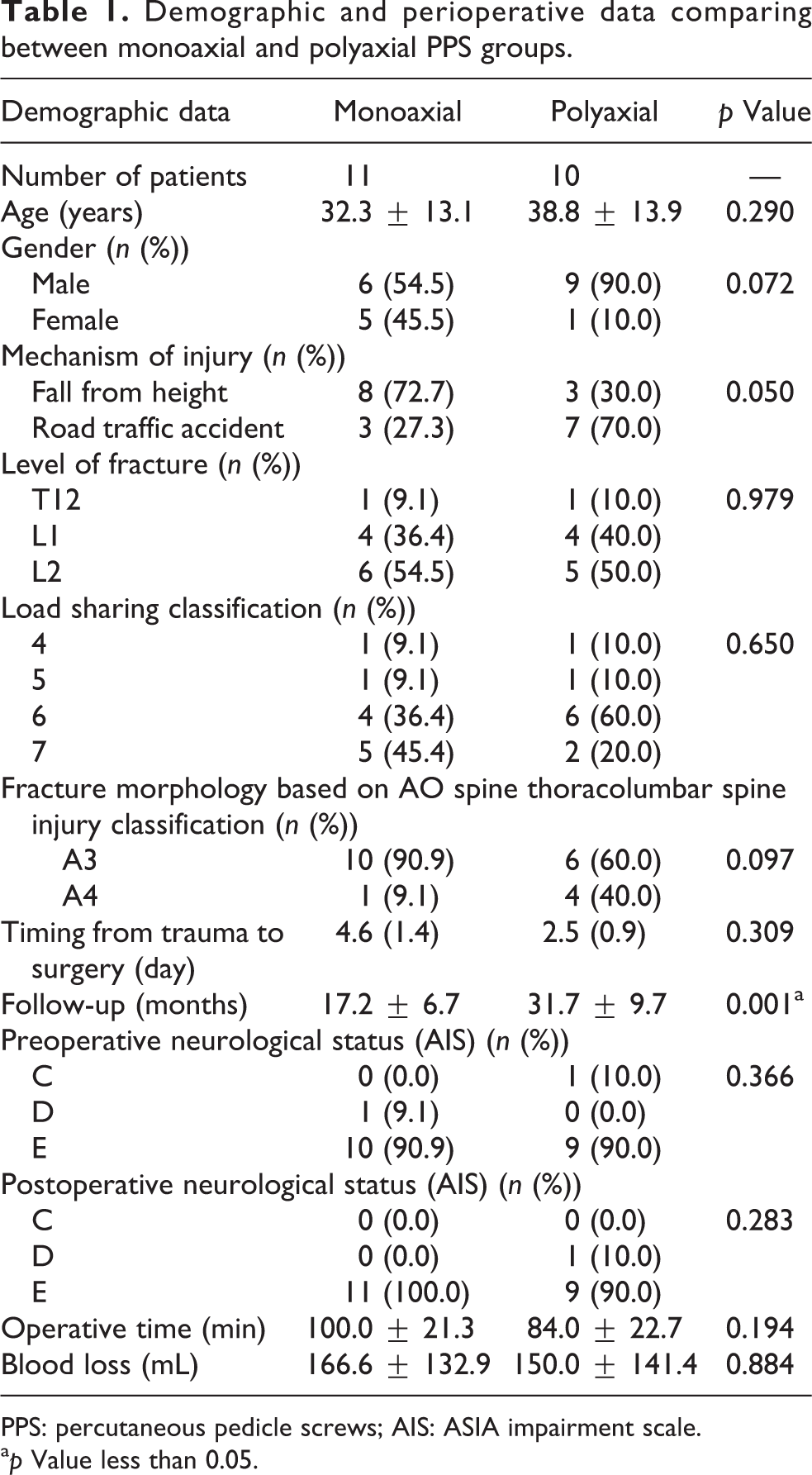
PPS: percutaneous pedicle screws; AIS: ASIA impairment scale.
a p Value less than 0.05.
Preoperative and postoperative neurological statuses were not significantly different between both groups. All patients achieved fracture union confirmed by CT scan (Figure 8).

Sagittal images of CT of a 24-year-old lady with an A3 fracture of L1 vertebra; (a) preoperative, (b) immediate postoperative, and (c) final follow-up at 12 months, showed fracture union with correction of kyphotic angle (RKA and LKA) and vertebral height (AVH and PVH) following PPS with monoaxial screws inserted at adjacent vertebrae. CT: computed tomography; LKA: local kyphotic angle; RKA: regional kyphotic angle; AVH: anterior vertebral height; PVH: posterior vertebral height; PPS: percutaneous pedicle screws.
For radiological parameters, there were significant differences in total correction of LKA, RKA, AVH ratio, PVH ratio, and SC ratio between both groups (Table 2). Total correction of LKA in monoaxial PPS group was significantly higher (13.1 ± 4.6°; 62.6%) than polyaxial PPS group (8.2 ± 5.7°; 48.0%) (p = 0.042). In RKA, total correction was twice higher in monoaxial PPS group (16.5 ± 6.4°; 103.1%) than in polyaxial PPS group (8.1 ± 5.0°; 76.4%) (p = 0.004). Monoaxial PPS group had significantly higher correction of AVH ratio (0.30 ± 0.10) than polyaxial PPS group (0.08 ± 0.07; p < 0.001). For PVH ratio, monoaxial PPS group had significantly more correction (0.11 ± 0.05) than polyaxial PPS group (0.02 ± 0.02; p < 0.001). Total correction of SC ratio in monoaxial PPS group was twice higher (0.30 ± 0.16) than in polyaxial PPS group (0.15 ± 0.13; p = 0.041).
Radiological parameters comparing between monoaxial and polyaxial PPS groups.

LKA: local kyphotic angle; RKA: regional kyphotic angle; AVH: anterior vertebral height; PVH: posterior vertebral height; SC: sagittal compression; PPS: percutaneous pedicle screws.
a p Value less than 0.05.
At the final follow-up (monoaxial PPS group: 17.2 ± 6.7 months and polyaxial PPS group: 31.7 ± 9.7 months), although not significant, there was loss of correction in LKA and RKA in both groups. In the monoaxial PPS group, the loss of correction in LKA was 1.8 ± 2.7° compared to 1.6 ± 1.8° in polyaxial PPS group. Whereas for RKA, the loss of correction was 2.2 ± 1.6° in monoaxial PPS group and 2.0 ± 1.4° in polyaxial PPS group.
Discussion
The introduction of MISt with the PPS system in the treatment of thoracolumbar fractures has reduced the morbidity associated with open surgery, such as longer operative time, increased intraoperative bleeding, longer duration of stay, higher infection rate, and slower recovery. 11,12,14,19 MISt also offers the advantage of long-segment fixation without much soft tissue damage. 27 Many authors had reported comparable clinical 20,21 and radiological outcomes 19,22 –25 between MISt and open technique. Kumar et al. 23 compared 23 patients treated with open surgery and 25 patients with mini-open surgery, both groups with monoaxial pedicle screws, and reported similar correction of kyphosis of 87% (from 25° preoperatively to 4° postoperatively) and no loss of correction after removal of implant 1 year later. Pelegri et al. 24 treated 15 fractures with MISt using polyaxial PPS and found good kyphotic correction (LKA from 16° to 8.1° and RKA from 12° to 2.5°) with minimal loss of correction (1.1° for LKA and 2.5° for RKA). McAnany et al. 25 in his meta-analysis reported no significant difference between open and percutaneous surgery in terms of vertebral body height and kyphotic angle. Wang et al. 19 also reported no difference in kyphotic angle, AVH ratio, and SC ratio in his study comparing 56 patients treated with MISt using polyaxial PPS and 49 patients with open surgery.
Different techniques had been described to obtain fracture reduction in thoracolumbar burst fractures. Tezeren et al. 28 emphasized the importance of using a long-construct as he found that long-construct had better results in kyphotic correction, AVH ratio, and SC ratio compared to short-construct. Logroscino et al. 18 reported that careful patient positioning and proper rod contouring prior to its final positioning were two most important technical details to achieve fracture reduction using MISt. Blondel et al. 26 utilized a combination of kyphoplasty and MISt in their treatment of 29 patients with thoracolumbar fractures.
Classically, posterior surgeries utilize a distraction maneuver to restore vertebral height and provide indirect decompression of spinal canal by ligamentotaxis. 29 However, there is a disadvantage associated with MISt. Kumar et al. 23 had commented that some MISt systems can only be used with polyaxial screws to allow for screw angle variation. Attachment of the screw sleeves magnifies this angle, and this will interfere with rod passage. Due to its multidirectional screw head, the polyaxial screw used in these systems cannot be used as a fracture reduction tool. Palmisani et al. 30 found that the loss of correction during follow-up of patients treated with polyaxial screws could be due to movement between the head and the arm of the screw and, therefore, suggested that monoaxial screws should be used. However, the reduction technique in thoracolumbar fractures using monoaxial percutaneous screws was not fully elucidated.
In our study, we found that the reduction technique using monoaxial percutaneous screws (which were inserted at the adjacent vertebrae one level above and one level below the fracture) had better kyphotic reduction and higher restoration of AVH and PVH compared to polyaxial PPS screws technique. This technique used monoaxial PPS screws inserted parallel to the superior end plate of the adjacent vertebrae with the rods precontoured. Tightening of the screw nuts to the rods forms a 90°–90° screw-rod construct will allow anatomical reduction of the fractured vertebrae by restoring the kyphotic angle and AVH. A distractor was applied onto the extension sleeves of the monoaxial screws which allowed distraction to correct the PVH. Additional polyaxial PPS screws were placed one vertebra proximally and distally to act as neutralization system to strengthen the final construct.
The major limitation of our study was the technical difficulty in inserting the rods percutaneously into the monoaxial PPS construct. Malpositioning of the monoaxial PPS screws in the axial plane may lead to a difficult passage of the rod. Variation in the sagittal angulation of the screws between right and left side on the same vertebrae may lead to improper engagement of the nuts on the screw heads which may lead to implant loosening and nuts dislodgement. The monoaxial PPS screws should be placed parallel to the superior end plate to ensure good control of the fracture reduction. Poor screw position placement may lead to difficulty in controlling a symmetrical fracture reduction and thus lead to spinal malalignment. This technical difficulty and learning curve of this technique were not looked into. Secondly, this is a preliminary report of the surgical technique on percutaneous monoaxial PPS screws in thoracolumbar fracture reduction; therefore, only a small sample was included. This was one of the major limitations in this study. Thirdly, we did not assess the functional outcome of the patients during the follow-up period.
Conclusion
Posterior minimally invasive stabilization with monoaxial PPS reduction technique provided good kyphotic reduction and restoration of AVH and PVH with significantly better results compared to posterior minimally invasive stabilization using polyaxial PPS in the surgical treatment of thoracolumbar burst fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.