
Abstract
Keywords
Introduction
Thoracolumbar spine fracture is one of the common spinal fractures, no matter high energy trauma in adults or osteoporotic fracture in elderly, contributing to 90% of all spine fractures.1–3 Burst fractures comprise 14% of all spinal fractures. 4 For unstable fracture or in the case of neurological deficits, surgical decompression and stabilization are necessary.
Surgical stabilization aims to restore vertebral column stability, vertebral height, and correct angular deformity 5 for early mobilization. The treatment of choice of surgery is still controversial. A posterior approach is a commonly used approach. It can directly decompress the spinal canal through a transpedicular approach or laminectomy, or indirectly through ligamentotaxis.
A balance between good stabilization, risk of post-traumatic kyphosis, implant breakage, and vertebral motion is very important. In Cochrane systematic review 2013, Cheng et al. 6 concluded that evidence is insufficient to inform on a selection of different methods of pedicle screw fixation.
In a meta-analysis from ASJ 2017, 7 nine eligible trials with a total of 365 patients, it was concluded that the short segment pedicle screw fixation was not significantly different from long segment pedicle screws fixation in terms of correction of kyphotic deformity, back pain, and return to work.
However, there were studies8–11 showing loss of reduction with a high rate of implant failure in the short segment stabilization group.
While long segment instrumentation could provide multiple fixation points and sufficient corrective force to reduce and maintain reduction and prevent coronal or sagittal translation of disrupted vertebral segments. It could distribute corrective force over a greater number of segments and minimize the risk of pullout failure.12,13,14
A systematic review and meta-analysis 15 showed that a percutaneous procedure was superior in terms of postoperative pain, blood loss, operating time, hospitalization stay, and incision size. However, a minimal invasive surgery (MIS) procedure required more radiation exposure and more expensive instruments. There was also a risk of inadequate reduction and limited ability to maintain sagittal correction in face of axial instability. 8
There are more studies favouring the MIS approach recently.12,16,21 It is believed that, with minimal dissection of paraspinal muscles, the damage to the posterior ligamentous complex, which is essential for spinal stability, could be minimized. In addition, studies have shown less blood loss, shorter surgical time, decreased postoperative pain, shorter recovery time, and decreased muscle atrophy, but with a similar reduction in the MIS group.
The goal of this study is to compare percutaneous short segment and long segment stabilization over clinical and radiological parameters in this locality.
Objective
To compare the clinical and radiological outcomes of percutaneous short segment and long segment stabilization for patients with a thoracolumbar burst fracture.
Methodology
This study is a retrospective review and will be conducted in compliance with the Declaration of Helsinki.
Subjects
All included patients are those who had thoracolumbar burst fracture with percutaneous short or open long segment stabilization surgeries done in Alice Ho Miu Ling Nethersole Hospital and North District Hospital from June 2007 to 31 May 2020, and, in Prince of Wales Hospital from January 2014 to 31 May 2020.
Clinical, radiological and surgical data of all eligible patients are traced using information stored in medical records and Clinical Management System.
Inclusion criteria
Diagnosis of thoracolumbar burst fracture (T11-L3) with Type A2, A3, A4, B1, B2 and B3 in accordance with Arbeitsgemeinschaft fur Osteosynthesefragen (AO) classification.
Short segment pedicle instrumentation.
Open long segment pedicle instrumentation.
Minimum follow-up of 1 year.
Thoracolumbar injury severity score more than 3.
Exclusion criteria
Documented history of spine fracture or pre-existing kyphotic or scoliotic deformity and those treated with surgical stabilization using a posterior pedicle screw-based system.
Follow-up <1 year.
Pathological fracture.
History of fragility fracture, known osteoporosis, age >75 years old.
Short segment stabilization refers to the use of screws just at the level above and below fracture. It is further divided into minimally invasive percutaneous (MIS) fixation and open fixation groups for statistical analysis. For the long segment group, the stabilizations involve the use of screws extending to at least 2 levels above and below the injury level.
Data collection
This is a retrospective study on reviewing the existing medical records of eligible patients. No additional recruitments and other interventions or procedures will be performed for patients.
Patient's demographics and injury details (age, sex, body weight, smoking and drinking status) were collected and compared.
Radiological assessment
All patients had preoperative radiographs and computed tomography to evaluate fractures. Preoperative, immediate postoperative, postoperative 3 months, 6 months and 1 year radiographs were evaluated and radiological parameters were measured. It included vertebral wedge angle (defined as the angle between the upper endplate and lower endplate of the vertebra, Figure 1), anterior vertebral body height ratio (defined as the anterior vertebral height (AVH) of the fractured vertebra divided by the mean AVH of the segment above and below, Figure 2), posterior vertebral body height ratio (defined as the posterior vertebral height (PVH) of the fractured vertebra divided by the mean PVH of the segment above and below, Figure 2), and adjacent segment degeneration at postoperative 1 year (defined as a reduction of disc space >50% compared with the injury film).
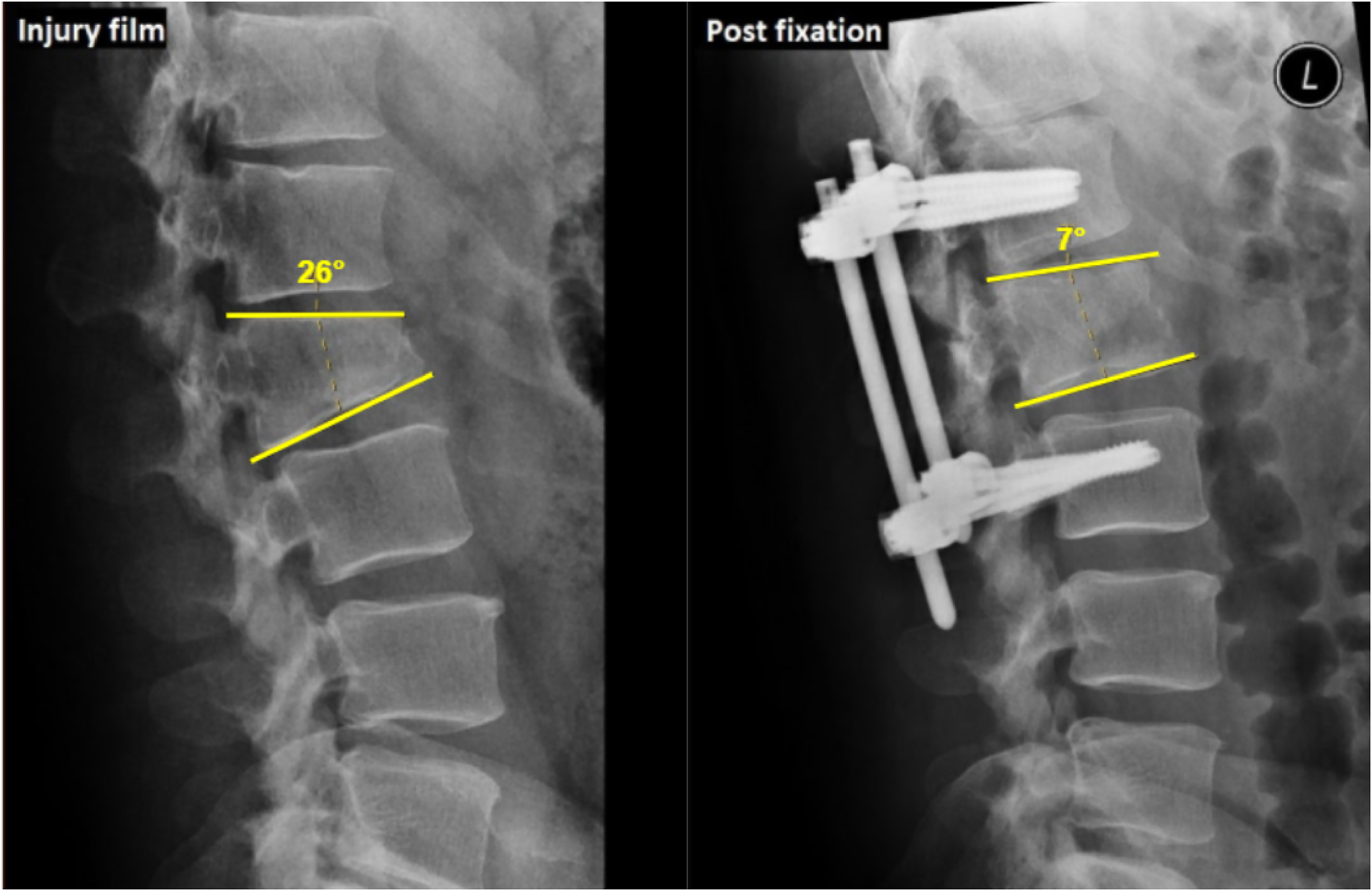
Vertebral wedge angle (defined as the angle between the upper endplate and lower endplate of the fractured vertebra).
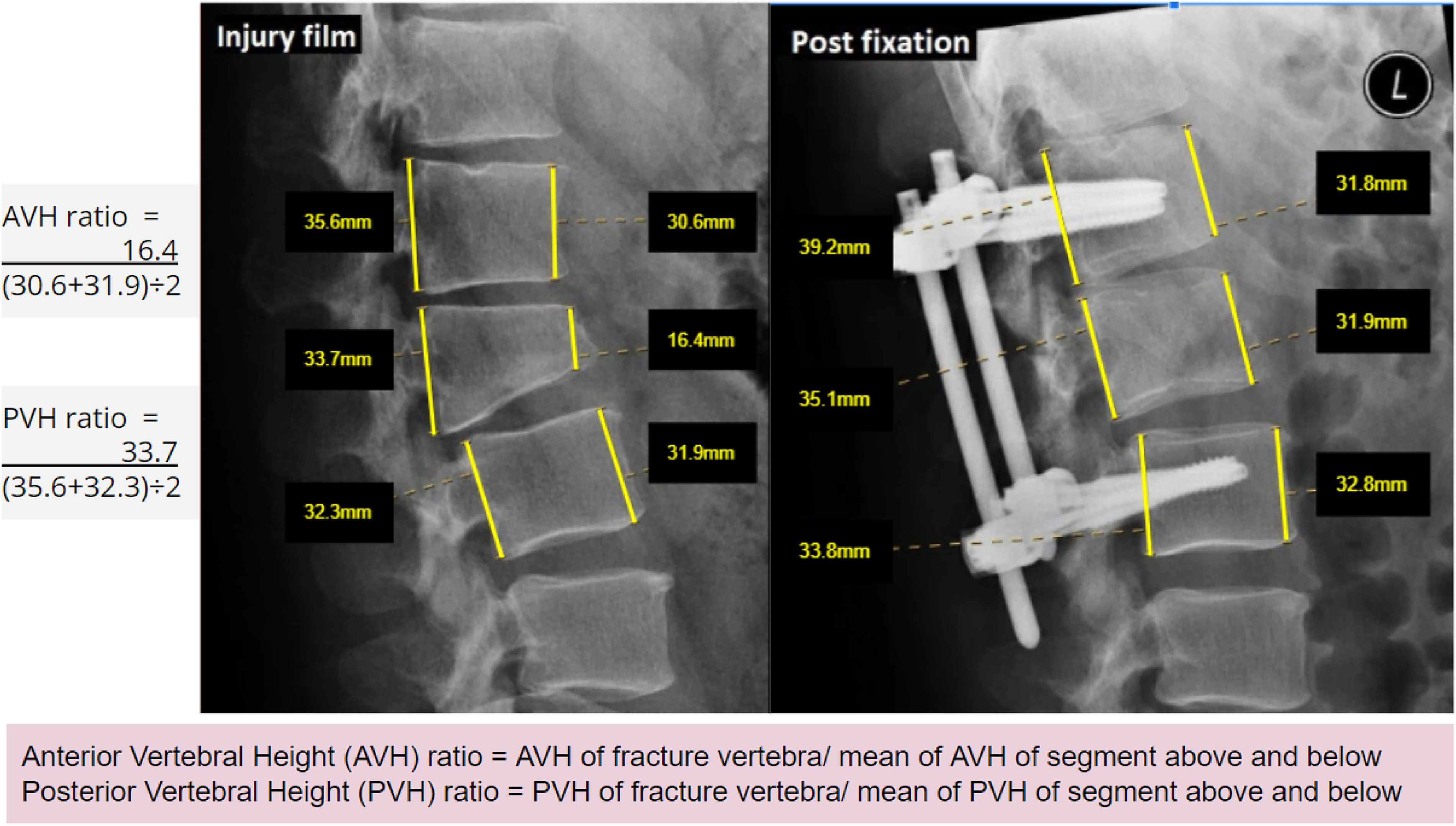
Anterior vertebral body height ratio (defined as the AVH of the fractured vertebra divided by the mean AVH of the segment above and below), posterior vertebral body height ratio (defined as the PVH of the fractured vertebra divided by the mean PVH of the segment above and below).
Clinical assessment
Operative parameters including operation time, amount of blood loss, postoperative length of stay, screw system, complications (infection, neurological deficit and implant failure), and need for removal of the implant were compared between two groups.
Clinical parameters including a visual analogue scale (VAS) for pain evaluation were assessed.
Statistical analysis
Descriptive statistics will be carried out for demographical data (age, sex, body weight, smoking, and drinking) and operative parameters (surgical time, intraoperative blood loss, postoperative length of stay, screw system, and need for removal of implant). Correlation between clinical outcomes (clinical parameters and radiological parameters) and demographics and operative parameters will be carried out using Student's t-test or chi-square test when appropriate. Complications will also be documented. Data analysis was carried out by IBM SPSS 25.0 (Armonk, New York). A two-sided p-value ≤0.05 was considered statistically significant.
Result
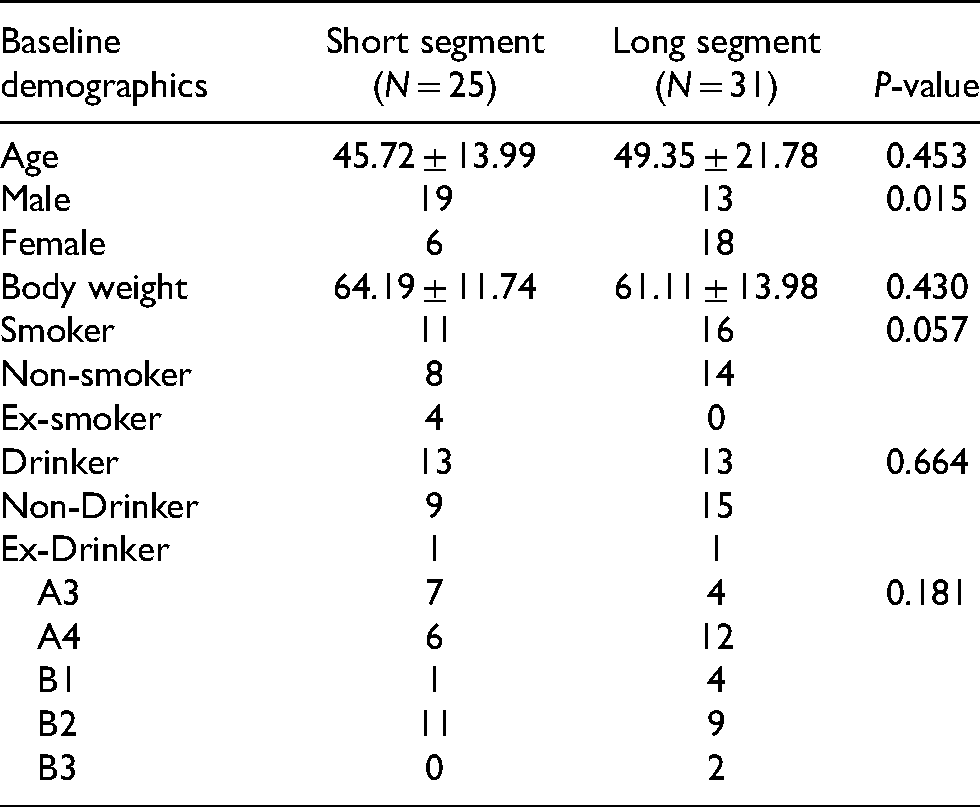
From June 2007 to May 2020, there were a total of 70 cases of a thoracolumbar burst fracture. Fifty-six cases fulfilled the inclusion criteria of this study. Of the 56 cases included (male = 31, female = 25), 25 patients underwent short segment stabilization (open = 11; MIS = 14) and 31 patients underwent long segment stabilization (open = 23; MIS = 8). The baseline demographics show that the female to male ratio is higher in the long segment group, while other parameters show no statistical difference between the two groups (Tables 1 and 2). There was no statistical difference in the distribution of fracture patterns in both groups. The mean follow-up is 39 months.
Demographics.
Result.
VAS: visual analogue scale; MIS: minimal invasive surgery; OT: operative time.
Short segment group versus long segment group
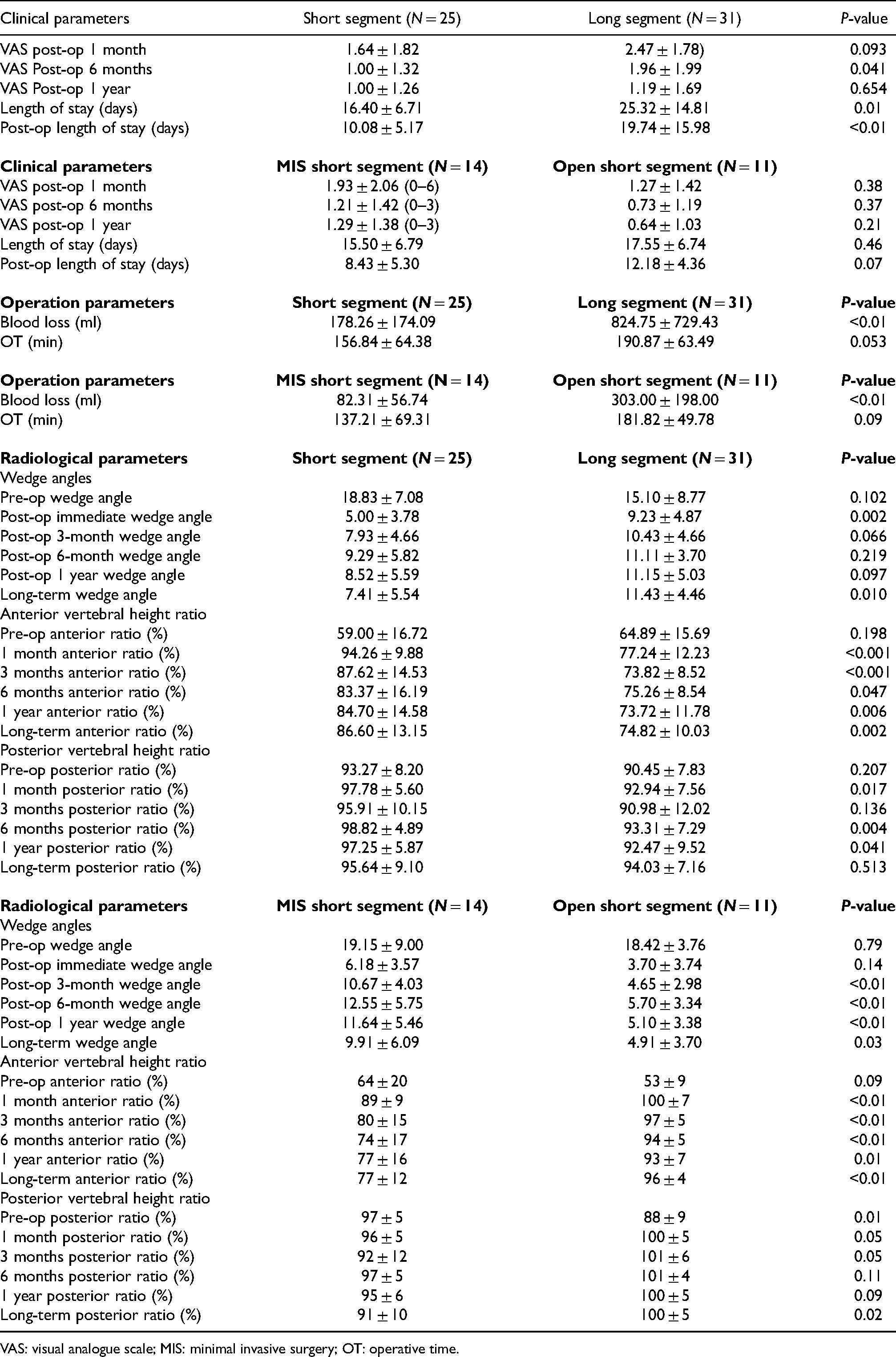
For clinical parameters, a better VAS was observed in the short segment group over 1 month, 6 months and 1 year post-operatively. The VAS score was statistically significant at 6 months post-operatively (1 vs. 1.96; p = 0.041). A shorter length of stay (16 days vs. 25 days; p = 0.01) and postoperative length of stay (10 days vs. 20 days; p < 0.01) were observed in the short segment group.
For operative parameters, there was significantly less blood loss (178 ml vs. 824 ml; p < 0.01) in the short segment group. Operative time was shorter in the short segment group but not statistically significant (157 min vs. 191 min; p = 0.053).
For radiological parameters, there was no statistical difference in preoperative wedge angle and AVH and PVH ratio in both short and long segment groups. Both groups showed statistically significant improvement in all parameters across the time.
The wedge angle was significantly smaller in the short segment group at immediate post-op (5° vs. 9.23°; p = 0.002) and long-term follow-up (7.41° vs. 11.43°; p = 0.01).
A short segment group also showed significantly better AVH ratio at immediate post-op (94% vs. 77%; p < 0.001), post-op 3 months (88% vs. 74%; p < 0.001), post-op 6 months (83% vs. 75%; p = 0.047), 12 months (85% vs. 74%; p = 0.006) and long-term follow-up (87% vs. 75%; p = 0.002).
The PVH ratio was significantly better in the short segment group at immediate post-op (98% vs. 93%; p = 0.017), post-op 6 months (99% vs. 93%; p = 0.004) and 12 months (97% and 92%; p = 0.041).
Open short segment group versus MIS short segment group
There was no significant difference in clinical parameters including VAS across time, length of stay (15.5 days vs. 17.5 days; p = 0.46) and post-op length of stay (8.4 days vs. 12.2 days; p = 0.07).
For operative parameters, there was significantly less blood loss in the MIS short segment group (82 ml vs. 303 ml; p < 0.01). The operating time was similar in both groups (137 min vs. 182 min; p = 0.09).
For radiological parameters, the wedge angle was significantly smaller in the open short segment group at post-op 3 months (4.6° vs. 10.7°; p < 0.01), post-op 6 months (5.7° vs. 12.6°; p < 0.01), post-op 12 months (5.1° vs. 11.6°; p < 0.01) and long-term follow-up (4.9° vs. 9.9°; p = 0.03; Figure 3).
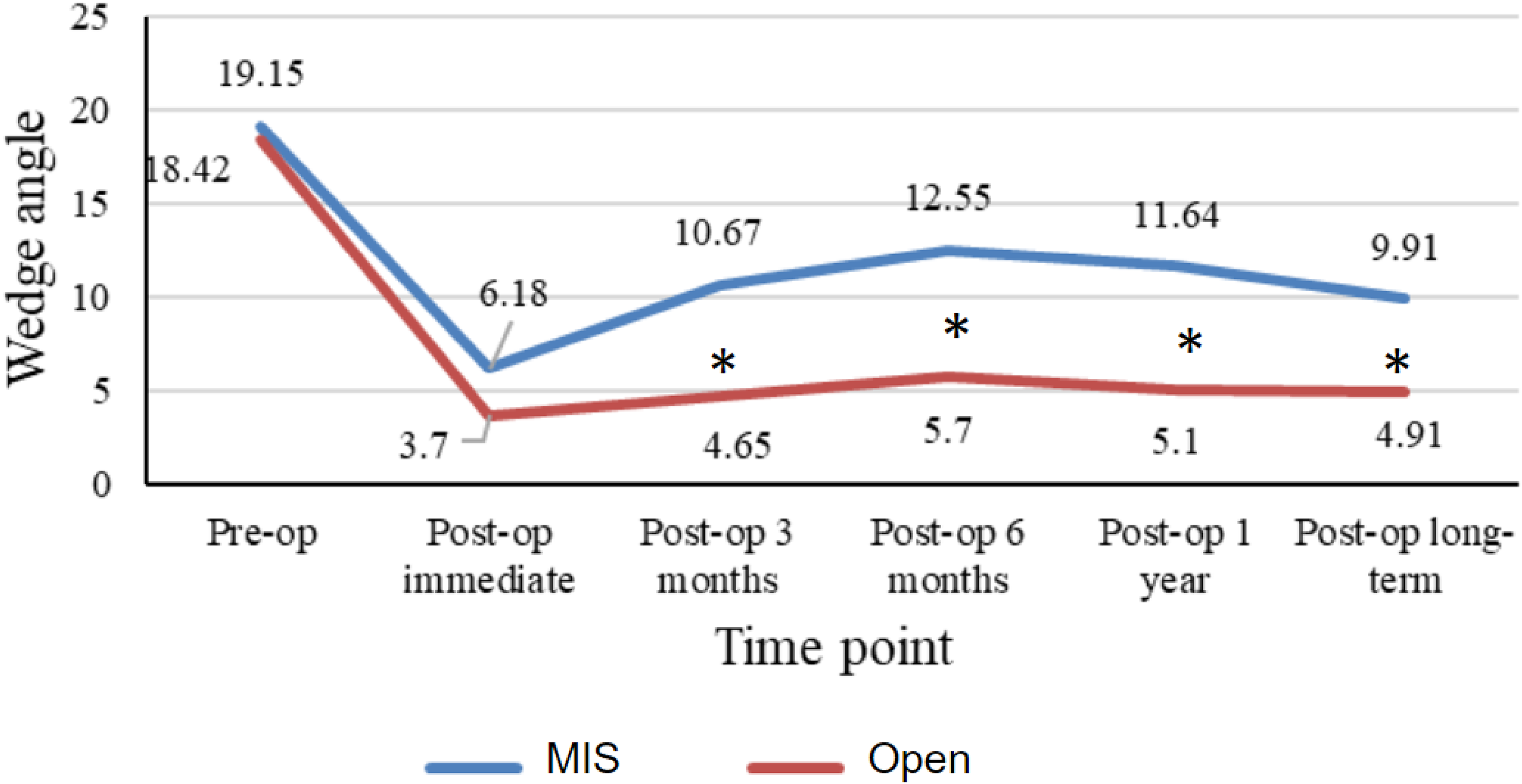
Diagram showing the wedge angle before and after operation for short segment group. *Comparison with statistical significance.
An open short segment group also showed significantly better AVH ratio at post-op 1 month (100% vs. 89%; p < 0.001), post-op 3 months (97% vs. 80%, p < 0.001), post-op 6 months (94% vs. 74%; p ≤ <0.01), 12 months (93% vs. 77%; p = 0.01) and long-term follow-up (96% vs. 77%; p < 0.01; Figure 4).
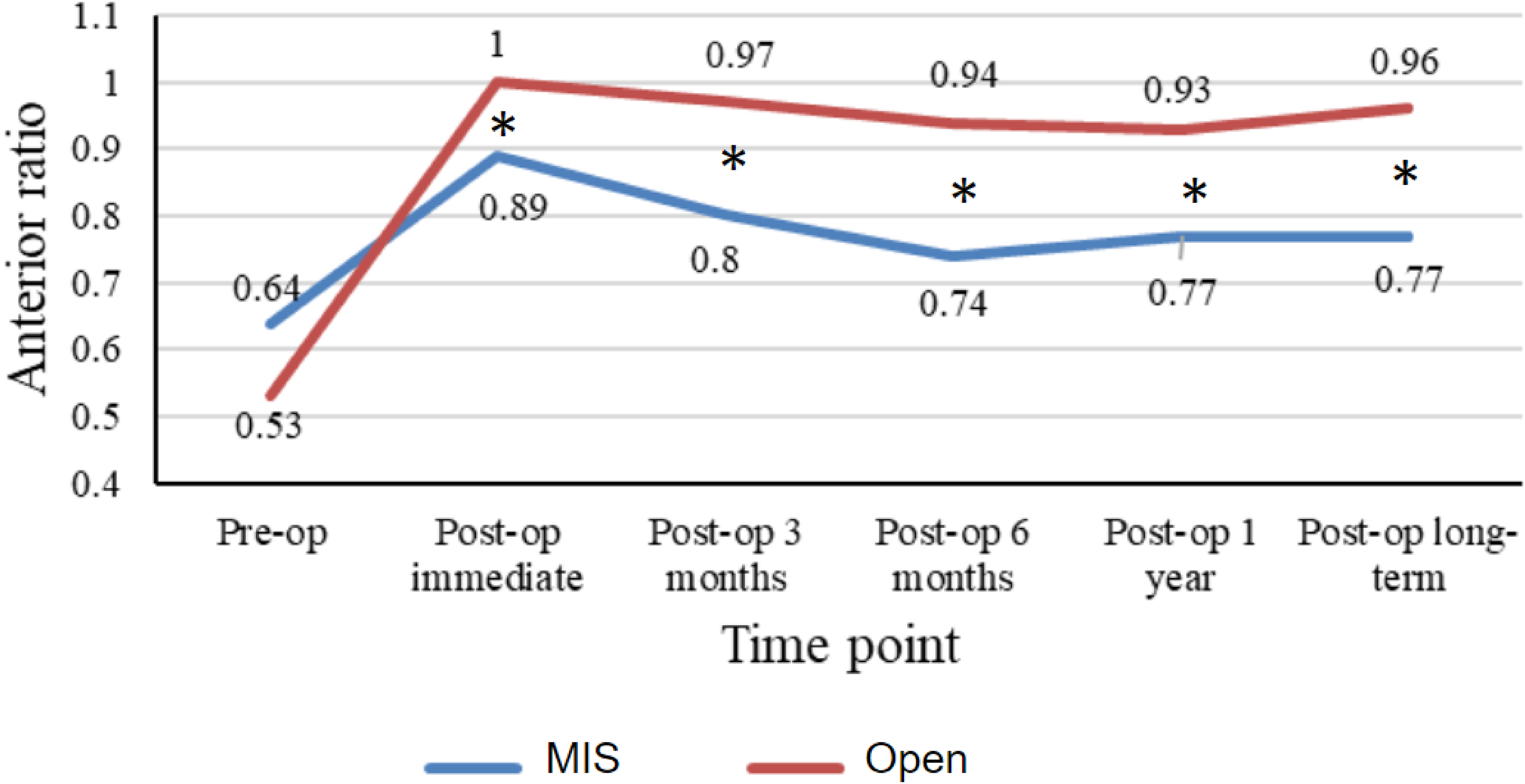
Diagram showing the anterior vertebral height (AVH) ratio before and after operation for short segment group. *Comparison with statistical significance.
A PVH ratio was also significantly better in the open short segment group at post-op 1 month (100% vs. 96%; p = 0.05), post-op 3 months (101% vs. 92%; p = 0.05) and long-term follow-up (100% and 91%; p = 0.02; Figure 5).
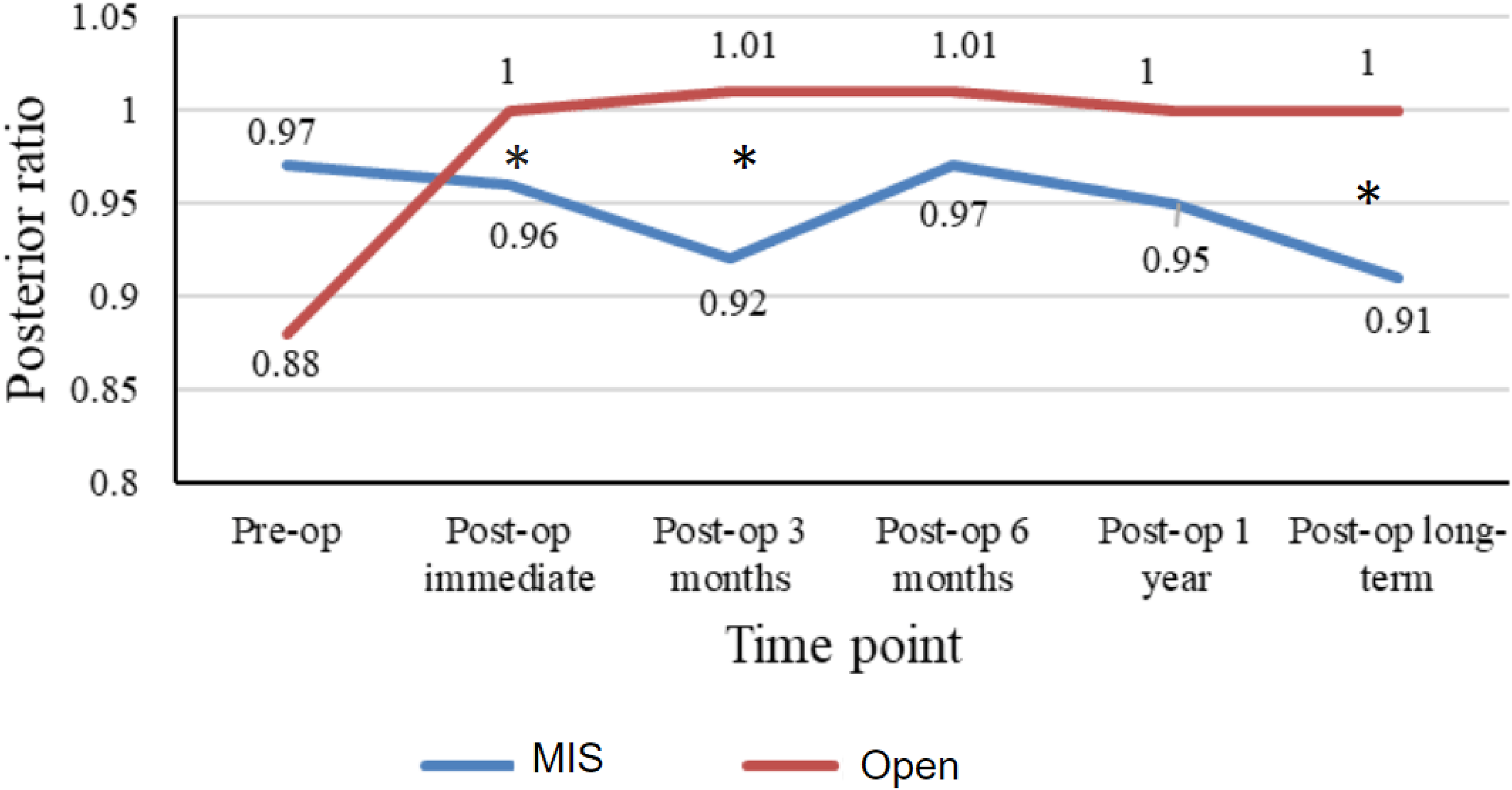
Diagram showing the posterior vertebral height (PVH) ratio before and after operation for short segment group. *Comparison with statistical significance.
Subgroup analysis of long and short segment groups over different fracture patterns
The short segment group showed statistically significantly better VAS at post-op 6 months and post-op 1 year, less intraoperative blood loss and shorter length in both AO type A and B fractures.
Radiological parameters were also statistically significantly better in the short segment group in AO type A and B fracture.
Absolute change in radiological outcome over time
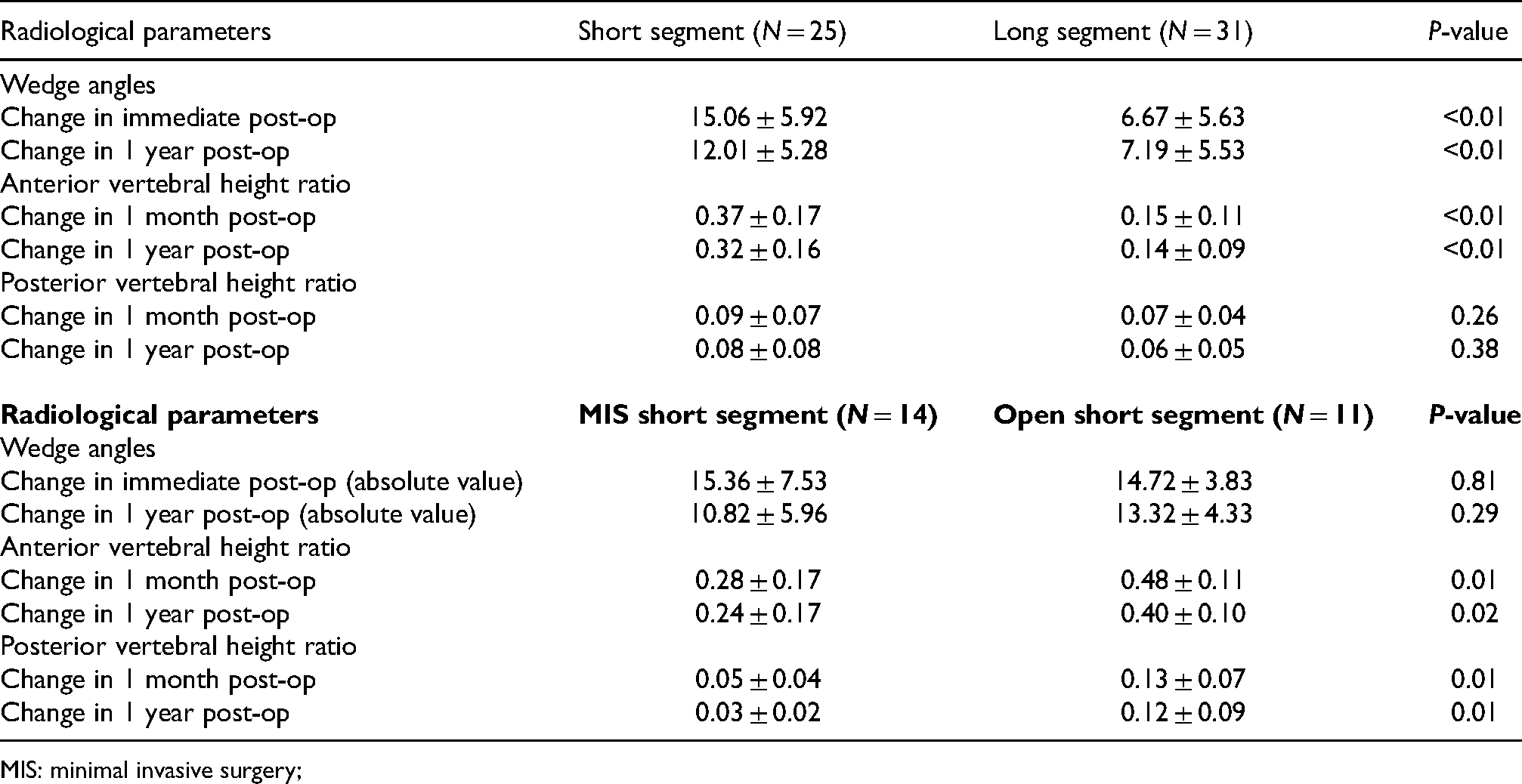
To compare the effectiveness in maintaining radiological reduction over time, the pre-op wedge angles were compared to the value at immediate post-op and post-op 1 year. The pre-op AVH and PVH ratios were compared to the value at post-op 1 month and post-op 1 year. There were significant differences in the change of radiological parameters within each group. There was a slight rebound in radiological outcomes at post-op 1 year in both the short and long segment group, as well as in the MIS short segment and open short segment group (Table 3, Figures 6–11).
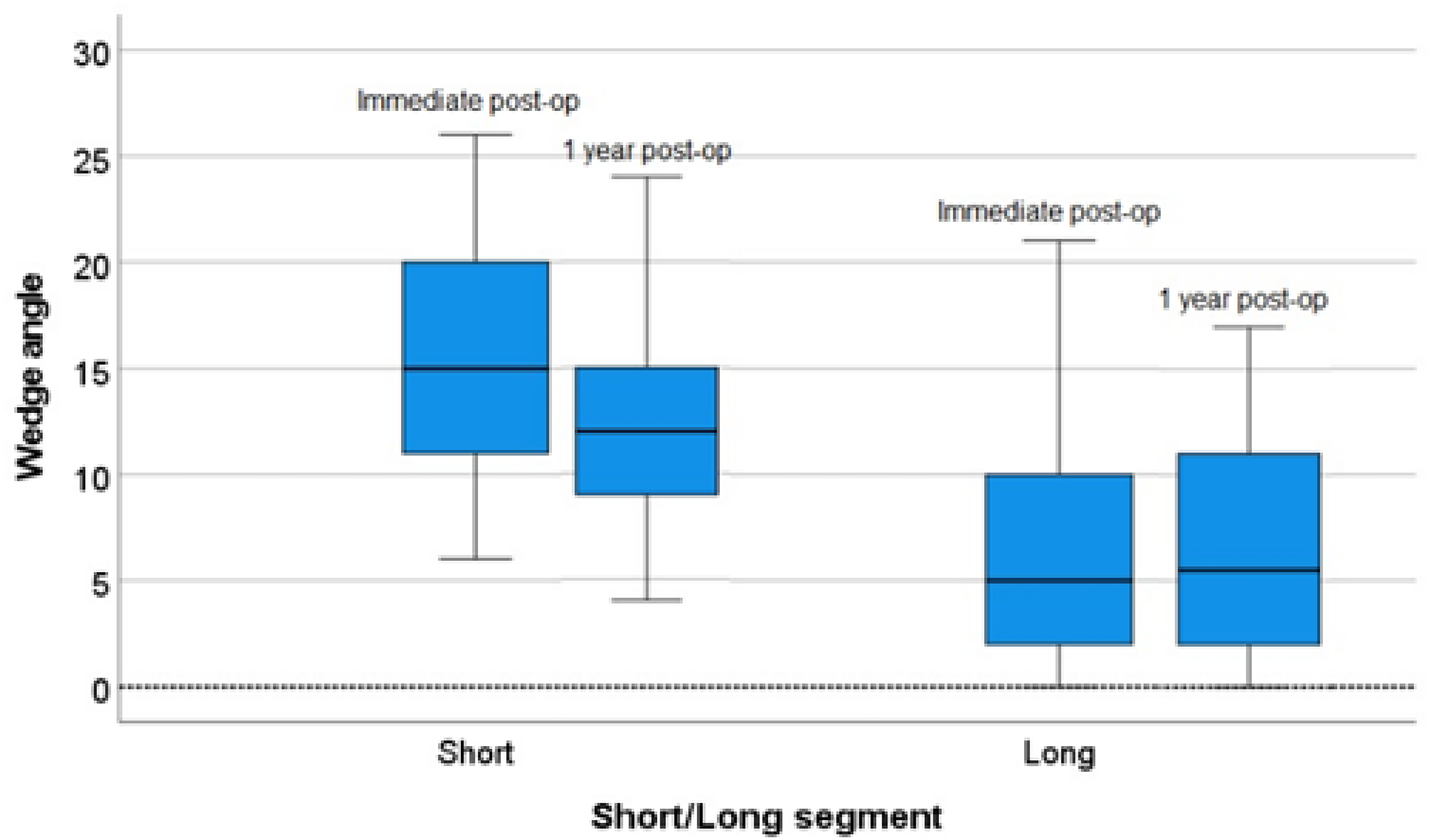
Box plot of the absolute change in (left) short segment (right) and long segment in wedge angle between immediate post-op and 1 year post-op.
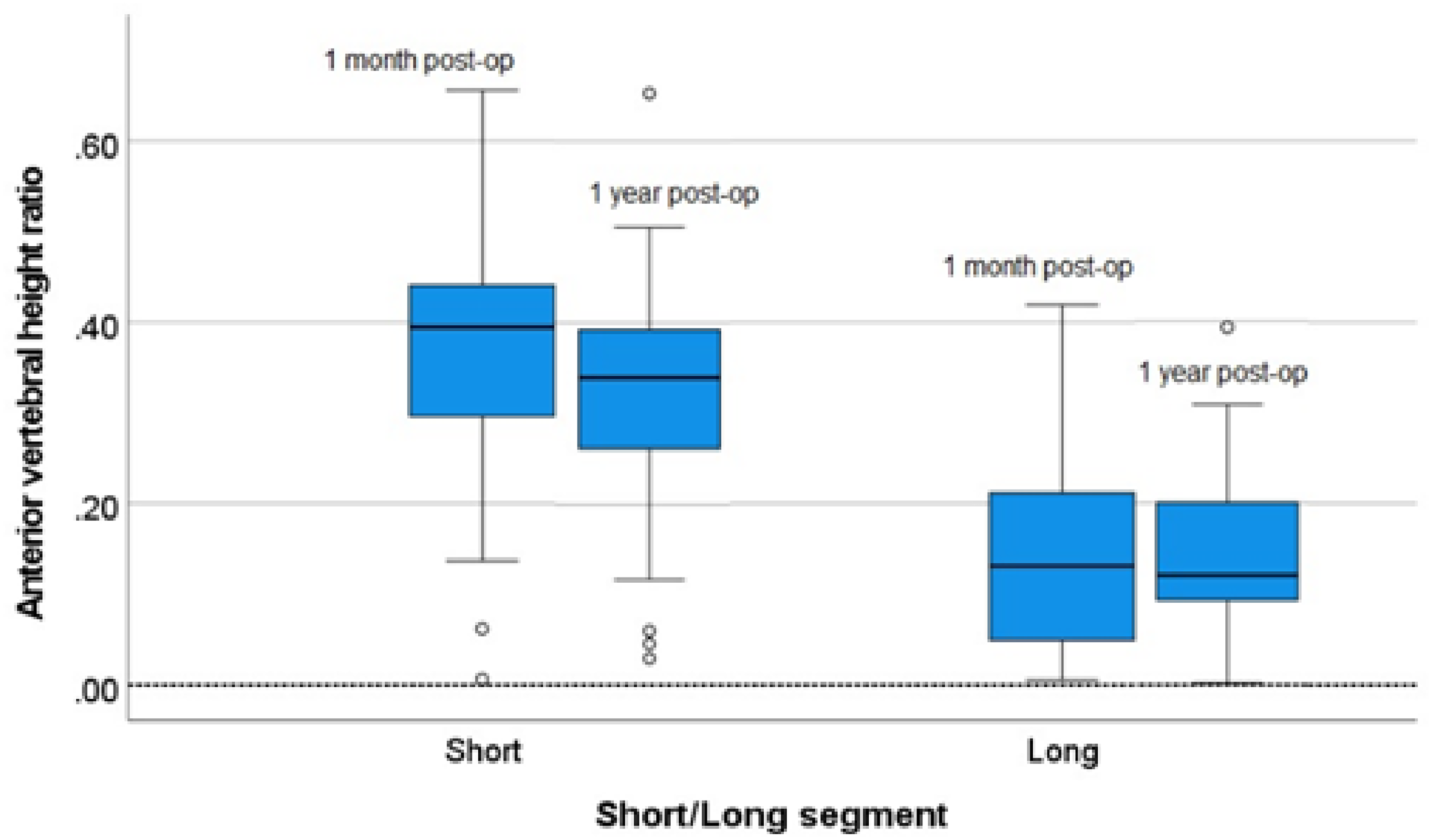
Box plot of the absolute change in (left) short segment (right) and long segment in anterior vertebral height (AVH) ratio between 1 month post-op and 1 year post-op. O: Outlier.
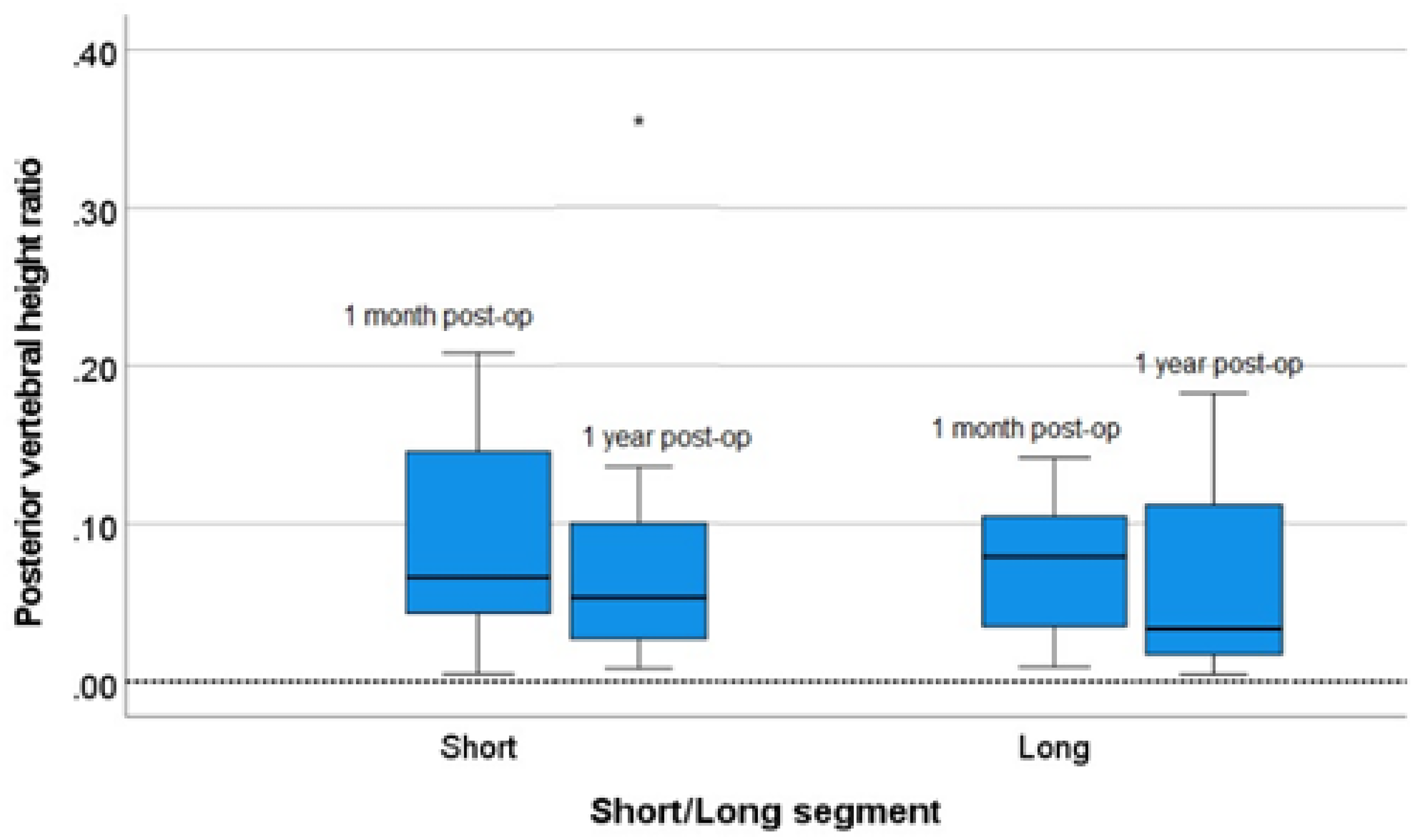
Box plot of the absolute change in (left) short segment (right) and long segment in the posterior vertebral height ratio between 1 month post-op and 1 year post-op. *Outlier.
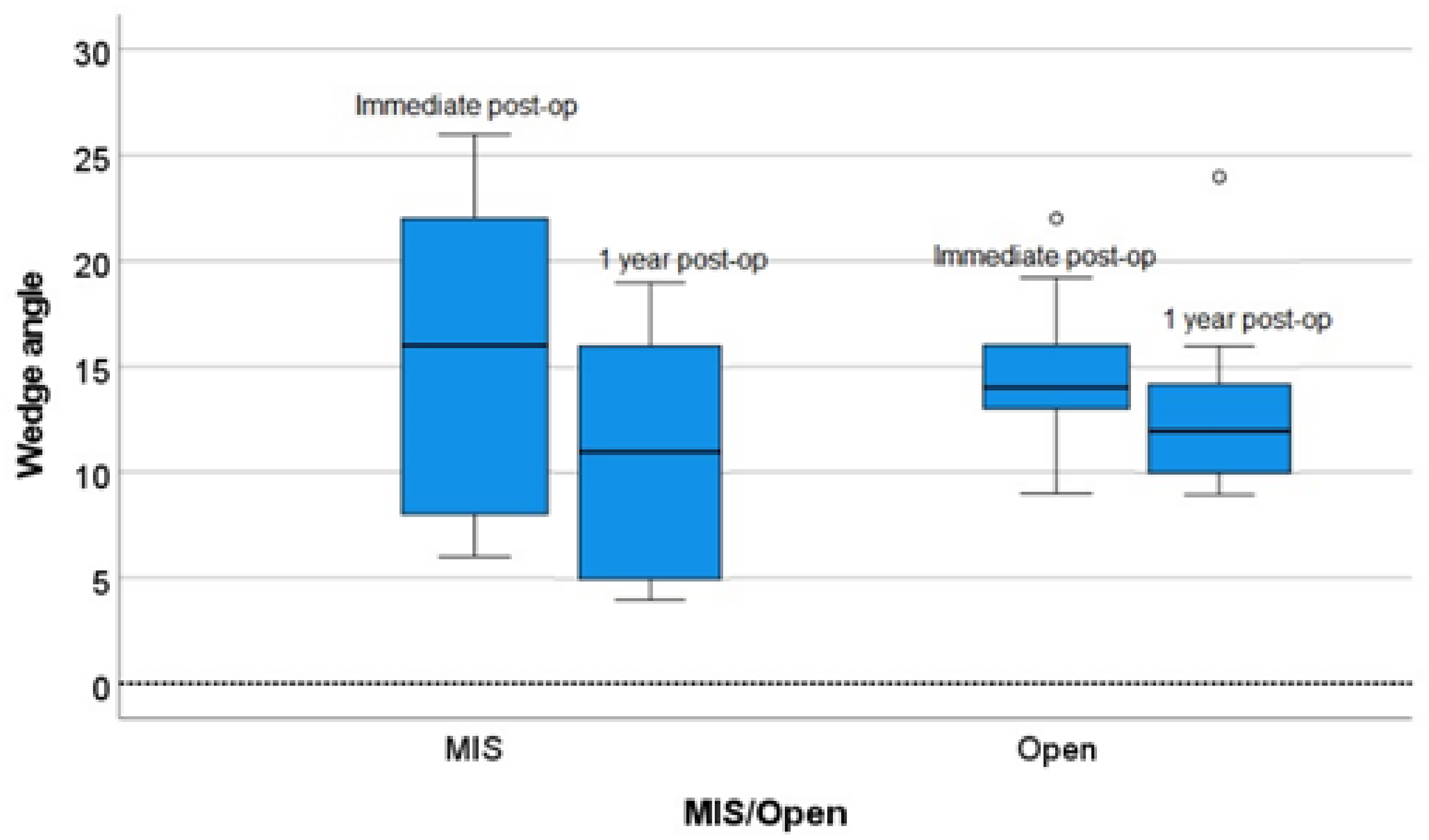
Box plot of the absolute change in (left) minimal invasive surgery (MIS; right) open in wedge angle between immediate post-op and 1 year post-op. O: outlier.
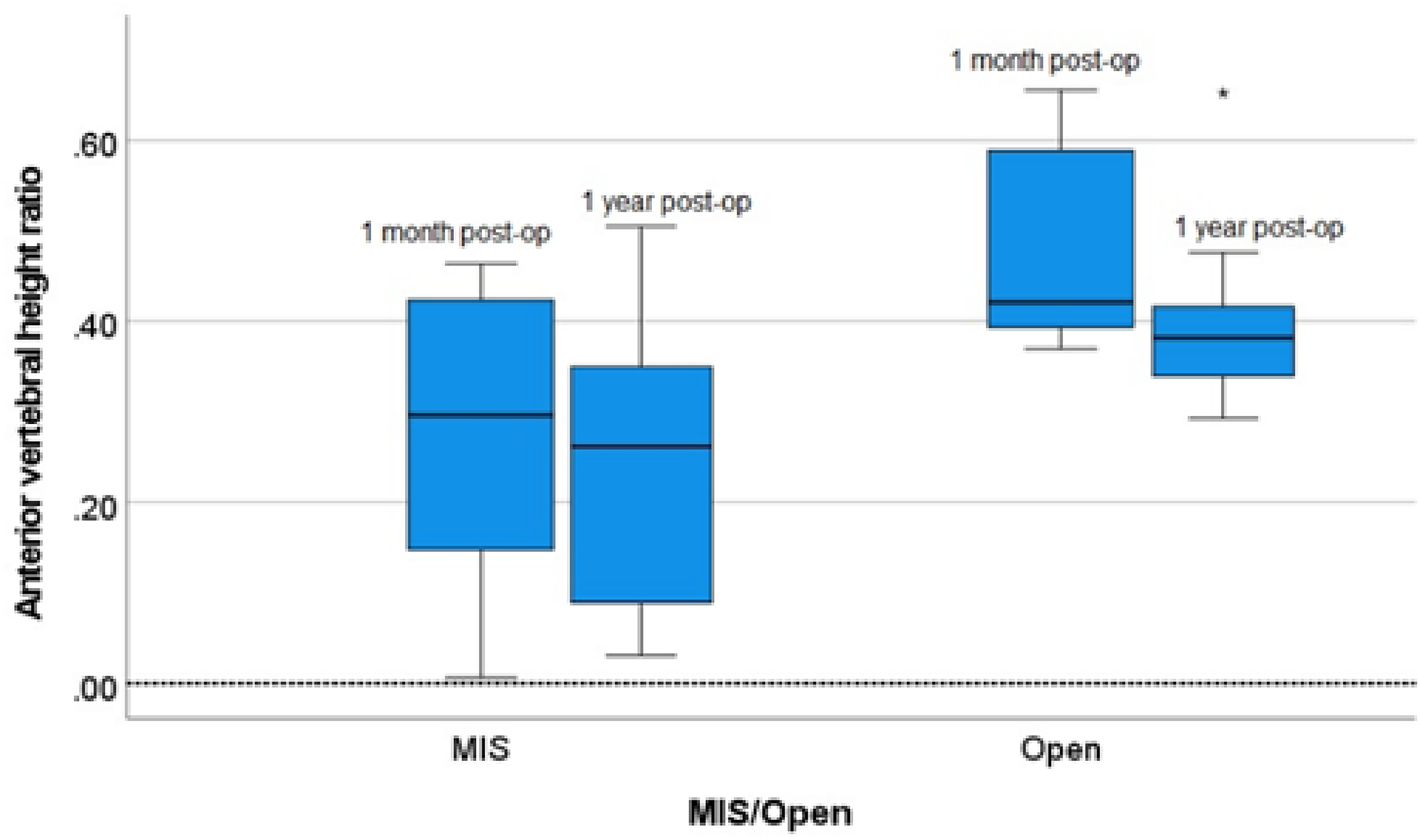
Box plot of the absolute change in (left) minimal invasive surgery (MIS; right) open in anterior vertebral height (AVH) ratio between 1 month post-op and 1 year post-op. *Outlier.
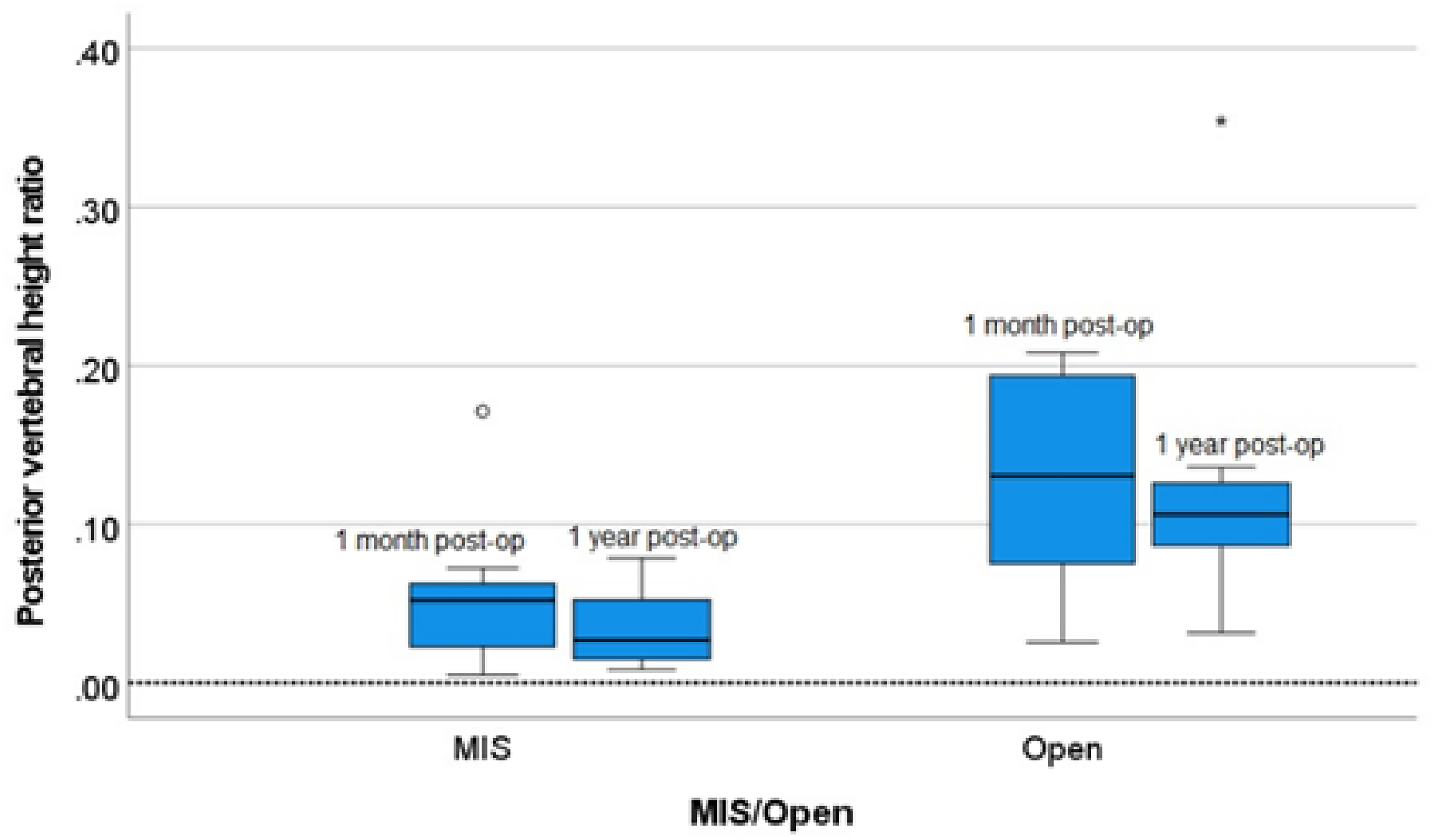
Box plot of the absolute change in (left) minimal invasive surgery (MIS; right) open in posterior vertebral height ratio between 1 month post-op and 1 year post-op. O: outlier.
Change in radiological outcome over time, comparing pre-op with immediate post-op/post-op 1 year.
MIS: minimal invasive surgery;
Overall
Superficial infection was seen in one patient after removal of the implant in the short segment group and no surgically related neurological injury were observed. No implant failure was seen in both groups.
No adjacent segment degeneration was seen in both groups one year after the operation.
Discussion
Dobran et al. 22 reviewed the outcome of 60 patients with unstable thoracolumbar burst fracture who underwent long or short segment fixation. There were 30 patients who underwent long segment fixation, while 30 patients underwent short segment fixation including screw at fracture level. The author reported similar kyphotic correction (local kyphosis angle) and sagittal alignment (AVH/PVH ratio) between the two groups. The short segment group also had the advantage of sparing 2 motion segments and the cost of implants.
In our study, the correlation of radiological parameters with clinical parameters was done by linear regression analysis. VAS score at post-op 12 months was negatively correlated with AVH and PVH ratios. In other words, the higher the AVH or PVH ratio, the lower the VAS.
Restoration of vertebral height can improve pain and hence daily function.
Cankaya et al. 23 concluded patients treated with short-segment posterior fixation have better sexual function and life quality with their partners compared to those treated with long-segment posterior fixation.
Moreover, subgroup analysis of the open and MIS short segment group showed interesting results. The MIS short segment group has significantly less blood loss but inferior wedge angle and vertebral ratio across time. We postulate that during the MIS short segment screw fixation, the Schanz screw might not be strong enough and the fracture clamp might be loosened by the interposed soft tissue. The MIS technique also prevents cross-link application.
We have further analysed the short segment group done by different implant systems, we found that the Universal Spine System (USS) (N = 17) and pedicle screw system (N = 8) both had similar blood loss, length of stay and post-op length of stay. The two groups were statistically better than the long segment group, respectively.
The AVH and PVH was better in the short segment USS group over time. The AVH was statistically better at immediate post-op, post-op 3 months, 12 months and long-term follow-up in the USS group, whereas the PVH was statistically better at post-op 6 months and long-term follow-up in the USS group. The wedge angle was also significantly smaller in the USS group at immediate post-op than in the long segment pedicle screw group.
The USS-based system seems to have better corrective power on kyphotic deformity with no inferior clinical and operative parameters.
Regarding the absolute change of radiological parameters over time, the long segment group (when compared with the short segment group) and the open short segment group (when compared with the MIS short segment group), were more effective in keeping the reduction of the wedge angle and AVH ratio. This could be contributed by the mechanical advantage of the construct.
A step further, we investigated the relationship between fracture patterns and type of fixation, the radiological parameters (wedge angle, AVH, and PVH) were statistically significantly better in the short segment group for thoracolumbar burst fractures A3, A4, B1 and B2.
The short segment group also showed less pain at post-op 6 months, less intraoperative blood loss and a shorter length of stay statistically in both AO type A and B fractures.
Short segment stabilization is not inferior to long segment stabilization in A3, A4, B1 and B2 burst fractures no matter from a clinical or radiological point of view. 24
In other words, one should offer short segment stabilization when a patient is suffering from A3, A4, B1 and B2 thoracolumbar spine traumatic fracture with no neurological deficit, osteoporosis and pre-existing spinal deformity or surgery.
There are biomechanical and clinical studies supporting short segment pedicle screw fixation with an intermediate screw.25,26
A meta-analysis study 27 evaluated 23 publications and concluded that the fixation method consisting of 2 levels above and 1 below with intermediate screws for the thoracolumbar burst fractures showed the highest correction of kyphosis angle both at immediate and final follow-up and also the lowest implant failure at final follow-up. 28
In a recent systematic review article reviewing 8 biomechanical studies on techniques of spine reconstructions in traumatic spinal injuries, 25 the author concluded that short segment posterior fixation (1 level above and 1 level below) with screws at the fracture level may improve construction stiffness and can even be compared with long-segment fixation or circumferential reconstruction in, for example, thoracolumbar burst fracture.
A recent review in 2020 29 concluded posterior segment instrumentation is sufficient for almost all type A and B fractures in a non-ankylosed spine. There might be a slight recurrence of kyphosis but the clinical implant is minimal. The author also points out that index-level screws (screws in the fractured vertebra) increase the effectiveness of short segment instrumentation and substantially decrease the implant failure rate.
Index-level screw seems to be a good strategy to counter short segment instrumentation failures30,31.
The limitation of this study includes an intraobserver error, small sample size and quality of x-ray. The centre of the x-ray beam was not always focusing on the injury level, which might affect the measurement. AVH and PVH ratios were henced adopted to improve the accuracy of the radiological measurement.
Furthermore, there were more females in the long segment group, which may be a confounding factor for the analysis as epidemiologically female has a higher chance of having undiagnosed osteoporosis or osteopenia, which could lead to inferior outcome.
Conclusion
For single-level thoracolumbar fracture, both long and short stabilizations were effective in reducing and stabilizing the fracture. However, the short segment group showed significantly superior results in both clinical and radiological parameters. Moreover, using minimally invasive techniques in short segment stabilization showed even less blood loss compared with the open approach, but a less optimal radiological outcome. Therefore, short segment stabilization could be the treatment of choice for traumatic thoracolumbar spine fractures in patients with no neurological deficit, no osteoporosis and no pre-existing spinal deformity or surgery.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.