
Abstract
Study Design
Retrospective cohort study.
Objectives
This study aims to analyze outcomes and complications of patients with thoracic and lumbar fractures in the setting of ankylosing spinal disorders (ASD) treated with minimally invasive surgery (MIS).
Methods
The operative logs from 2012 to 2019 from one academic, Level I trauma center were reviewed for cases of thoracic and lumbar spinal fractures in patients with ASD treated with a MIS approach. Variables were compared between patients with ankylosing spondylitis (AS), diffuse idiopathic skeletal hyperostosis (DISH), and advanced spondylosis.
Results
A total of 48 patients with ASD and concomitant thoracic or lumbar spinal fracture managed with an MIS approach were identified. A total of 11 patients were identified with AS, 21 with DISH, and 16 with advanced spondylosis. A total of 27 (56.3%) patients experienced complications. Complications differed between groups; DISH patients experienced a greater number of post-operative complications compared to AS and advanced spondylosis patients (P = .009). There was no significant difference in length of surgery, estimated blood loss, length of stay, readmission, and reoperation rates between AS and DISH patients. There were 3 mortalities unrelated to the surgery.
Conclusion
Percutaneous stabilization of patients with ankylosing spinal disorder fractures remains a viable management method. Operative characteristics were similar between AS, DISH, and advanced spondylosis patients; however, DISH patients experienced a greater number of post-operative complications.
Keywords
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) and ankylosing spondylitis (AS) are the 2 main ankylosing disorders affecting the spine. 1 These disorders produce bony proliferation in the spine as well as the extraspinal entheseal sites, which lead to limitations of spinal mobility and postural abnormalities.2,3 DISH is a non-inflammatory disorder characterized by calcification and ossification of ligaments, entheses, and other soft tissues, which can be seen in one or multiple segments of the spine, but is more common in the thoracic spine.2,4,5 In contrast, AS is a systemic chronic spondyloarthropathy that primarily affects the axial spine. 6 In addition, AS is also characterized by fusion of the SI joints, and in contrast to DISH which tends to affect older individuals, AS begins in adolescence or young adult life. 4
These ankylosing spine disorders (ASD) result in the formation of a stiff spine with long lever arms, making patients increasingly susceptible to injury, even after minor trauma. 7 Traditionally, these patients are operatively managed with open instrumented fusions. 8 However, standard open techniques are often morbid and associated with large blood loss, increased operative time, and higher wound-related complications such as infections. 9 Therefore, minimally invasive spine surgery has gained popularity when managing patients with these complex spine disorders.10-13
AS and DISH are often thought of as one entity; however, these disorders differ in terms of outcomes, number and type of surgical complications, and mortality rates in the conventional open approach. 14 However, to date there has been no comparison of how AS or DISH may impact complications and outcomes following MIS fixation. The goal of this study was to analyze outcomes and complications of patients with thoracic and lumbar fractures in the setting of ASD treated with minimally invasive surgery.
Methods
Patient Selection
After obtaining Institutional Review Board (IRB) approval (HP-00082698), we retrospectively reviewed all patients at our institution sustaining thoracic or lumbar spine fractures from 2012 to 2019. We followed the Strengthening the Report of Observational Studies in Epidemiology (STROBE) Guidelines to assure high quality of our study.
15
The patient sample was identified from a surgical billing database querying for current procedural terminology (CPT) and International Statistical Classification of Diseases and Related Health Problems (ICD) codes to identify patients with thoracic or lumbar spinal fractures. Using preoperative imaging, patients were identified as having either DISH, AS, or advanced spondylosis by both a fellow and a fellowship-trained physician. AS was defined as patients with bilaterally sacroiliac erosion and vertebral scalloping using the radiographic criteria of the modified New York criteria.
16
The modified New York criteria includes 3 additional clinical criteria (1) lumbar back symptoms improved with activity for at least 3 months, (2) limited range of motion in forward and lateral bending of the lumbar spine, and (3) limited chest wall expansion. It was not feasible to include the clinical criteria in the retrospective chart review. The DISH group was identified using criteria established by Resnick and Niwayama, presence of non-marginal syndesmophytes at 4 consecutive vertebrae without significant intervertebral disc high loss or ankylosis of the facet joints.
17
Advanced spondylosis was defined as patients with advanced degenerative changes with bridging or kissing osteophytes who did not meet the radiographic criteria for AS or DISH. Figure 1 illustrates examples of AS, DISH, and advances spondylosis on sagittal CT imaging. Patients who did not meet the criteria for AS, DISH, or advanced spondylosis were excluded. Procedures were performed by 1 of 4 fellowship-trained orthopaedic spine surgeons at a single Level 1 trauma and academic institution. Sagittal CT imaging of AS, DISH, and advanced spondylosis. Illustrating vertebral scalloping in AS (left), anterior syndesmophytes at consecutive vertebrae without significant intervertebral disc high loss or facet joint ankylosis in DISH (center), and advanced degenerative changes with kissing osteophytes in advanced spondylosis (right).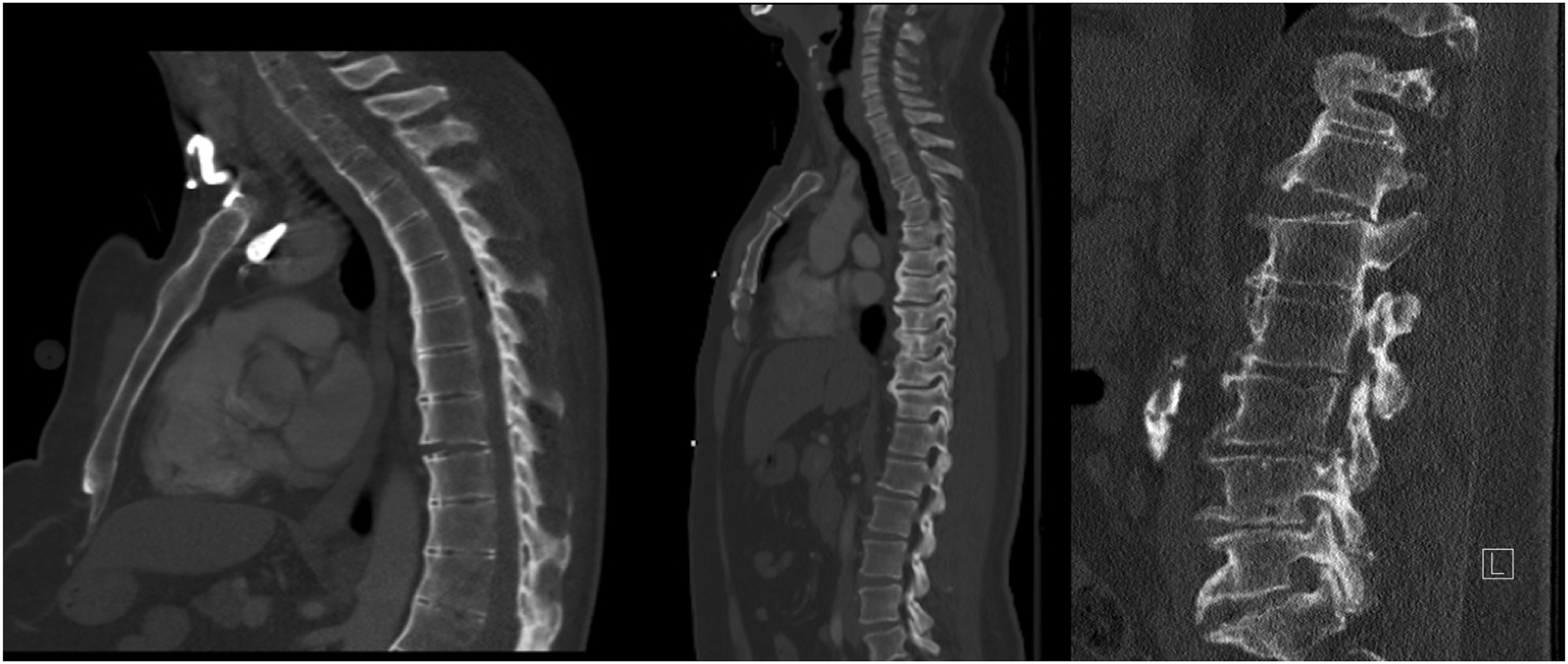
Surgical Technique
After administration of general endotracheal anesthesia, patients were positioned prone onto an open Jackson table, and all bony prominences were padded. Jamshidi needles were navigated across the pedicle while keeping the tip of the needle lateral to the medial boarder of the pedicle until a depth of at least 20 mm had been achieved. Lateral fluoroscopy images were obtained to check placement within the pedicle and depth in the vertebral body. Guidewires were then placed through the cannulated Jamshidi needles. The pedicles were then tapped 1 mm smaller in diameter than the planned screw to be placed followed by placement of the appropriately sized pedicle screws. Screw placement was confirmed fluoroscopically followed by placement of subfascial rods into the pedicle screws. The rods were secured to the screws with locking caps.
Multiple factors influence the number of instrumented levels included in the surgical construct. These factors include the facture pattern, degree of displacement, bone quality, intraoperative pedicle visualization, pedicle screw purchase, and a patient’s intraoperative physiologic stability. Figure 2 illustrates a typical surgical construct in a patient with advanced spondylosis. Radiographs demonstrating a typical surgical construct in a 90-year-old male with advanced spondylosis. Preoperative crossable lateral radiograph (left). AP (center) and lateral (right) radiographs of T10-L2 posterior fusion.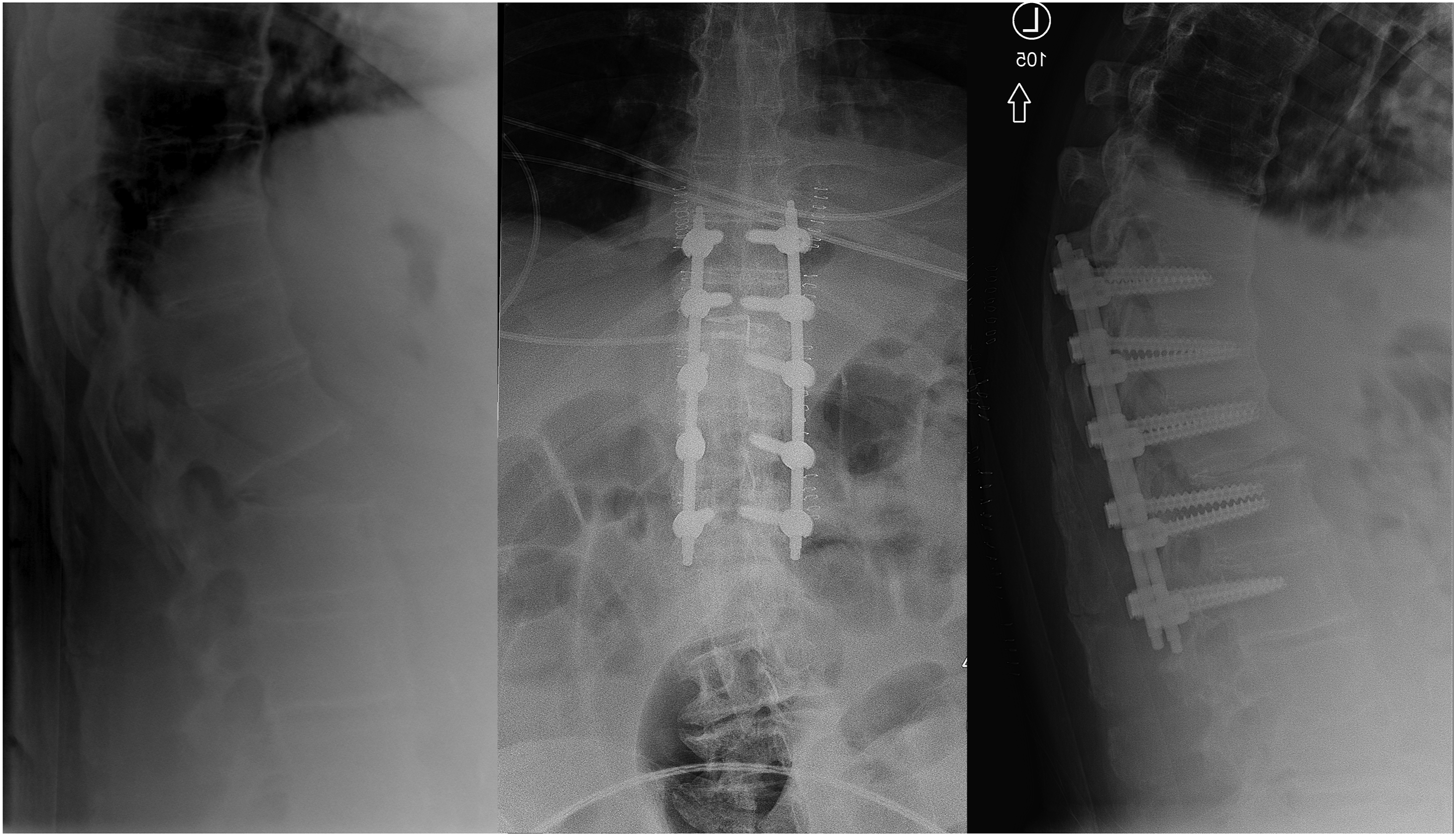
Outcomes
Our primary outcomes were perioperative characteristics including blood loss, surgical time, and intraoperative blood transfusions. Secondary outcomes measured were peri-operative complications and reoperations.
Data Collection
Retrospective chart review was performed by 2 research assistants from the inpatient and outpatient medical records. Patient demographic information included: age, gender, BMI, and discharge facility. We collected perioperative variables from operative notes and anesthesia reports, including surgical approach, operative procedure, length of surgery, estimated blood loss, intraoperative blood transfusions, and in-hospital post-operative complications. Additionally, we retrieved mechanism of injury, spine fracture level, in-hospital post-operative complications, neurological status at initial evaluation, Charlson’s Comorbidity Index (CCI), American Society of Anesthesiology (ASA) score, length of stay, ICU length of stay, readmission, and reoperation data.
Data Analysis
JMP® Pro (Version 13.0.0; SAS Institute Inc, Cary, NC, 1987-2007) was used for descriptive statistics. Mean, standard deviation, and 95% confidence interval (CI) were calculated for continuous variables along with frequencies for ordinal and nominal variables. Significance level was set at P < .05. Continuous variables were tested for normality with the Shapiro–Wilk test. Analysis of variance (ANOVA) test was used to evaluate continuous variables with normal distribution, and a non-parametric Kruskal–Wallis test was used for non-normally distributed continuous variables. Fisher’s exact test or Pearson’s chi-square test were used to evaluate categorical dependent variables.
Results
Patient Characteristics Between AS and DISH Trauma.
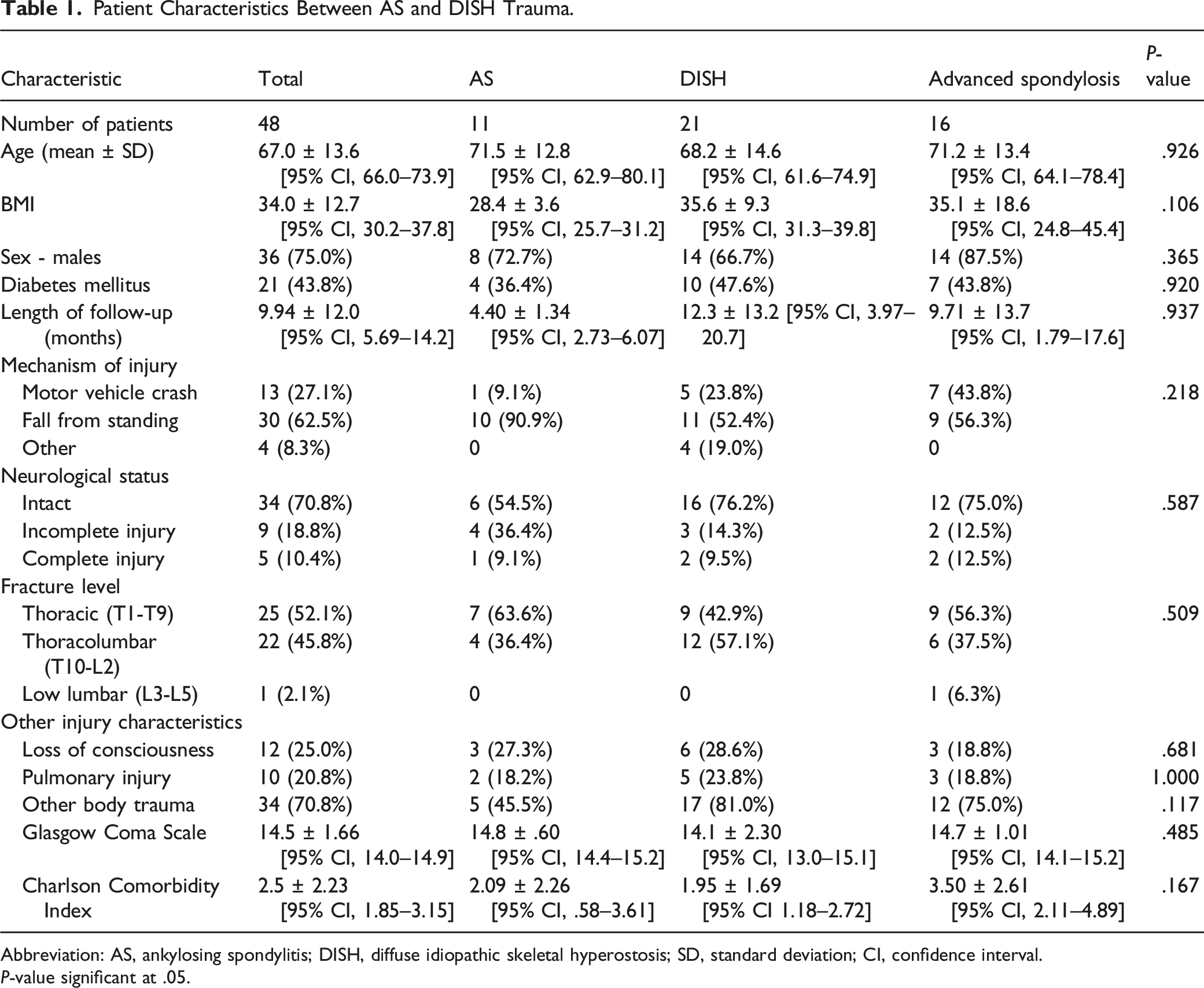
Abbreviation: AS, ankylosing spondylitis; DISH, diffuse idiopathic skeletal hyperostosis; SD, standard deviation; CI, confidence interval.
P-value significant at .05.
The majority of patients’ mechanism of injury was from a fall from standing (62.5%, n = 30), with motor vehicle crashes being the second most common mechanism of injury (27.1%, n = 13). There was no significant difference in mechanism of injury observed between groups (P = .218). Across all 3 cohorts, 70.8% of the patients (n = 34) did not have a neurologic deficit. In the AS group 54.5% (n = 6), in the DISH group 76.2% (n = 16), and in the advanced spondylosis group 75.0% of the patients (n = 12) did not have a neurologic deficit (P = .587). Injuries occurred within the thoracic (AS: n = 7, 63.6%; DISH: n = 9, 42.9%; advanced spondylosis : n = 9, 56.3%) and thoracolumbar (AS: n = 4, 36.4%; DISH: n = 12, 57.1%; advanced spondylosis : n = 6, 37.5%) zones, with no difference between cohorts (P = .509). Other characteristics including loss of consciousness, concomitant injury, and CCI were not significantly different between the cohorts (Table 1).
Operative Characteristics between AS and DISH Trauma.
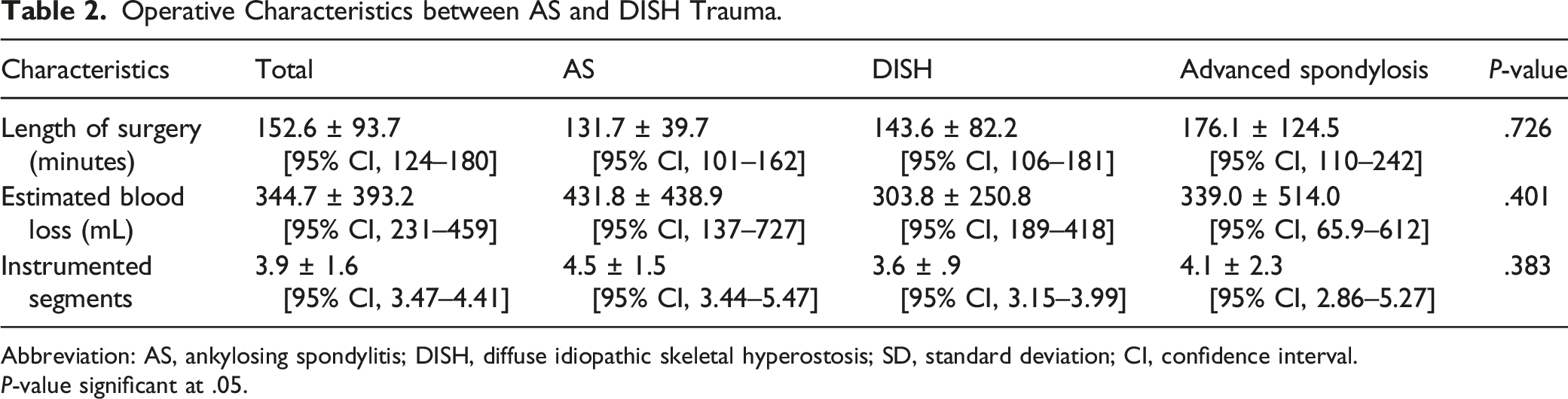
Abbreviation: AS, ankylosing spondylitis; DISH, diffuse idiopathic skeletal hyperostosis; SD, standard deviation; CI, confidence interval.
P-value significant at .05.
Hospital Stay Characteristics between AS and DISH Trauma.
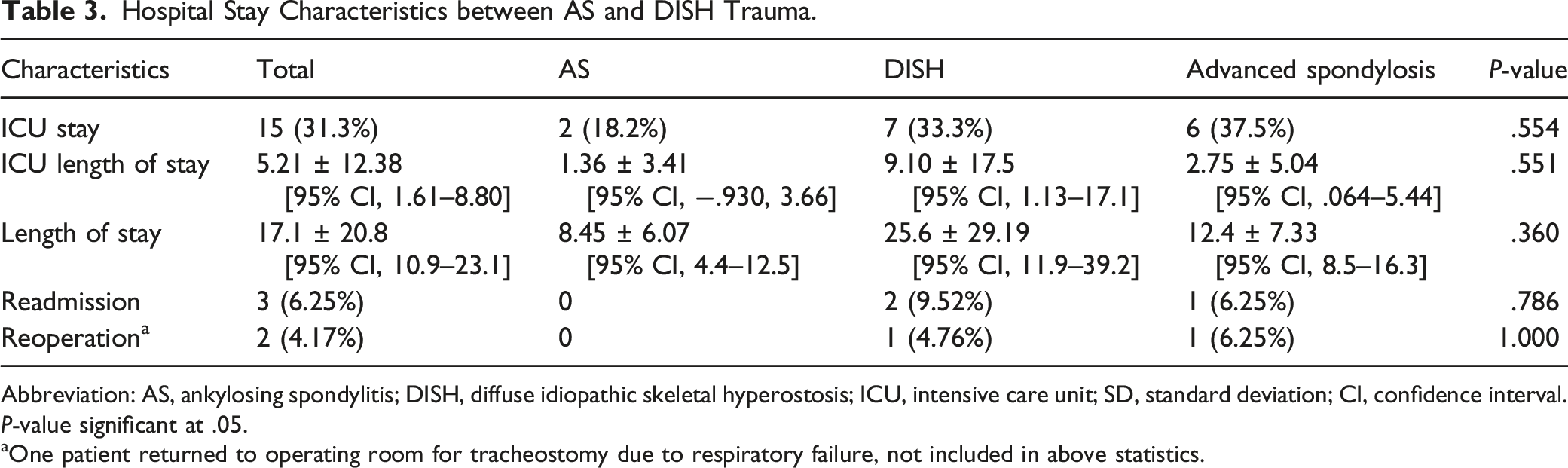
Abbreviation: AS, ankylosing spondylitis; DISH, diffuse idiopathic skeletal hyperostosis; ICU, intensive care unit; SD, standard deviation; CI, confidence interval.
P-value significant at .05.
aOne patient returned to operating room for tracheostomy due to respiratory failure, not included in above statistics.
Complications between AS and DISH Trauma.
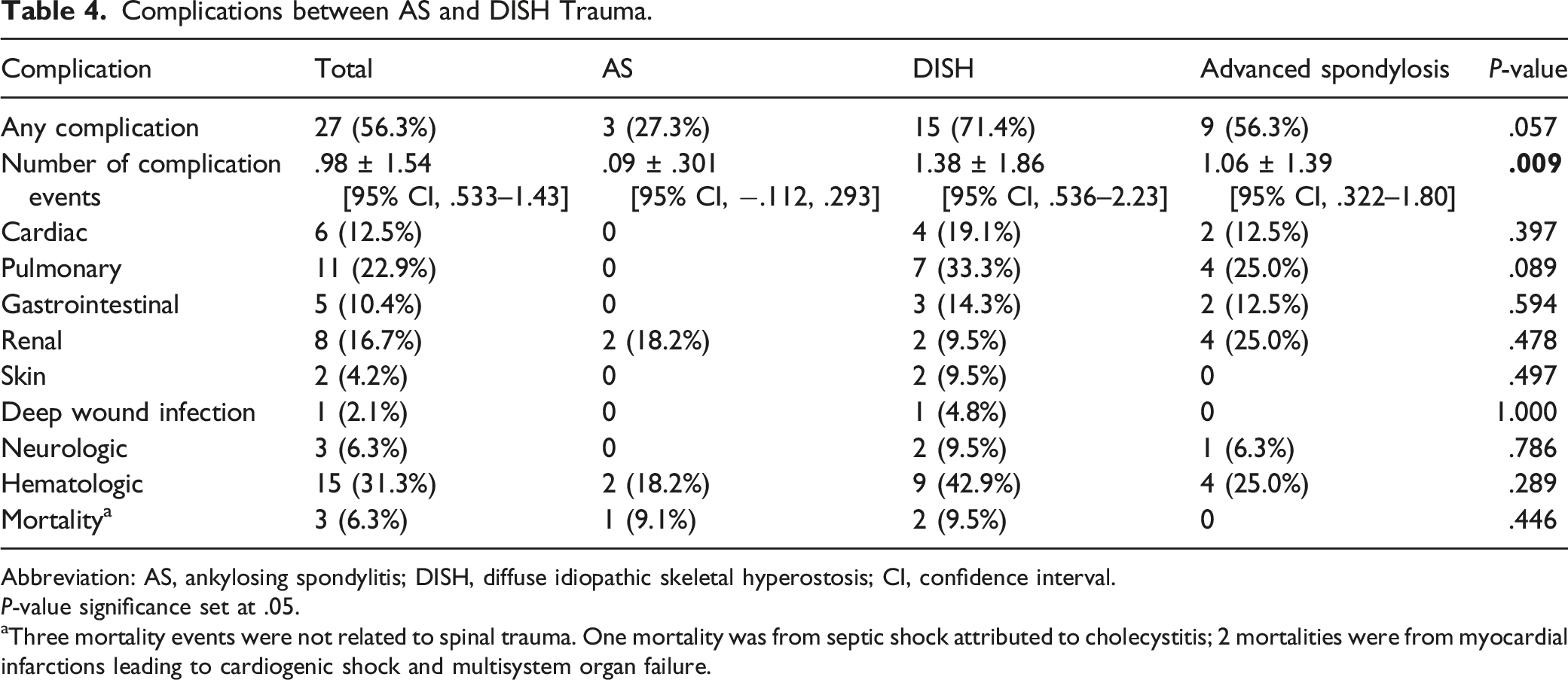
Abbreviation: AS, ankylosing spondylitis; DISH, diffuse idiopathic skeletal hyperostosis; CI, confidence interval.
P-value significance set at .05.
aThree mortality events were not related to spinal trauma. One mortality was from septic shock attributed to cholecystitis; 2 mortalities were from myocardial infarctions leading to cardiogenic shock and multisystem organ failure.
Discussion
Patients with ankylosing spinal conditions are at higher risk for sustaining spine injuries.2,5 Many of these injuries ultimately require surgical stabilization due to the unstable nature of the fracture caused by the relatively long lever arms that develop as the spine becomes ankylosed.18-20 The highly unstable nature of fractures in this population outweigh the risks associated with a predisposition for osteoporosis and stress shielding around spinal instrumentation. This patient population tends to have a higher operative risk given their poor functional status; therefore, the surgical plan must account for and mitigate this risk. 21 MIS techniques with or without navigation provide an alternative to open surgical fixation in this higher risk trauma population. MIS techniques have shown good safety and efficacy with spinal stabilization in this patient population while decreasing operative times and blood loss.10,12,13,22 To the best of our knowledge, this is the first study that has directly compared surgical outcomes after percutaneous treatment of their spinal injuries in AS and DISH patients.
Patients with ankylosing spinal conditions have demonstrated a higher complication and mortality rate following traumatic spine injuries.23,24 Westerveld et al. 3 retrospectively investigated clinical outcomes in AS and DISH patients with spinal fractures regardless of treatment compared to a control group of patients without an ankylosed spine. 3 Their ankylosed cohort included 14 patients with AS and 40 patients with DISH who had an average age of approximately 69 years old. Complications were reported in approximately 85% in the surgically treated ankylosed groups in comparison to ∼50% complications seen in the surgically managed control group. The mortality rate was reported to be 7.1% in AS, 15% in DISH, and 2.7% in the control group. There was a similar CCI score between the 2 ankylosed groups, however the DISH group was found to have a much higher percentage of patients who had diabetes and were obese, 30.8% and 50% respectively, compared to 14.3% and 33.3% in the AS group. 3 Our patient demographics show a similar trend with a greater percentage of patients with obesity and diabetes in our DISH cohort. This may explain the higher complication rate seen in this subset of patients; however, it is difficult to identify the cause of this difference given the relatively low prevalence of ASD and subsequent cohort size.
Sedney et al. reported on the direct comparison of surgical outcomes in patients with ankylosing spinal disorders treated with either traditional open or MIS techniques. They were able to demonstrate a decrease in operative time, estimated blood loss, and need for transfusion in the MIS cohort. However, they found no difference in overall length of hospital stay or mortality rate. 10 Nayak and colleagues similarly reported on a series of 11 patients with ankylosed spines who underwent percutaneous fixation following thoracolumbar trauma. They found MIS stabilization to be an acceptable option allowing for favorable post-operative quality of life as evidence by an average ODI 21 and no patients requiring revision surgery for instrumentation failure or non-union. 12 Our series showed similar results, with no patients requiring revision for non-union or instrumentation failure.
As mentioned above, the surgical risk in this cohort of patients is substantially higher than the general population given their older age and multiple medical comorbidities. In the present study we found a mortality rate of 9.1% in the AS cohort and 9.5% in the DISH cohort. While our findings demonstrate the elevated mortality risk in these patients, however, they are lower than those reported in the systematic review by Westerveld et al. In their review of 400 trauma patients with ankylosed spines, they found a 3-month mortality rate of 17.7% from the cohort of patients with AS and 20.0% from the patients with DISH. 14 Other studies have shown in-hospital mortality rates as high as 30%. 25 This is substantially higher when comparing the reported mortality rate of 2% in individuals treated surgically for traumatic spinal fractures with normal spines. 3 Several studies have suggested advanced age, obesity, and diabetes to be associated with higher mortality rates in trauma patients, all of which are associated with DISH and may explain the higher mortality rates reported.4,23 Our study corroborates this elevated morbidity and mortality risk, although because the variations in diabetes and CCI are not significant, we are unable to conclude that those factors may contribute to these increased risks.
In the AS and DISH population, surgical stabilization is typically extended 2–3 levels above and below the fracture segment due to the inherent instability of the fracture and higher biomechanical stress in ankylosed spines.1,9,18,20 Most prior studies in AS and DISH report instrumentation spanning an average of 5.2 to 7.9 segments.9,10,12-14 In a small cases series of 10 patients undergoing MIS fixation for thoracolumbar trauma with AS or DISH utilized a shorter segment construct, instrumenting an average of 1.8 segments, Krüger et al. reported no instrumentation failures or other operation-associated complications in the short-term post-operative period. 22 In the current study, an average of 3.9 ± 1.6 spinal levels were instrumented across all groups; there was no difference in the number of levels instrumented between the AS, DISH, and advanced spondylosis groups (P = .383). Despite a shorter segment construct, no patients required a revision for instrumentation failure during short-term post-operative follow-up. These results suggest a fusion over a shorter segment than previously described may provide adequate stabilization in AS, DISH, and advanced spondylosis.
Limitations of this study include the small sample size in each cohort and relying on radiographic criteria to determine AS, DISH, and advanced spondylosis groups. While the extensive criteria for spondyloarthropathy and AS were not included in this study, the study used widely accepted radiographic criteria to assign patient to the AS and DISH groups. Another limitation is that ossification posterior longitudinal ligament (OPLL) and ossification of the yellow ligament (OYL) were not reported in this study, which are 2 conditions frequently associated with AS and DISH. Due to the low prevalence of ASD, it was necessary to include patients treated by 1 of 4 surgeons at our institution to maximize the study sample size. However, we acknowledge differences in surgical management, surgical technique, and surgeon experience may confound patient outcomes in this study. Despite the limited number of patients, our series exceeds or is on par with the number of patients included in prior case series published in the literature.7,10,12,14,22 The study was designed to evaluate short-term post-operative outcomes; long-term outcomes were not assessed in this study. Additionally, the retrospective nature of the study lends itself to implicit bias in the selection of patients.
Conclusion
Patients with ankylosing spinal disorders often develop unstable fractures, typically from low energy trauma. MIS remains a viable option in these medically complicated patients, with similar length of surgery, blood loss, and hospital and ICU length of stay between AS and DISH patients. DISH patients a greater number of post-operative complications than AS and advanced spondylosis patients.
Footnotes
Acknowledgments
None.
Declaration of Conflicting Interests
The authors disclose the following outside of the current work: payment for lectures from AOSpine NA and DePuy Synthes Spine; royalties from DePuy Synthes Spine; stock in the American Society for Investigative Pathology; consultant for Biomet; board member for the American Board of Orthopaedic Surgery, the American Orthopaedic Association, the Cervical Spine Research Society, and the Society for Minimally Invasive Spine Surgery; consultant for DePuy Synthes and K2M/Stryker; payment for lectures and travel accommodations from DePuy Synthes and K2M/Stryker; payment for patents and royalties from DePuy Synthes; stock in Innovative Surgical Designs and the American Society for Investigative Pathology; research support from AO Spine North America Spine Fellowship support and AOA Omega Grant; a board member of Maryland Development Corporation; royalties from Thieme, Quality Medical Publishers; and editorial board of Journal of Spinal Disorders and Techniques, The Spine Journal, and Contemporary Spine Surgery. The authors have no further potential conflicts of interest to disclose. DG is a receives payment for lectures from AOSpine NA and DePuy Synthes Spine; receives royalties from DePuy Synthes Spine; has stock in the American Society for Investigative Pathology. EK is a consultant for Biomet. SL is a board member for the American Board of Orthopaedic Surgery, the American Orthopaedic Association, the Cervical Spine Research Society, and the Society for Minimally Invasive Spine Surgery; is a consultant for DePuy Synthes and K2M/Stryker; is a board member for Nuvasive; receives payment for lectures and travel accommodations from DePuy Synthes and K2M/Stryker; receives payment for patents and royalties from DePuy Synthes; has stock in Innovative Surgical Designs and the American Society for Investigative Pathology; receives research support from AO Spine North America Spine Fellowship support and AOA Omega Grant; is a board member of Maryland Development Corporation; receives royalties from Thieme, Quality Medical Publishers; is on the editorial board of Journal of Spinal Disorders and Techniques, The Spine Journal, and Contemporary Spine Surgery. SM, JC, JB, JJ, AT, IY, and DC have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
IRB approval was obtained by the University of Maryland IRB (Protocol: HP-00082698) due to the retrospective nature of the study specific consent requirement was waived by the IRB. This study was conducted in accordance with the 1964 Helsinki Declaration, its amendments, and other equivalent ethical standards.
Disclaimers
The views expressed in the submitted article are our own and not an official position of the institution.