
Abstract
Objective
This study was performed to describe a new minimally invasive surgical technique and to explore its effects and practical use in the clinical setting.
Methods
In total, 22 patients with single-segment thoracolumbar burst fractures underwent treatment with an intelligently inflatable reduction device before common percutaneous pedicle screw fixation. Complications were recorded and short-term effectiveness was evaluated using the visual analogue scale (VAS) score for pain, Oswestry Disability Index (ODI), kyphotic Cobb angle, and anterior edge height of the fractured vertebra preoperatively and postoperatively.
Results
The patients were followed up from 2 to 5 years. The differences in the VAS score and ODI reached statistical significance at different time points. Similar significant differences were observed in the kyphotic Cobb angle and the vertebral body anterior height except between the two postoperative measurements.
Conclusions
The current study indicated that use of the intelligently inflatable reduction device with conventional percutaneous pedicle screw fixation can improve the reduction and healing of single-segment thoracolumbar burst fractures in adult patients. This technique induces minimal trauma, provides reliable fixation, and has few complications.
Keywords
Introduction
Spinal fractures account for 5% to 6% of all fractures, and those in the thoracolumbar region are most common. Thoracolumbar burst fractures are usually caused by high-energy impact. Such fractures can be found in the anterior, middle, and even posterior axis of the spinal column, often leading to progressive instability and kyphosis of the spine. Spinal cord or nerve root injury can sometimes accompany extensive fractures. 1 Pedicle screw fixation has become a conventional treatment approach for thoracolumbar burst fractures because it provides immediate stability of the three axes of the spinal column after the operation and is associated with fewer complications involving the blood vessels and nerves.2,3 However, operative procedures using pedicle screws in traditional open surgery lead to frequent complications, such as higher bleeding volumes and a longer hospitalization time, because of the need for extensive dissection of the surrounding muscles, fascia, and ligaments. Additionally, they often affect the daily life and work of the patient because of persistent back pain, spinal stiffness, and similar complications.4,5 With the development of minimally invasive techniques and fluoroscopic devices, percutaneous pedicle screw fixation procedures are becoming more widely used in spinal surgery. These procedures have the advantages of minimal damage to the posterior spinal column, low bleeding volumes, and a short recovery time after surgery.6–8 Nonetheless, the use of simple posterior percutaneous pedicle screw fixation procedures for thoracolumbar burst fractures reportedly results in poor fracture realignment and loss of repositioned fracture ends after the operation. 9 Therefore, we designed an intelligently inflatable reduction device for such fractures and evaluated the clinical outcomes of its use in patients with single-segment thoracolumbar burst fractures.
Methods
Patients
Institutional review board approval was obtained before collection of data for this retrospective review, and written informed consent was obtained from each participant. The study population comprised consecutive patients with single-segment thoracolumbar burst fractures. None of the patients had neurological abnormalities of the lower extremities or abnormalities of bowel or bladder function. All patients underwent fracture repair using our novel intelligently inflatable reduction device in addition to conventional percutaneous pedicle screw fixation from January 2013 to December 2015 at a single institution. The patients were consecutively treated by the same surgeon using a standard operative technique.
Preoperative evaluation
The eligibility criteria were as follows: (a) no history of surgery for thoracolumbar fracture or spinal deformity in the fracture segment, (b) an isolated-segment burst fracture within the thoracolumbar region (T10 to L2) as determined on anteroposterior and lateral radiographs, (c) pain in the thoracic and lumbar region corresponding to the segment on the radiographs, (d) no neurological abnormality of the lower extremities or abnormality of bowel or bladder function (American Spinal Injury Association category E), (e) no complications of the posterior osteoligamentous complex (such as facet fracture or flexion-distraction ligament disruption) (Frankel grade E), (f) invasion by the dislocated fractured fragments of ≤30% of the spinal canal in cases of posterior wall fracture, (g) age of 32 to 56 years, (h) provision of patient consent, and (i) follow-up duration of ≥2 years.
The exclusion criteria were as follows: (a) prior surgery involving the corresponding spinal segment or a history of spinal column deformity; (b) multiple levels of thoracolumbar fractures; (c) an alteration of structural integrity within the posterior axis of the spinal column or neurological abnormality; (d) invasion by the dislocated fractured fragments of >30% of the spinal canal in case of posterior wall fracture requiring decompression; (e) a diagnosis of osteoporosis, a vertebral body tumor, tuberculosis, or other pathological fractures; (f) hepatic or renal malfunction, hemostatic disorders, or systemic infections; and (g) unsuitability for surgery or unwillingness to attend follow-up visits.
Description of the reduction device
An intelligent inflatable reduction device was proprietarily designed and developed by our team. 10 This device consists of an inflatable airbag, automatic air pump, inlet hose, exhaust valve, and associated control panel. The maximum height of the airbag was set to 25 cm after inflation. The appearance of the device is three superimposed semicircles resembling a clover. The device comprises two layers: the inner layer is made of polyvinyl chloride sheets for better air containment, and the outer layer is reinforced Oxford cloth. The automatic air pump includes electromagnetic air compressors (385 W, 220 V/50 Hz) with output air pressure of 0.05 MPa and an airflow rate of 300 L/min (Figure 1(a)).

(a) Intelligently inflatable reduction device and components. a: Supporting arms. b: Radiolucent spine operating table. c: Main power switch. d: Power cord. e: Pressure gauges. f: Speed control knobs. g: On/off switches. h: Air pump. i: Exhaust valve. j: Air cushion sac. k: Inlet hose. (b) The state of complete expansion of the airbag. In the schematic diagram, the patient was positioned supine on a radiolucent spine operating table. (c, d) At the center of the fractured vertebra, the airbag of the inflatable reduction device was placed on the back of the patient.
Inflatable reduction
Under general anesthesia with endotracheal intubation, the patient was positioned supine on a radiolucent spine operating table. At the center of the fractured vertebra, the airbag of the inflatable reduction device was positioned to the back of the patient. After the power was turned on, the airbag was inflated slowly (2 mm/s) by the air pump when the inlet valves were open. Meanwhile, the patient’s shoulders and buttocks were arranged to achieve effective hyperextension in the subsequent steps. When the airbag was initially inflated at a height of 10 cm, the pump was stopped for 5 minutes to allow adjustment of posture. Inflation was continued to 15 to 20 cm and held for 5 minutes to allow adjustment of posture, and the airbag was then deflated slowly (2 mm/s). Three cycles of inflation and deflation were performed under G-arm fluoroscopy, and the maximum height of the airbag was limited to <25 cm (Figure 1(b)–(d)). After reaching the ideal reduction, the patient was gently placed in the prone position under maintenance of traction to allow for percutaneous implantation of pedicle screws and rods (Figure 2).

(a) On lateral X-ray fluoroscopy of the lumbar spine, the kyphotic angle was 16.8 degrees and the average preoperative percentage of the relative height of the anterior margin of the fractured vertebra was 56.6% before the inflatable reduction. (b) The patient was stretched under anesthesia. (c) The kyphotic angle was −4.6 degrees and the average preoperative percentage of the relative height of the anterior margin of the fractured vertebra was 88.7% after the inflatable reduction on the lateral view. (d) The percutaneous pedicle screws were implanted under X-ray fluoroscopy.
Surgical techniques
The first step of the surgical procedure was to locate the entry points of the pedicles on anteroposterior and lateral views of the thoracolumbar spine using the G-arm fluoroscope. The two vertebral bodies adjacent to the fractured vertebra were percutaneously fixed by the pedicle screws. A 20-mm skin incision that covered the entry points of the pedicle screws was made and extended into the underlying fascia. A series of four sequential tissue retractors were then used to pull open the muscles and fascia. The guide wire of each percutaneous pedicle screw was inserted into the pedicle according to the “Scotty Dog” imaging monitoring technique. 11 Briefly, the wire was inserted into the central axis of the pedicle, parallel to the endplate of the corresponding vertebral body on the lateral view. It was slowly advanced into the vertebral body through the pedicle using a power drill with visualization through the G-arm fluoroscope. A self-tapping cannulated screw with matching diameter and length was inserted into the vertebra over the wire within the protection sleeve, and the wire and protection sleeve were subsequently removed. According to the preoperative computed tomography (CT) scan, the pedicle screw was percutaneously implanted into the fractured vertebral body through the intact pedicle. In total, four to six pedicle screws were percutaneously inserted into the adjacent vertebrae or the fractured vertebra using the same approach (Figure 2(d)). These operative procedures were carried out using the G-arm fluoroscope. The U-shaped openings of the head of the two ipsilateral pedicle screws were aligned to facilitate placement of the rod. Two titanium rods with matching length were inserted respectively through the U-shaped openings of the two ipsilateral pedicle screws from the coronal incision and linked to the rod in the prepared channel of the paraspinous muscles to secure the pedicle screws. The caudal, middle, and cranial pedicle screws were then tightly fixed in sequence. Once the placement was satisfactory as shown by fluoroscopy, the U-shaped tails were removed and the incisions were irrigated and closed in layers.
Postoperative management and follow-up
A prophylactic antibiotic was given intravenously for 3 days after surgery. Ambulatory activities while wearing a brace were allowed on postoperative day 7, and the brace was kept in place for 3 months.
In all patients, clinical and functional outcomes were evaluated by the visual analogue scale (VAS), Oswestry Disability Index (ODI), Cobb angle, and anterior edge height of the fractured vertebra preoperatively, 7 days postoperatively, and at the last follow-up. The relative height of the anterior margin of the fractured vertebra (H) was defined as follows: H = Hc / Hr × 100%, where Hc and Hr are the actual and expected height of the anterior margin of the fractured vertebra, respectively. The Hr was the mean value of the height of the anterior margin of the two vertebral bodies adjacent to the fractured vertebra. 12 The height of the anterior margin and the Cobb angle of kyphosis were measured on the supine lateral plain film.
Statistical analysis
The data, expressed as mean ± standard deviation, were analyzed using SPSS version 18.0 software (SPSS Inc., Chicago, IL, USA). Statistically significant values were defined as those with a p value of <0.05 with a two-tailed distribution. Repeated-measures analysis of variance was used to examine the improvements in the disease severity scores (VAS score, ODI, and anterior edge height of the fractured vertebra) before versus after surgery, and a paired-sample t test was used to examine the variation in the Cobb angle before versus after surgery.
Results
Twenty-two patients were included in this study (12 men, 10 women; age range, 32–56 years). Two patients had T10 fractures, three patients had T11 fractures, five patients had T12 fractures, seven patients had L1 fractures, and five patients had L2 fractures (Table 1). All patients were successfully treated with percutaneous minimally invasive procedures after inflating reduction. No patients’ fractures involved invasion of the spinal canal or foramen. The average operative time was 65 minutes (range, 45–90 minutes) in addition to the 45 minutes required for inflating reduction. The average intraoperative blood loss volume was 60 mL (range, 30–120 mL). The average hospital stay was 7 days (range, 5–14 days). The average follow-up duration was 36 months (range, 24–60 months). No patients required a blood transfusion or hospitalization in the intensive care unit. The postoperative complications included pedicle screw misplacement, but with no neurologic sequelae (n = 1); a superficial infection of the incision that was remedied with intravenous antibiotics (n = 1); and a loose screw (n = 1). No implant breakage occurred. Bone union was achieved in all cases. Twenty patients underwent a second operation to remove the implants from 1.5 to 2.5 years postoperatively, and two patients declined surgical removal of the implants.
Patients’ demographic data.

Demographic data
The mean preoperative VAS pain score was 7.82 (range, 6–9). This score improved to 3.09 (range, 2–5) at 1 week postoperatively and to 1.05 (range, 0 to 3) at the last follow-up assessment. The mean clinical improvement in the ODI was also significant for the entire cohort (84.2 preoperatively, 46.3 at 1 week postoperatively, and 12.2 at the last follow-up) (Table 2).
Clinical assessment.

Data are presented as mean ± standard deviation.
VAS, visual analogue scale; ODI, Oswestry Disability Index.
Significant difference between 1 week postoperatively and preoperatively (p < 0.05).
Significant difference between last follow-up and preoperatively (p < 0.05).
Significant difference between last follow-up and 1 week postoperatively (p < 0.05).
Radiographic outcomes
The average preoperative Cobb angle was 16.3 degrees (range, 8–24 degrees). This angle had decreased to 3.7 degrees (range, 1–8 degrees) at 1 week postoperatively, representing an average deformity correction of 12.6 degrees. At the last follow-up, the Cobb angle was 5.5 degrees (range, 2–12 degrees), and the average loss of kyphotic correction was approximately 2 degrees (Figure 3). The average preoperative percentage of the relative height of the anterior margin of the fractured vertebra was 59.5% (range, 49% to 77%), and the percentage had improved to 86.9% (range, 72% to 98%) at 1 week postoperatively. At the last follow-up, the percentage of the relative height of the anterior margin of the fractured vertebra was 83.5% (range, 72% to 92%) (Table 3).
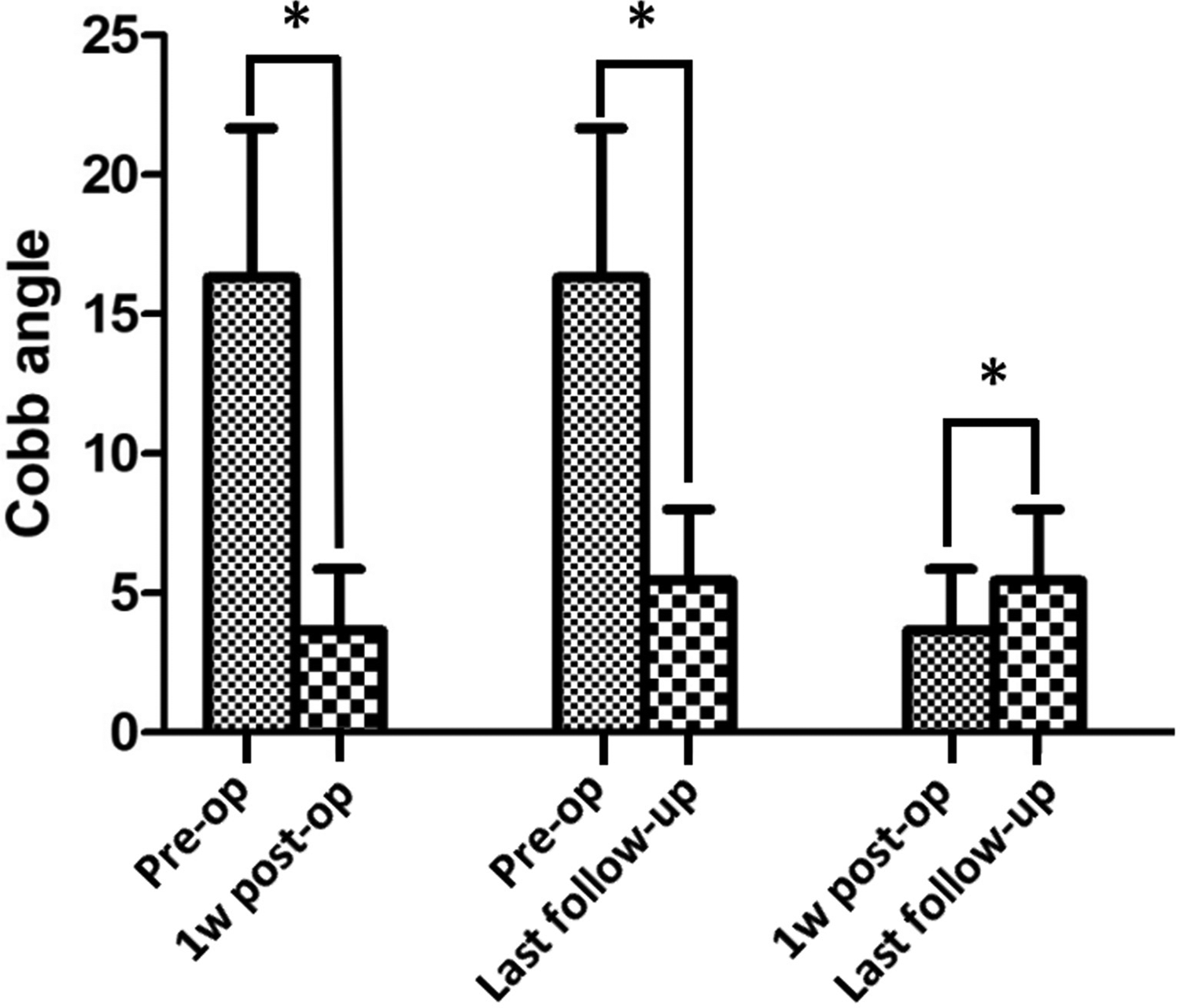
The differences in the kyphotic Cobb angle reached statistical significance at different time points. The asterisk (*) indicates a significant difference (p < 0.05).
Roentgenographic changes.

Note: H indicates the relative height of the anterior margin of the fractured vertebra.
Significant difference between 1 week postoperatively and preoperatively (p < 0.05).
Significant difference between last follow-up and preoperatively (p < 0.05).
Clinical efficacy and outcome: representative case
A 50-year-old woman with burst fractures of the first lumbar vertebra underwent the above-described combinational procedure. She underwent a second operation to remove the implants and had satisfactory spine function at 2 years postoperatively (Figure 4).

(a, b) The burst fractures of the lumbar vertebrae were diagnosed by anteroposterior and lateral X-ray fluoroscopy of the lumbar spine preoperatively. (c, d) A satisfactory outcome was achieved for the reduction of the vertebral fracture and the position of the pedicle screws. (e, f) The vertebral fracture exhibited bony union when the pedicle screws were removed at 2 years postoperatively.
Discussion
Whether surgical treatment should be used for thoracolumbar burst fractures without neurological abnormalities of the lower extremities or abnormalities of bowel and bladder function remains controversial. A systematic review and meta-analysis revealed no differences in disability or pain outcomes between operative and nonoperative treatments of A3 and A4 thoracolumbar fractures in neurologically intact patients. 13 However, a previous study showed that in about 25% of neurologically intact patients with thoracolumbar burst fractures and a thoracolumbar injury classification and severity score of 2, nonsurgical management failed because of pain that limited mobilization. 14 Greater kyphosis, stenosis, and fragmentation of the fracture was associated with a higher likelihood of requiring surgery. 14 A literature review demonstrated that operative treatment may decrease the risk of neurologic impairment. 15 Prophylactic stabilization and fusion of acute burst fractures without neurologic deficits has significant advantages over conservative management. Therefore, appropriate clinical management of thoracolumbar burst fractures without neurological deficits is important to prevent the development of spinal deformities, chronic pain, and latent nerve injury.
Advantages of intelligently inflatable reduction in conjunction with percutaneous pedicle screw fixation for treating thoracolumbar burst fractures
The hypothesis of this study was that reduction of a fractured vertebra can be achieved using our intelligently inflatable reduction device before percutaneous placement of pedicle screws and rods. The desired height of reduction was achieved under G-arm fluoroscopy with multiple in-procedure adjustments, and satisfactory reduction occurred in most cases. Additionally, satisfactory clinical efficacy and outcomes of percutaneous pedicle screw fixation were obtained. Reduction of a fractured vertebra historically relied on manual positioning of the patient under general anesthesia with endotracheal intubation, and this technique also achieved a somewhat good effect in the clinical setting. However, manual postural reduction is associated with potential complications such as excessive reduction and injury of the posterior osteoligamentous complex, spinal cord, and nerve root. The intelligently inflatable reduction device described in the present report has many advantages, such as safety, reliability, portability, and convenient operation in the surgical suite. Previous studies have shown satisfactory clinical efficacy of this device for the treatment of non-osteoporotic thoracolumbar vertebral compression fractures when used in combination with multifunctional external fixation braces. 16 Additionally, it was used as a substitute for a balloon in percutaneous balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures and achieved satisfactory reduction and the expected clinical efficacy. 10
In the current study, the technique of intelligently inflatable reduction in situ and in combination with placement of percutaneous pedicle screws and rods represents a unique fixation system for treating thoracolumbar burst fractures. The results were satisfactory during an average 36-month follow-up. Intraoperative variables, including the operation time (average, 65 minutes in addition to the 45 minutes required for inflatable reduction) and blood loss (average, 60 mL), were more favorable than those in another report describing open (posterior spine) surgery with short-segmental pedicle screw fixation (average operation time and blood loss of 140.3 minutes and 311.5 mL, respectively). 17 This difference is mainly attributable to the performance of extensive paraspinal muscle stripping in open procedures. In contrast, percutaneous pedicle screw fixation in this current study dramatically decreased the severity of iatrogenic damage to the paraspinal musculature and actually had positive effects on postoperative trunk muscle performance.
The clinical outcomes in the present study were based on the VAS score for pain and the ODI for disability. Significant improvements in overall pain and disability were observed at 1 week postoperatively and at the last follow-up (p < 0.001). This result is similar to the cited literature. 18 Percutaneous polyaxial screws can preserve the minimally invasive aspect of the procedure in favor of osteosynthesis and can improve the mean local kyphosis. The average correction in the Cobb angle and the restoration of the vertebral body height were comparable with those reported in open operations. However, less Cobb angle loss occurred than in a long-term follow-up study 12 ; in the present study, the average deformity correction of the Cobb angle was 12.6 degrees at 1 week postoperatively, albeit with loss of 2 degrees at the last follow-up. Additionally, the average preoperative percentage of the relative height of the anterior margin of the fractured vertebra had improved 27.4% at 1 week postoperatively, although a loss of 3.4% had occurred at the last follow-up.
Biomechanical evidence
Compared with a four-screw construct, biomechanical stability can be significantly increased through the implantation of six pedicle screws in the fractured vertebral body and the vertebral bodies adjacent to the fractured vertebral body. A six-screw short-segment construct has been recommended as an option in the surgical treatment of unstable axial load injuries of the thoracolumbar spine as long as the additional screws could be safely placed. 19 In the present clinical study, the percutaneous pedicle screw was implanted into the pedicle of the fractured vertebral body if it was determined to be intact according to the preoperative CT scan. In total, 123 pedicle paths with pedicle screw insertion were analyzed in this cohort of 22 patients. There were two cases of bilateral rupture of vertebral arch pedicles and five cases of unilateral rupture of vertebral arches where they were not implanted with pedicle screws. All other cases involved bilateral pedicle screw implantation. Within the study period, the differences in the Cobb angle and anterior edge height of the fractured vertebra were not significantly different between 1 week postoperatively and the last follow-up.
In terms of safety, the procedures performed in the current study showed a high accuracy of pedicle screw placement. We assessed the accuracy of the pedicle screw insertion footprints on the postoperative CT scans. The outcome indicated a misplacement incidence of 8.1% (10 of 123 screws), while a previous report showed that the proportion of misplaced screws was higher in the freehand fluoroscopy group than in the robot-assisted group (11.1% vs. 6.6%, respectively). 20 All misplaced screws were clinically asymptomatic until removal at 2 years postoperatively. Although three-dimensional robotic-assisted fluoroscopy improved the accuracy of percutaneous pedicle screw insertion, 21 we believe that G-arm fluoroscopy is a reliable tool for in situ inflatable reduction and placement of percutaneous thoracolumbar pedicle screws, despite the longer learning curve required to improve the accuracy of percutaneous pedicle screw insertion techniques and the challenges encountered in maintaining the desired median operation time.
Conclusion
As a new minimally invasive surgical technique, intelligently inflatable reduction in conjunction with percutaneous pedicle screw fixation can be an alternative procedure for treating thoracolumbar burst fractures without inducing neurological abnormalities of the lower extremities or abnormalities of bowel or bladder function. This technique does not increase the rate of postoperative nerve deficits and does not have a high rate of other complications. A prospective randomized controlled trial may provide more evidence of the advantages of this technique. The results of our study indicate that this is a reliable and safe procedure. In addition, intelligently inflatable reduction combined with percutaneous pedicle screw fixation provides a viable and useful alternative to the other open surgical techniques.