
Abstract
Background:
Transforaminal lumbar interbody fusion (TLIF) is presently the most used method to achieve lumbar interbody fusion worldwide. The special preparation and cage insertion imply a risk of an undesirable side effect in the form of residual neurogenic pain. This issue has not been investigated prior in a randomized clinical trial (RCT) set up.
Aim:
To test whether TLIFs had a higher incidence of leg pain in comparison to a common instrumented posterolateral fusion (PLF) and to test whether a higher occurrence of leg pain on the ipsilateral side in the TLIF group was present.
Methods:
One hundred patients included in a RCT comparing TLIF and PLF fulfilled pain drawings and numeric rating scale (NRS) scale from 0 to 10 preoperatively, after 1 year, and after 2 years. Difference in pain appearance, type, localization, and intensity was compared between groups.
Results:
A slightly higher number of patients in the TLIF group reported leg pain at 2 years follow-up: no leg pain, 47% (PLF) and 37% (TLIF); unilateral leg pain, 31% (PLF) and 25% (TLIF); bilateral leg pain, 22% (PLF) and 37% (TLIF), p = 0.270. Numbness and pins and needles on the anterior aspect of the lower leg were marked by 10% and 12% of TLIF patients compared to 6% and 4% in PLF patients p = 0.498/0.197. The ipsilateral side of cage insertion in the TLIF group was not a place for new leg pain compared to the contralateral side.
Conclusion:
The special surgical preparation used in TLIFs does not result in the development of new ipsilateral leg pain. However, a higher percentage of the patients in the TLIF group had new leg pain in comparison to PLF after 2 years.
Keywords
Introduction
Transforaminal interbody lumbar fusion (TLIF) has become the method of choice to achieve anterior support in lumbar fusions. 1 –3 The approach changed over time from anterior lumbar interbody fusion (ALIFs) in the 90s (4, 5) to TLIFs in the 00s. However, the benefits of anterior support in lumbar fusions have been difficult to validate. 2,3,5 –9 Today, the TLIF procedure is often done with minimal invasive spinal surgery (MISS) technique. 10
The procedure carries a risk of damage to the nerve root or the dorsal root ganglion compared to a standard instrumented lumbar fusion (posterolateral fusion (PLF); Figure 1). On the other hand, the use of interbody fusion might indirectly decompress the neuro foramina and by that relieving existing radicular pain (Figure 2). Recently, TLIF in MISS technique has been claimed to cause much higher rates of nerve root injuries. 11 One might speculate that the reason for lack of superiority in TLIF surgery 2,3 could be due to preparation and cage insertion, affecting the nerve. Alternatively, by scar tissue formation compromising the upper nerve root, resulting in residual radiculopathy or permanent radiculitis.

Intraoperative preparation of surgical field in a patient randomized to TLIF. TLIF: transforaminal lumbar interbody fusion.

TLIF used in a degenerative spondylolisthesis, with restoration of the sliding, disc space, and neuroforamen to anatomical normal position. Patient randomization number 14 pre- and postoperative. TLIF: transforaminal lumbar interbody fusion.
Pain drawings could be used as a tool to access leg pain after lumbar spine surgery, since one would expect an increase in radiating pain in the leg, if the root should be irritated by the procedure by handling or by scar tissue formation (Figure 1). The aim of the present study was therefore to determine the presence and type of pain 12 as well as the distribution and intensity of pain after TLIF surgery compared to standard posterolateral instrumented fusions (PLF) using pain drawings and pain scores in a randomized clinical trial (RCT) setting with 2-year follow-up.
Materials and methods
The original study was carried out between 2003 and 2008. The primary article presents details of the methods used in this study. 2 One hundred patients (mean age 49.8 years) were randomized (Table 1). Baseline demographics of the two randomized groups were equal at baseline except for ongoing compensatory/ligation case and whether laminectomy or laminotomy was done. The latter was due to the different operation techniques, where TLIF always implied partial laminectomy/facetectomy (Table 1). Baseline characteristics concerning pain type and distribution of the patients completing pain drawings are presented in Table 2.
Demographics and patient characteristics according to treatment at baseline.a

TLIF: transforaminal lumbar interbody fusion.
a Values are mean (range) or number (percentage).
Presence and type of pain in the four pooled areas.a
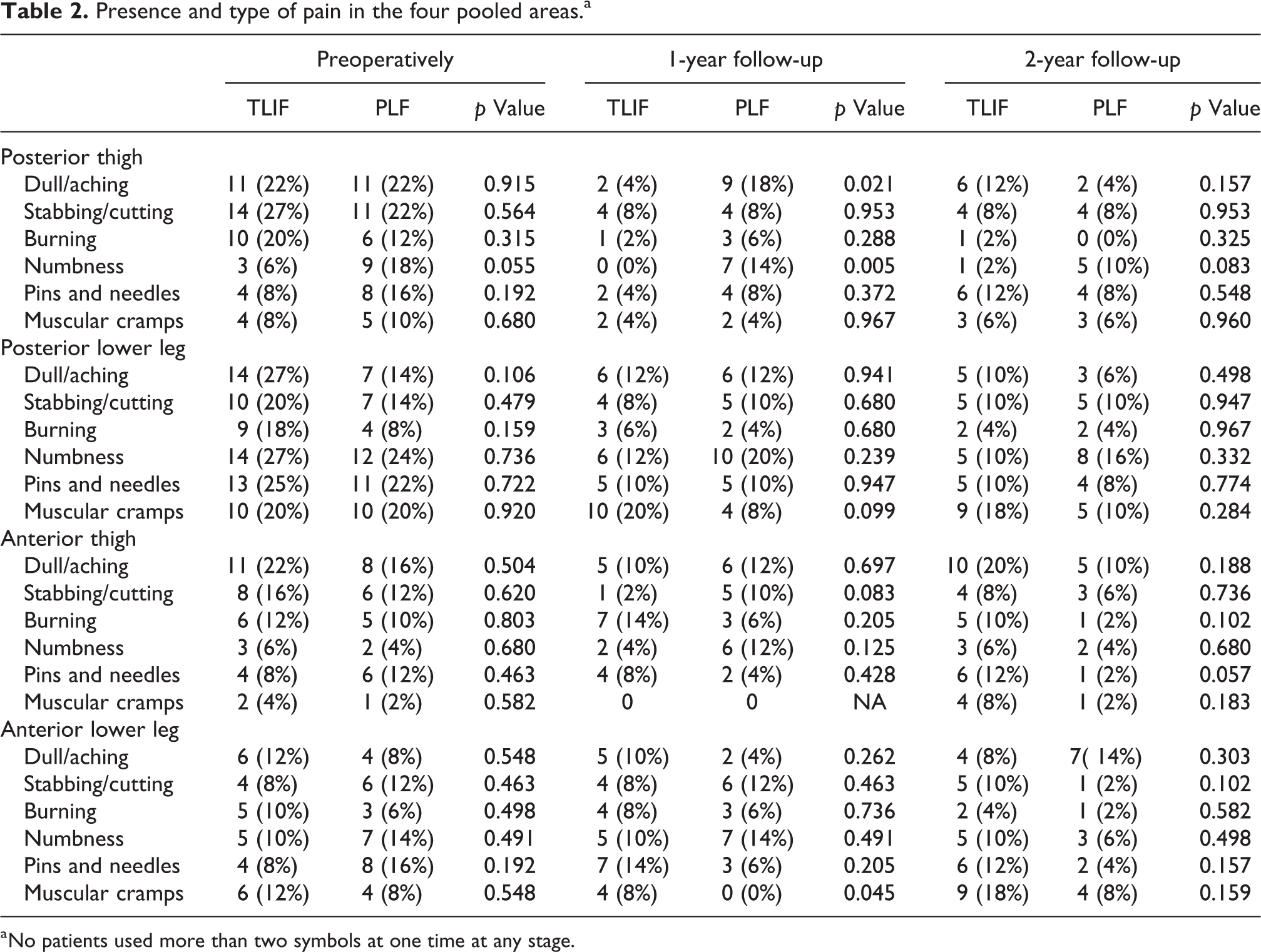
a No patients used more than two symbols at one time at any stage.
Forty-nine patients were allocated to PLF with titanium TSRH (Medtronic, Minneapolis, Minnesota, USA) pedicle instrumentation and fifty-one patients to TLIF in the form of a tantalum cage (Implex/Zimmer, Warsaw, Indiana, USA) placed using an approach lateral to the facet joint, supported by a PLF using pedicle screws (titanium TSRH, Medtronic).
Outcome parameters
The pain drawings consisted of a front and back outline of a person as well as the area under the feet. The patients were asked to draw all their different pain using six different symbols for marking pain: (1) dull/aching, (2) burning, (3) numbness, (4) pins and needles, (5) stabbing/cutting, and (6) muscular cramps (Figure 3). Special attention was also paid to the side of insertion of the cage in the TLIF group and compared to the presence and type of newly developed pain after surgery. The data were pooled into four areas: posterior thigh, posterior lower leg, anterior thigh, and anterior lower leg, and the presence of the six abovementioned types of pain in each area was registered. The second author blinded to treatment groups scored initially all pain drawings, and data were pooled and compared between preoperative and after 1 and 2 years, as shown in Table 2.
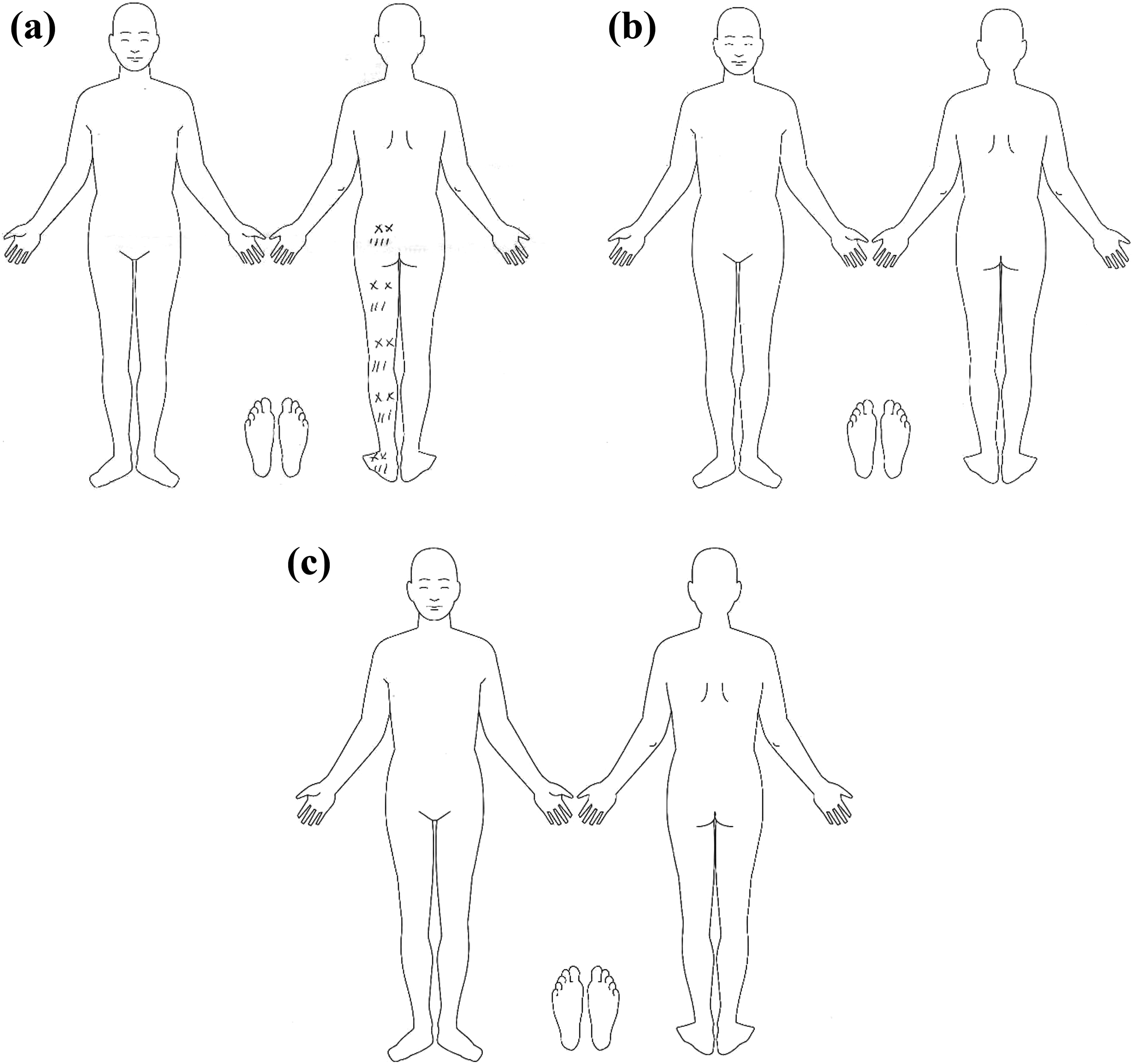
Representative pain drawings, example from patient randomization number: 87 (a) Preoperative pain drawing, S1 dermatome; (b) pain drawings after 1 year, pain removed; and (c) pain drawings after 2 years, pain still removed. Symbols used: dull/aching NNN, burning XXX, numbness = =, pins and needles:::, stabbing/cutting ///, and muscular cramps SSS.
The leg-pain intensity was registered using a NRS scale 0 (no pain) to 10 (worst) with the leg-pain intensity experienced at the time of examination, with their average perceived leg-pain intensity in the last 2 weeks, and the worst leg-pain experienced in the last 2 weeks. 13
Statistics
All analyses comparing the two intervention groups were done using the intention to treat principle. Comparison between groups was done using nonparametric tests (Mann–Whitney rank-sum test for unpaired data, Wilcoxon signed rank test for paired data, χ 2 statistics, or the Kruskal–Wallis test for equality at groups, with correction for ties) depending on the nature of the data. Significance level was 5% using two-tailed testing. Intercooled Stata version 13 for Windows was the software used for statistical analysis.
Ethics
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (the local Danish regional research and ethical committee approved this study. Study protocol (20030172)) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Results
Except for one variable regarding pain, the two groups were similar at baseline (Table 2). The one exception was numbness in the posterior thigh, which was reported by 6% in the TLIF group and 18% in the PLF group (p-value 0.055). This difference remained present at both 1-year and 2-year follow-up.
The total reduction in intensity pain score from preoperative to postoperative was significant in both groups using average-leg pain NRS score as it is within the last 14 days changed from 5.1 to 3.5 p = 0.008 (TLIF) and from 5.0 to 2.9 p = 0.0003 (PLF; Table 3; Figures 4 and 5).
Intensity in leg pain NRS 0–10 pain was reduced in both groups. Data preoperatively, 1 year and 2 years.a
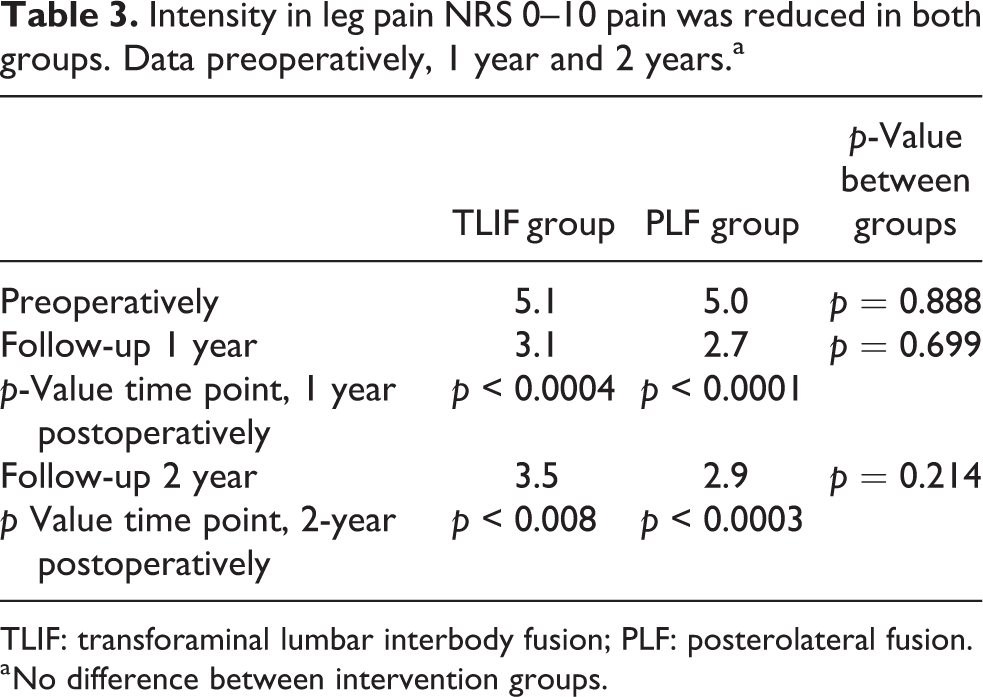
TLIF: transforaminal lumbar interbody fusion; PLF: posterolateral fusion.
a No difference between intervention groups.

Presence and distribution of leg pain in the whole leg.

Presence and distribution of leg pain below the knee.
At 1-year follow-up, five patients (10%) in the TLIF group had developed new leg pain, two patients on the ipsilateral side to cage insertion, and three patients on the contralateral side. In comparison, seven patients (14%) in the control group developed new leg pain (p = 0.491). TLIF patients developing pain on the side contralateral to cage insertion used the following symbols: burning (one patient), numbness (two patients), pins and needles (one patient), and cramps (one patient). The two patients developing ipsilateral pain used stabbing, dull, pins and needles. Burning symbol was not used by these two patients. The seven patients in the control group used the following symbols: numbness (five patients), dull (two patients), stabbing (two patients), and pins and needles (one patient). Four of the five patients in the TLIF group, who developed leg pain at 1-year follow-up, did not mark this at their 2-year follow-up. However, another five patients marked new presence of leg pain at their 2-year follow-up in a leg marked pain free preoperatively. Two patients marked pain ipsilateral to the side of cage insertion, two patients marked pain on the contralateral side, and one patient marked the appearance of bilateral leg pain. In the PLF group, only one patient marked pain in a leg marked pain free preoperatively at 2-year follow-up. Numbness and pins and needles on the anterior aspect of the lower leg were marked by 10% and 12% of TLIF patients compared to 6% and 4% in PLF patients (p = 0.498/0.157). Looking at the posterior aspect of the lower leg, numbness and pins and needles were marked by 10% and 10% of TLIF patients compared to 16% and 8% in PLF patients (p = 0.332/0.774). Looking at the anterior thigh, numbness and pins and needles were 6% and 12% in the TLIF group compared to 4% and 2% in the PLF group, respectively (p = 0.680/0.057; Table 2; Figures 4 and 5). The development of new pain in the TLIF cohort alone was examined in relation to the side of cage insertion (Table 4). This was further investigated according to gender (p = 0.626), age, ongoing case (p = 0.510), and diagnosis (p = 0.843). No significant correlation appeared.
Distribution of leg pain according to side of TLIF cage insertion.a
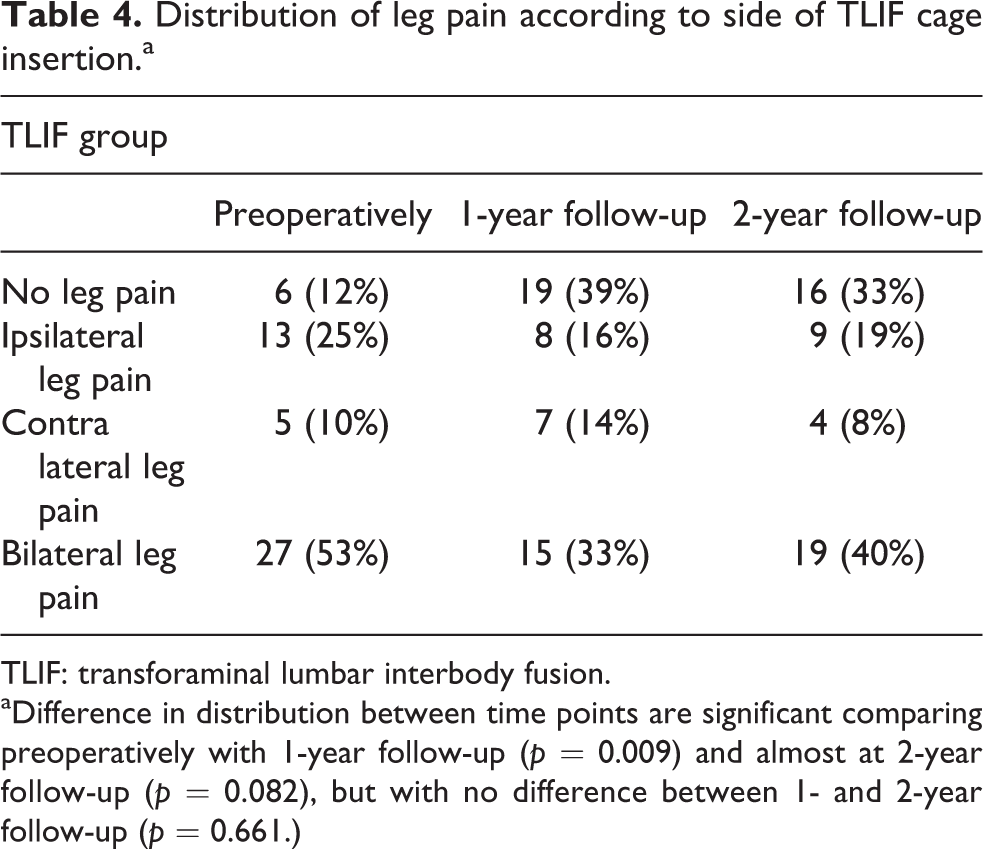
TLIF: transforaminal lumbar interbody fusion.
aDifference in distribution between time points are significant comparing preoperatively with 1-year follow-up (p = 0.009) and almost at 2-year follow-up (p = 0.082), but with no difference between 1- and 2-year follow-up (p = 0.661.)
Discussion
In this article, we investigated pain 1 and 2 years after primary index surgery in a RCT between PLF and TLIF procedure to see whether there was a difference in the: (1) presence of pain, (2) type of pain, (3) distribution of pain, (4) appearance of new pain, and (5) the intensity of pain. To our knowledge, this is the first study to address the question whether the special approach and the cage insertion could be a cause of development of persistent radiculitis or radiculopathy in a randomized setting. Further strength of the study is a one-center design, which gives the possibility of standardizing the patient selection, the surgical techniques, and the rehabilitation. With a follow-up rate of 96% after 2 years, the study can be classified as valid. Relevant issues regarding external validity are the degree of patient heterogeneity, specialization and surgical strategies, and the individual surgeon’s skills. Senior surgeons performed all operations.
The patient alone did all pain drawings beforehand and without any assistance of the doctor. The pain drawings were scored blind to the type of intervention. Pain drawings have, for many years, been used as a tool to access low back pain 14,15 and the repeatability concerning pain is acceptable, however, the sensational drawings can be challenged. The pain drawings done in this study were a simplified version of the method used by Margolis et al. 12 close to the simplified version used by Ohnmeiss. 16 This scoring method has been shown to have very high reliability/repeatability, 12,15,17 and since it offers no clinical judgment, the scoring can be done without an expert. Using this simple method, we found no difference between the two treatment groups.
Pain drawings have earlier been associated with positive radiological nerve root entrapment syndromes, 18 –21 however, Bertilson et al. found a weak agreement between MR visible nerve root entrapment and pain drawings with a specificity of 61–77%. 22 Prins et al. found that higher lower extremity region scores in pain drawings were associated with significant poorer outcome in Owestry Disability Index (ODI) and Short Form Health Survey (SF). 23 Hence, we found that they were able in a reliable way to assess the presence of radicular symptoms.
Our goal in the present study was to test whether TLIF surgery could be associated with a higher amount of radiculopathy or radiculitis, reflected in change in pain drawings and pain intensity 1 and 2 years after surgery between the randomized groups, thus suggesting unwanted side effects of the method. We found no such correlation and our results are in accordance with the results from Desai et al. 24,25
TLIF is the method of achieving circumferential fusion with the lowest frequency of roots injuries/radiculitis 2% posterior lumbar interbody fusion 7.8% and ALIFs 15.8%, 4,11 but since the incidence of nerve root injury is higher than a normal PLF, 26 the procedure should only be performed in case a PLF is not suffice. Our results in the present study support this view.
The reason of the slight rise of more pain in the TLIF group can be a reminder that lumbar fusion is not necessarily a pain removing operation, but rather a pain reducing operation and the procedure might affect the total balance of the spine. 27 One might speculate about the reasons. The TLIF construct is a circumferential fusion and due to that more rigid with a higher stiffness. Theoretically, this would result in earlier development of adjacent segment degeneration (ASD), compared to the normal PLF, 28 and actually, this could be the primary sign of ASD in our material, which calls for further research in a long-term perspective.
The place and role of minimally invasive TLIF is still debatable due to the latest reports with higher and severe amounts of nerve root injuries and concomitant radiculitis. 11,26 So, the conclusions which can be drawn from our study are that a slightly higher percentage of the patients in the TLIF group developed bilateral leg pain 2 years after, however, not significant. With regard to our open TLIF procedures, cage insertion could not be related to a significant increase in radiculopathy or radiculitis at ipsilateral side of cage insertion and the patients had significant reduction in pain intensity score compared to preoperative. New literature concerning TLIFs used in MISS technique has shown different results with higher nerve root injuries and radiculitis, which indicate that if TLIFS should be performed, it should be performed as open procedure based on existing literature. 11,26
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.