
Abstract
Purpose:
To validate the effectiveness of percutaneous pedicle screw (PPS) fixation for spinal fractures associated with diffuse idiopathic skeletal hyperostosis (DISH) by comparing surgical outcomes for PPS fixation and conventional open posterior fixation. Patients with DISH are vulnerable to unstable spinal fractures caused by trivial trauma, and these fractures have high rates of delayed paralysis, postoperative complications, and mortality.
Methods:
This retrospective study assessed surgical outcomes for 16 patients with DISH (12 men; mean age 76.1 ± 9.4 years) who underwent PPS fixation for spinal fractures (pedicle screw (PS) group), and for a control group of 25 patients with DISH (18 men; mean age 77.9 ± 9.9 years) who underwent conventional open fixation (O group) at our affiliated hospitals from 2007 to 2017. We evaluated the preoperative physical condition (American Society of Anesthesiologists (ASA) classification), neurological status (Frankel grade), and improvement after surgery, fusion length, operating time, estimated blood loss, and perioperative complications.
Results:
Preoperatively, the PS group consisted of one ASA-1 patient, eight ASA-2 patients, six ASA-3 patients, and one ASA-4 patient; by Frankel grade, there were 2 grade B patients, 13 grade C, 4 grade D, and 6 grade E patients. The O group had 2 ASA-1 patients, 13 ASA-2, 9 ASA-3, and 1 ASA-4 patients. Frankel grades in the O group reflected severe neurological deficits, with 3 grade C patients, 2 grade D, and 11 grade E (p = 0.032) patients. The two groups had similar rates of neurological improvement (33.3% of PS and 40.0% of O patients; p = 0.410) and mean fusion length (PS 5.1 ± 0.8 segments; O 4.9 ± 1.2). The mean operating time and estimated blood loss were 168.1 ± 46.7 min and 133.9 ± 116.5 g, respectively, in the PS group, and 224.6 ± 49.8 min and 499.9 ± 368.5 g in the O group. Three O-group patients died of hypovolemic shock, respiratory failure, and pneumonia, respectively, within a year of surgery.
Conclusion:
Conventional open posterior fixation and PPS fixation for DISH-related spinal fractures were similar in fusion length and neurological improvement. However, PPS fixation was less invasive and had lower complication rates.
Keywords
Diffuse idiopathic skeletal hyperostosis (DISH), a noninflammatory systemic condition characterized by ossification of the spinal ligaments and entheses, was first described by Resnick et al. 1 DISH occurs most frequently in elderly men. 2,3 DISH typically appears on radiographs as ossification along the anterolateral aspect of the vertebral bodies, especially in the thoracic spine. 1,4 Although DISH can be asymptomatic, patients typically complain of low back pain and of limited range of motion in the trunk (caused by spinal ossification). 5
In DISH patients, trivial trauma can cause serious spinal fractures that carry a high risk for delayed paralysis and perioperative complications. 6 –10 We recently observed that among elderly people with DISH-related spinal fractures (mean age 77.1 ± 10.1 years), 47.6% were affected by delayed paralysis. 6 We examined these injuries by computed tomography (CT) with multiplanar reformatting (CT-MPR) and concluded that spinal fractures in regions with posterior-column ankylosis led to three-column injuries and delayed paralysis. As with fractures in long bones, the long lever arm formed by the ossified spine increases the mechanical stress at the fracture, destabilizing the spine even further. Therefore, multiple anchors should be placed during fixation to stabilize the fractured segments. Caron et al. 9 recommend extending spinal fixation to three vertebrae above and below the fractured segments in patients with ankylosing spinal disorders (ASDs) to avoid implant failures. However, including more levels in the fixation increases the invasiveness and length of the operation, which might contribute to the high rates of perioperative complications reported (26–84%) in these elderly patients. 6 –10
Percutaneous pedicle screws (PPSs) are widely used in various spinal fixation surgeries, 11 –13 in part because PPS fixation is less invasive than conventional open procedures. Using PPS fixation for spinal fractures with DISH might decrease perioperative complications by minimizing the burden of surgery. However, there is little information about the effectiveness of PPS fixation for fractures in DISH. Although a few case series have reported that PPS fixation is effective for spinal injuries with ASDs, 14,15 these case series involved only a small number of subjects or lacked controls. 15,16
This retrospective study was conducted to validate the effectiveness of PPS fixation specifically for DISH-associated spinal fractures and to compare surgical outcomes between PPS and conventional open fixation using the cohort from the same database. 6
Materials and methods
This study was approved by our institutional review board. We retrospectively evaluated medical records and outcomes for patients who underwent surgery for DISH-related spinal injuries at a university hospital or its affiliated hospitals. Inclusion criteria for this study were the presence of DISH, defined as flowing ossification along the anterolateral aspect of at least four contiguous vertebral bodies, 1 and an injury in the ossified spine—specifically a fracture in the thoracolumbar spine—that was treated by posterior spinal fixation with minimum 12 months of follow-up. Patients were excluded if they had ankylosing spondylitis or a prior spinal surgery. The 41 patients who met the inclusion criteria (30 men and 11 women; mean age at injury 77.2 ± 9.6 years) were divided according to the surgical technique, either PPS fixation (P group) or the conventional open posterior fixation (O group). The surgical technique was decided by each surgeon. PPS fixation was performed in 4 hospitals and conventional open posterior fixation was performed in 12 hospitals. In two hospitals which performed PPS fixation, the surgical technique was changed from the conventional open posterior fixation to PPS fixation. Therefore, patients in the O group were treated from 2009 to 2015 and patients in the P group were treated from 2013 to 2017. All the patients in both groups who had neurological deficit underwent midline open decompression of the spinal canal with spinal fixation. There were no cases who underwent minimally invasive decompression, that is, endoscopic decompression. In the O group, 6 subjects underwent bone graft and decortication at the fracture level and 19 patients within the fusion area. Bone cement was not used for screw augmentation in the present study, because this application is not approved in Japan. In the P group, neither bone grafting nor posterior decortication was performed in any case.
Preoperatively, the fracture type was evaluated by CT-MPR in all patients and categorized according to the AOSpine thoracolumbar spine injury classification. 17 We compared demographic data, fracture type according to the AOSpine thoracolumbar spine injury classification, the presence of three-column injury, cause of spinal injury (high-energy injury or not), and preoperative condition between the two groups. A high-energy injury was defined as an injury caused by a fall from over 15 ft 8 or by traffic accident. The preoperative condition was evaluated by the American Society of Anesthesiologists (ASA) physical status classification, 18 a relatively simple system that can predict morbidity and mortality in general surgical procedures 15 –17 and is typically used for every surgical patient. Neurological status was evaluated by Frankel grade 19 at the time of injury, at the first hospital visit, and at the final follow-up. We also assessed neurological improvement at the final follow-up, the number of levels fused, operative time, estimated blood loss, and surgical complications. Status of bony fusion was assessed by lateral dynamic radiography in 16 patients and CT-MPR in 25 patients, 12 months after the surgery.
Data were analyzed for significance using SPSS Statistics 22 (IBM Corp, Armonk, New York, USA). Associations between the groups were compared by χ 2 and Mann–Whitney U tests. The value of p < 0.05 was considered significant.
Results
Demographics
There were no significant differences between the O and P groups in age, gender, history of diabetes mellitus, percentage of high-energy injuries, preoperative ASA scores
Demographic characteristics and clinical features by group.
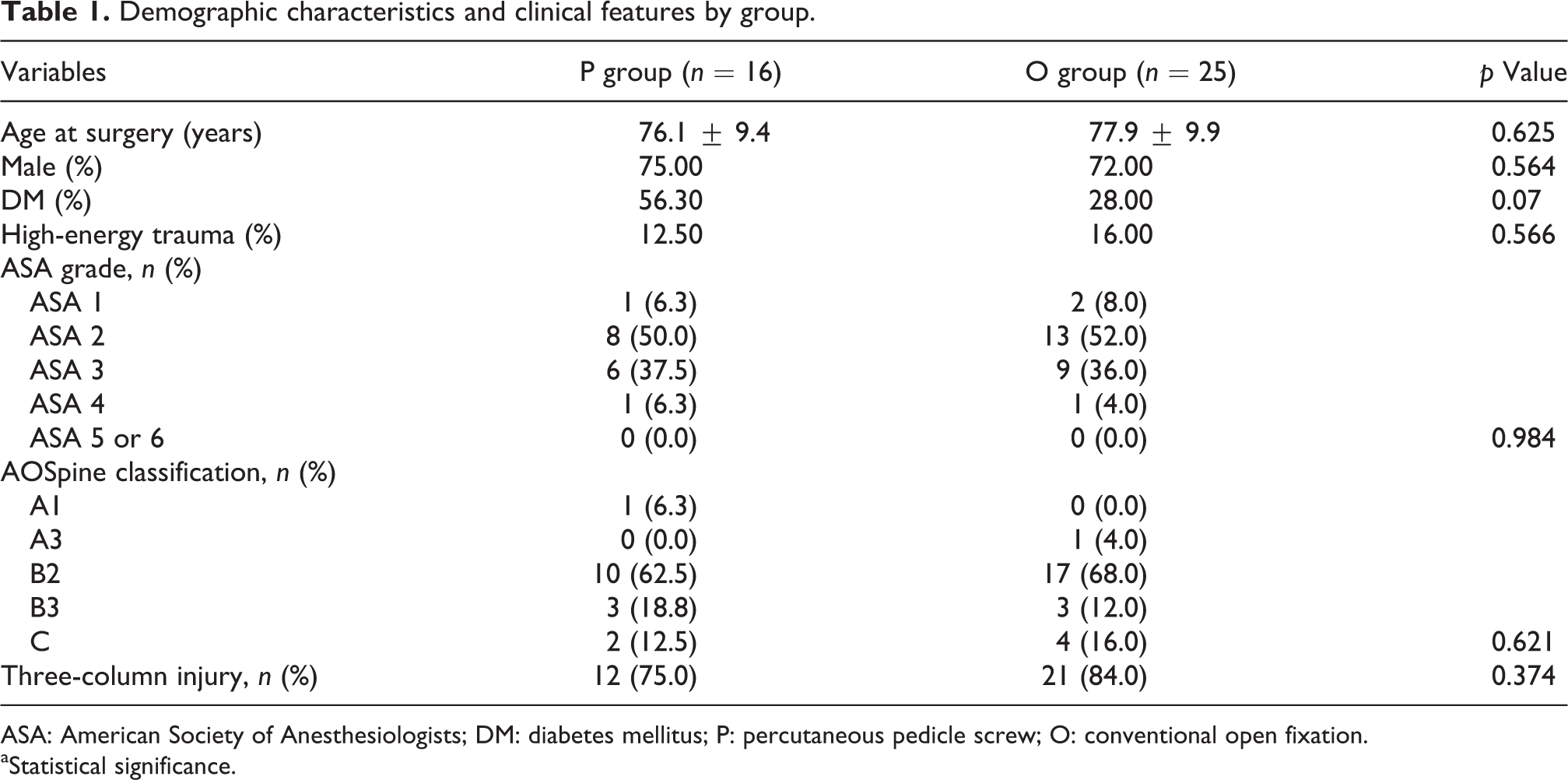
ASA: American Society of Anesthesiologists; DM: diabetes mellitus; P: percutaneous pedicle screw; O: conventional open fixation.
aStatistical significance.
Neurological status
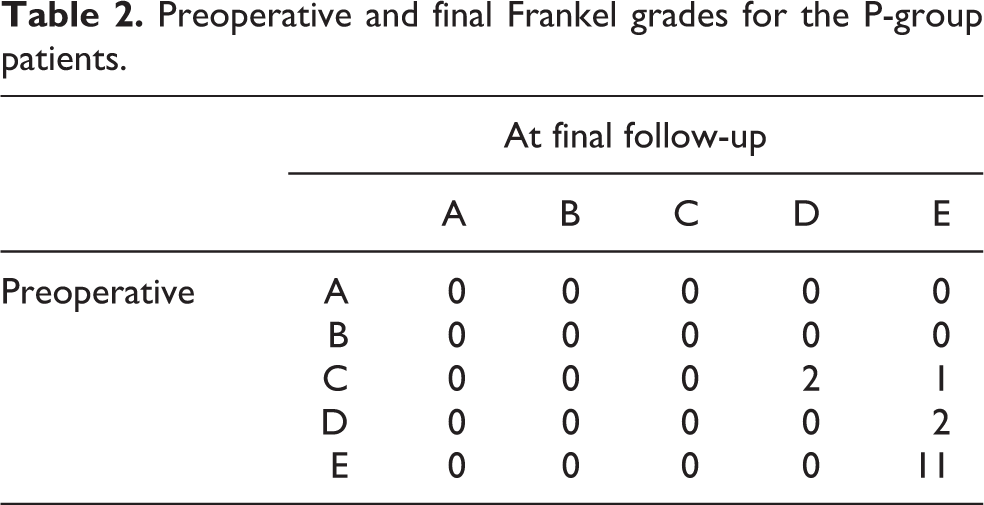
Preoperatively, the P group included 3 patients with Frankel grade C, 2 with grade D, and 11 with grade E. The O group included 1 patient with Frankel grade B, 13 with grade C, 6 with grade D, and 6 with grade E. Thus, the preoperative neurological status was significantly better in the P group than in the O group (p = 0.032). Frankel grades at the final follow-up indicated significant neurological improvement in both groups, with 2 patients with grade D and 14 with grade E in the P group, while the O group had 1 patient each for grades A and B, 5 each for grades C and D, and 14 with grade E (p = 0.154). The percentage of patients that showed significant neurological improvement at the final follow-up was similar in the two groups (33.3% in the P group and 40.0% in the O group, p = 0.410; Tables 2 and 3).
Preoperative and final Frankel grades for the P-group patients.
Preoperative and final Frankel grades for the O-group patients.

Treatment
The mean fusion length was similar in the two groups (5.1 ± 0.8 levels in the P group and 4.9 ± 1.2 in the O group). However, the mean operation time was significantly shorter for the P group (168.1 ± 46.7 min) than for the O group (224.6 ± 49.8 min; p = 0.001), and the mean estimated blood loss was significantly less in the P group (133.9 ± 116.5 g) than in the O group (499.9 ± 368.5 g, p = 0.006; Table 4).
Surgical parameters by group.

aStatistically significant.
Complications
In the P group, two intraoperative pedicle screw loosening, two pneumonia, and two urinary tract infection were observed, and one decubitus ulcer and one gastric ulcer were observed during the period (Table 5). In the O group, there were five instances of pneumonia, three of surgical-site infection (two superficial infection and one deep), two of decubitus ulcer, and one each of postoperative screw loosening, urinary tract infection, and hyper-bleeding shock. Three patients in the O group died within 1 year of surgery; the deaths were due to hypovolemic shock, respiratory failure, and pneumonia. Because bony fusion was obtained in all the patients examined 12 months after surgery, there were no cases of nonunion in either groups. Only one case required additional surgery; this was a patient in the O group who developed a deep surgical site infection.
Surgical complications by group.

PS: pedicle screw.
Case presentation
An 84-year- old female, having multiple comorbidities, such as breast cancer, diabetes, hypertension, and dementia, fell down from standing position in her house. She presented a medical institution without any neurological deficit a day after injury. She was diagnosed with the spinal fracture at T10 (Figure 1) and had PPS fixation from T8 to T12 without decompression, which was performed 6 days after injury (Figure 2). The operation time was 59 min, and the estimation of blood loss was less than 10 g. Six months after the surgery, bony fusion was seen by plain radiograph and CT scan of thoracic spine (Figure 3).

Case 1: An 84-year-old female. (a) A lateral plain radiograph of the thoracic indicates the fracture line was seen at T10 vertebral body. A white arrow indicates the fracture line. (b) A sagittal view of the thoracic spine by CT scan shows three-column fractures at T10. A white arrow indicates the fracture line. CT: computed tomography.
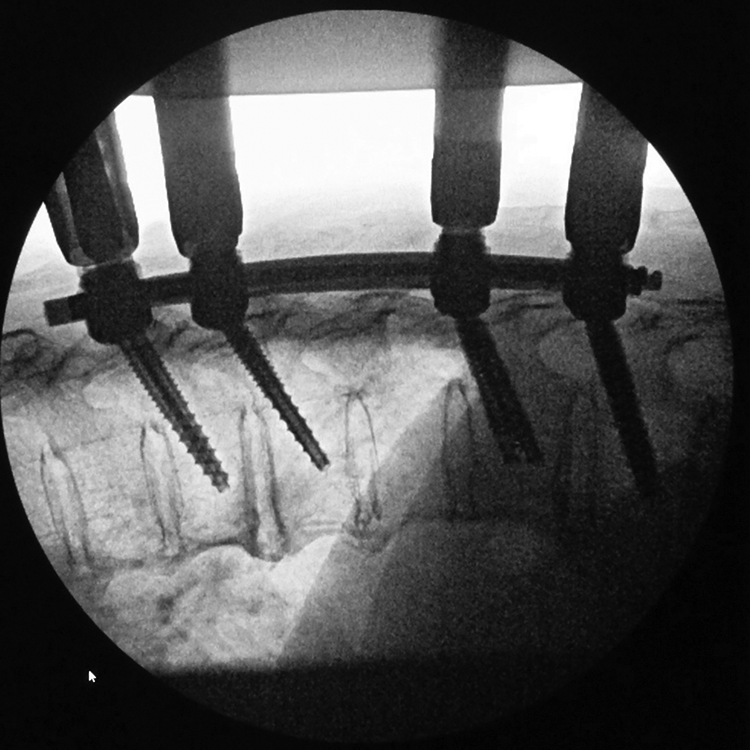
Intraoperative fluoroscopy. Percutaneous pedicle screw fixation from T8 to T12 was performed under fluoroscopy.

Six months after surgery, lateral plain radiograph of the thoracic spine shows bony fusion at T10.
Discussion
PPS fixation for thoracolumbar injury
Hu et al. conducted a cross-sectional database study of the incidence of spinal fractures in 1996 20 and reported an annual incidence of 64 per 100,000 people, with 75% of the fractures occurring in the thoracolumbar region. Minimally invasive spinal fixation techniques are now widely used for spinal fractures, and PPS fixation is especially useful for fractures in the thoracolumbar region. Several studies have reported the advantages of PPS fixation. 21 –23 McAnany et al. conducted a systematic literature review and meta-analysis 23 comparing the surgical outcomes between open and percutaneous fixation for traumatic thoracolumbar fracture and noted that the benefits of minimally invasive fixation, such as the relatively low intraoperative blood loss and operating time in percutaneous surgeries, are especially important when treating patients with multiple injuries. In the present study, blood loss and operation time in the P group were lower than those in the O group. DISH patient with spinal fracture may be a good candidate for PPS fixation because (1) they do not need bone grafting, (2) they do not lose range of motion because segments are already fused by hyperostosis, (3) majority of patients are elderly with general comorbidities, and (4) removal of the spinal implants for the purpose of retrieving the segmental motion 24 is not mandatory.
Previous studies of PPS fixation for spinal fractures in ASDs
DISH and ankylosing spondylitis (AS) are both ASDs, and they are often grouped and analyzed as a single condition. However, their etiologies and characteristics are quite different. Although the outcomes have not been described for the PPS fixation of fractures in DISH, four articles describe surgical outcomes for the PPS fixation of spinal fractures in ASD (Table 6). 14,15,25,26 Two of these, Yeoh et al. 14 and Sedney et al., 25 did not comment on the percentage of DISH patients in the ASD cohorts. Yeoh et al. and Nayak et al. 15 reported favorable outcomes and low complication rates (20–36%) for the PPS fixation of spinal fractures with ASD but did not compare the outcomes between PPS fixation and conventional fixation techniques. Sedney et al. recently compared percutaneous and conventional open fixation techniques for spinal fractures in ASD and reported shorter operative times, lower estimated blood loss, and fewer blood transfusions with PPS fixation. The follow-up period was too short to evaluate postsurgical mortality. In the present study, mortality rates for DISH patients with spinal fractures were higher with conventional open fixation than with PPS fixation, which had no postoperative deaths. The results of this study emphasized the advantage of PPS fixation for DISH patients with spinal fracture. In the thoracolumbar spine, the surgical indications for conventional open fixation are limited but include fractures with a large bony defect, which require a posterolateral bone graft, or with severe dislocation, which require open reduction.
Studies of outcomes for PPS or open fixation for spinal fractures with DISH or AS.
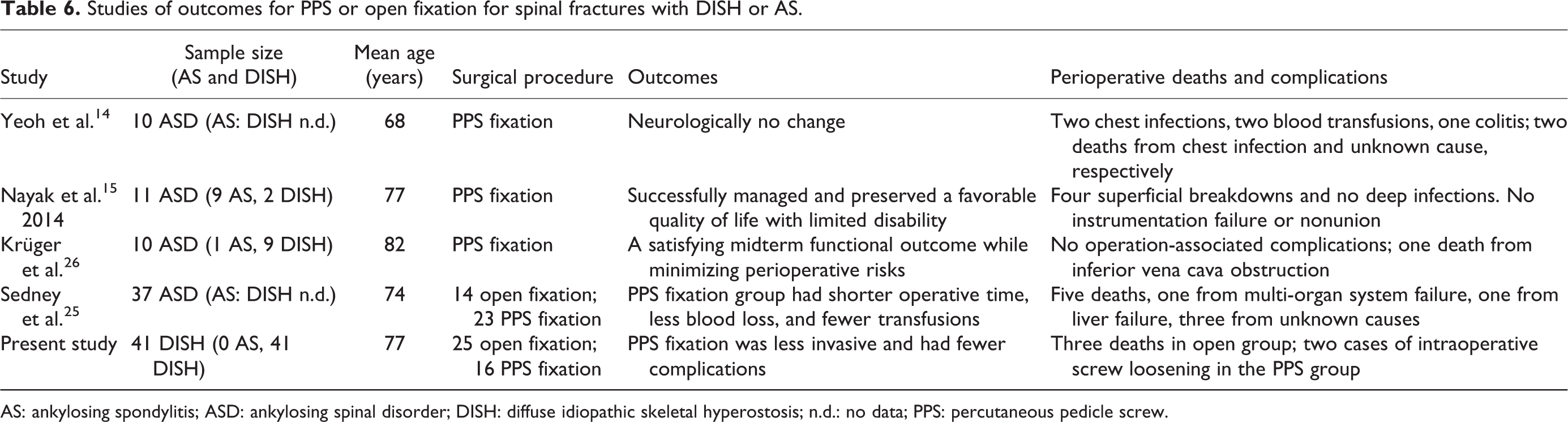
AS: ankylosing spondylitis; ASD: ankylosing spinal disorder; DISH: diffuse idiopathic skeletal hyperostosis; n.d.: no data; PPS: percutaneous pedicle screw.
Since patients with DISH tend to have poor bone quality (unless the bone mineral density is good 27 ), the spinal fractures are often treated by multilevel fusion to ensure stable fixation. In 2010, after conducting a single-center retrospective study of spinal fractures in ASD (the largest cohort to date), Caron et al. recommended extending posterior segmental fixation at least three levels above and below the injured segment for stronger, more reliable fixation. In contrast, a 2014 study by Krüger et al. 26 reported favorable outcomes for PPS fixation for spinal fractures in an ASD cohort (most of whom had DISH), with no instrumentation failures despite a surprisingly short mean fusion length of 1.8 segments. Thus, the optimal fixation length for the stable fusion and instrumentation of spinal fractures in DISH is still unclear.
Limitations of previous four studies 14,15,25,26 were small sample size (Yeoh: 10; Nayak: 11; and Krüger: 10 patients), subjects including AS (Nayak and Krüger), lack of control (Yeoh, Nayak, and Krüger), no description of fracture pattern (Yeoh, Nayak, and Sydney), and short follow-up. The present study demonstrated the advantages of PPS fixation by exclusively evaluating DISH-related spinal fractures, and by comparing PPS fixation with conventional open fixation in the largest cohort. Although both DISH and AS are ankylosing disorders, AS cases should be omitted when assessing the efficacy of PPS fixation for DISH because of the different etiologies, characteristics, and fracture patterns of the two conditions. The fracture line, which is generally at disk level in AS, runs through the vertebral body in DISH, 6,8,28 indicating that the mechanism of fracture differs. Ossification in DISH is characterized by a hyperostosis pattern that is often described as a flowing candle wax morphology, 1 while the ossification in AS is thicker and includes the intervertebral disk. The distinct ossification patterns of AS and DISH are likely to affect the characteristics and response of fractures in each condition.
In the present study, there were no significant differences in age or gender between the P and O groups. However, the O group had more severe neurological deficits prior to surgery. This is probably because most of the cases in the O group were from an older series, while the P group consisted mostly of more recent cases. In 2016, after a retrospective survey to characterize the spinal fractures in DISH, 6 we reported that injuries at ankylosed posterior elements of the spine led to three-column instability and predicted delayed paralysis. Therefore, we adopted a strategy of early surgical fusion by PPS for DISH-associated spinal fractures with three-column instability, to stabilize the spine and prevent neurological deterioration. This difference in strategy could have affected the neurological status at the time of surgery.
Complications
There was no significant difference between the P and O groups in the number of fused segments, and neurological recovery was similar in the two groups. PPS fixation tended to have fewer complications than conventional open fixation, consistent with previous reports. 14,15,25 Importantly, surgical site infections occurred only in the O group. Many patients had comorbidities, including diabetes, making surgical site infection a significant concern. There were three deaths after surgery in the O group, but there were no deaths in the P group. Pneumonia and other respiratory complications are common perioperative complications. 6,9 Procedures that require more time in surgery 25 and longer hospital stays, such as conventional open fixation, might contribute to a high frequency of perioperative complications.
Although the P group had fewer complications, there were two cases of intraoperative PPS loosening due to poor bone quality and the difficulty of keeping the screw heads properly positioned on the ankylosed segments while applying the rods. Thus, a surgeon dealing with a fracture in DISH must give extra attention to the screw placement to avoid intraoperative screw loosening. To obtain better bone purchase, cement augmentation 29,30 or grove entry technique 31 may be used in the patient with poor bone quality.
Study limitations
One limitation of this study is its retrospective nature; another is the lack of preoperative and postoperative patient-oriented outcome measures even with a relatively large number of patients. Most patients presented with acute trauma or paralysis, which makes it difficult to obtain preoperative patient-oriented questionnaires. Another limitation is that since the cases in the P group were more recent than those in the O group, they were more likely to be treated by fusion surgery by PPS at an early stage to prevent late paralysis. This study bias probably accounted for the higher incidences of neurologic injury and surgical site infection in the O group. The early intervention in the P group may have affected neurological status at the time of surgery and accounted for its decreased complication, surgical infection, and mortality rates. Ideally, a well-designed prospective study with a larger number of subjects would be most helpful in determining the optimal treatment for the unique issues of spinal fractures in DISH.
Conclusion
Both methods, PPS fixation and conventional open posterior fixation, provided similar neurological improvement for DISH-related spinal fractures. However, the PPS fixation method was much less invasive, and the complication rate was lower than with conventional open posterior fixation.
There were some instances of intraoperative PS loosening with PPS fixation, which highlights the importance of careful PS placement in cases of DISH.
Footnotes
Acknowledgments
The authors thank Kazuhiro Chiba (Department of Orthopaedic Surgery, National Defense Medical College), Yuichiro Takahashi (Department of Orthopaedic Surgery, Sano General Hospital), Michihiro Kamata (Department of Orthopaedic Surgery, Keiyu Hospital), Tetsuya Kuramoto (Department of Orthopaedic Surgery, Saitama City Hospital), Katsuki Kono (Department of Orthopaedic Surgery, Kono Orthopaedic Surgery Clinic), Masayuki Ishikawa (Department of Orthopaedic Surgery, International University of Health and Welfare), Hikata Tomohiro (Department of Orthopaedic Surgery, Kitasato University, Kitasato Institute Hospital), Ken Ninomiya and Satoshi Suzuki (Department of Orthopaedic Surgery, Tokyo Dental College, Ichikawa General Hospital), Kunimasa Okuyama (Orthopaedic Surgery, Sizuoka City Shimizu Hospital), Kazuya Kitamura (Department of Orthopaedic Surgery, Saiseikai Yokohamahi Tobu Hospital), Kenya Nojiri (Department of Orthopaedic Surgery, Isehara Kyodo Hospital), Yohei Takahashi (Department of Orthopaedic Surgery, Shizuoka Red Cross Hospital), Yosuke Horiuchi (Japan Community Health care Organization, Saitama Medical Center), Tomoki Ieda (Department of Orthopaedic Surgery, Ashikaga Red Cross Hospital), Seiji Ueda (Department of Orthopaedic Surgery, Kawasaki municipal Hospital), Kiyoshi Inoue (Department of Orthopaedic Surgery, Saiseikai Mukoujima Hospital), Daisuke Nakashima and Akio Iwanami (Department of Orthopaedic Surgery, Keio university), all doctors participating in the Keio Spine Research Group for their help with this study, and Yuji Nishiwaki (Department of Environmental and Occupational Health, School of Medicine, Toho University) and Midori Morishita, Masaki Tezuka, and Shigeru Yanagimoto (Department of Orthopaedic Surgery, Saiseikai Central Hospital) for their kind help and comments on this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.