
Abstract
Introduction
The anterior osteophyte is a bony hardening of the ligaments in areas where they attach to the spine. Diffuse Idiopathic Skeletal Hyperostosis (DISH) can be manifested as huge, multilevel anterior osteophytes of the cervical spine. The incidence of DISH is variable and ranges about 10–20% of the general population.1,2 However, DISH is generally asymptomatic. Studies have found that approximately 10% of patients older than 65 years commonly had anterior osteophytes of the cervical spine and more than 17% were found with DISH complaints of dysphagia.3,4 A previous literature review did not offer guidelines for the surgical treatment of these large anterior osteophytes of the cervical spine. This review article presents the current surgical treatment options for large anterior cervical osteophyte or DISH causing dysphagia.
The authors aim to summarize the current evidence on surgical treatment for large bridging osteophytes of the anterior cervical spine from Diffuse Idiopathic Skeletal Hyperostosis (DISH) that can cause dysphonia, dyspnea, and/or dysphagia. The authors propose a treatment algorithm for management because to date there have been only case reports and retrospective studies.9–18
Methods
Literature search
Literature search was performed to collect the articles published in PubMed using the MeSH terms “Anterior Cervical Osteophyte,” “Diffuse Idiopathic Skeletal Hyperostosis (DISH),” “Dysphagia,” and “Treatment”. Articles published between January 2000 and February 2020 were selected for further screening. Additional manual searches were performed using relevant references in selected articles concerning anterior cervical osteophytes causing dysphagia.
Inclusion and exclusion criteria
Randomized controlled studies, observational studies, and case series were included in this review. There was no preference in the type of study (retrospective/prospective), and all studies had to be published in the English language. Case reports and technical reports were excluded. All the articles were screened for titles and abstracts. Selected articles were studied in detail, and the relevant data were recorded.
Data extraction
The following data were recorded: (1) Study ID: including author(s) and journal name; (2) year of publication; (3) type of study design; (4) study sample size: Number of patients; (5) average patient age (mean ± SD); (6) clinical findings of symptomatic DISH; (7) nationality; (8) radiologic findings (level of the cervical spine where the bridging osteophytes occurred); (9) surgical treatment: Anterior cervical osteophytectomy alone without fusion, multilevel cervical oblique corpectomy, anterior cervical discectomy without plating, anterior cervical discectomy and fusion (ACDF) plus plate, anterior cervical osteophytectomy + stand-alone polyetheretherketone (PEEK) cage without plating, and anterior cervical osteophytectomy + PEEK plus plate; (10) clinical results; and (11) follow-up duration.
Results
The PubMed search resulted in the identification of 117 articles that met the initial screening criteria. Detailed analysis found 40 matching articles; however, when applying the full inclusion and exclusion criteria, only 11 articles were determined to be eligible for this review. All articles reported an incidence of secondary dysphagia associated with DISH in elderly patients (average 65 years). Clinical findings were dysphagia or respiratory compromise with the most common level of bridging osteophytes of the cervical spine at C3–C5. The nationality of the authors showed 3 articles from USA, 3 articles from Germany, 2 articles from Japan, and 1 article each from India, Italy, and United Kingdom. Surgical treatment showed 10 articles for anterior cervical osteophytectomy without fusion, 1 for multilevel cervical oblique corpectomy, 1 for anterior cervical discectomy with ACDF (plus plate), and 1 article for anterior cervical osteophytectomy + stand-alone PEEK cage without plating and anterior cervical osteophytectomy + PEEK plus plate. All of the articles reported significantly improved clinical results following the treatment without recurrence; only 1 study reported post-operative complication, stroke, and Horner’s syndrome, which improved at 6 months. The follow-up duration was 3–70.3 months.
Demographic data analysis
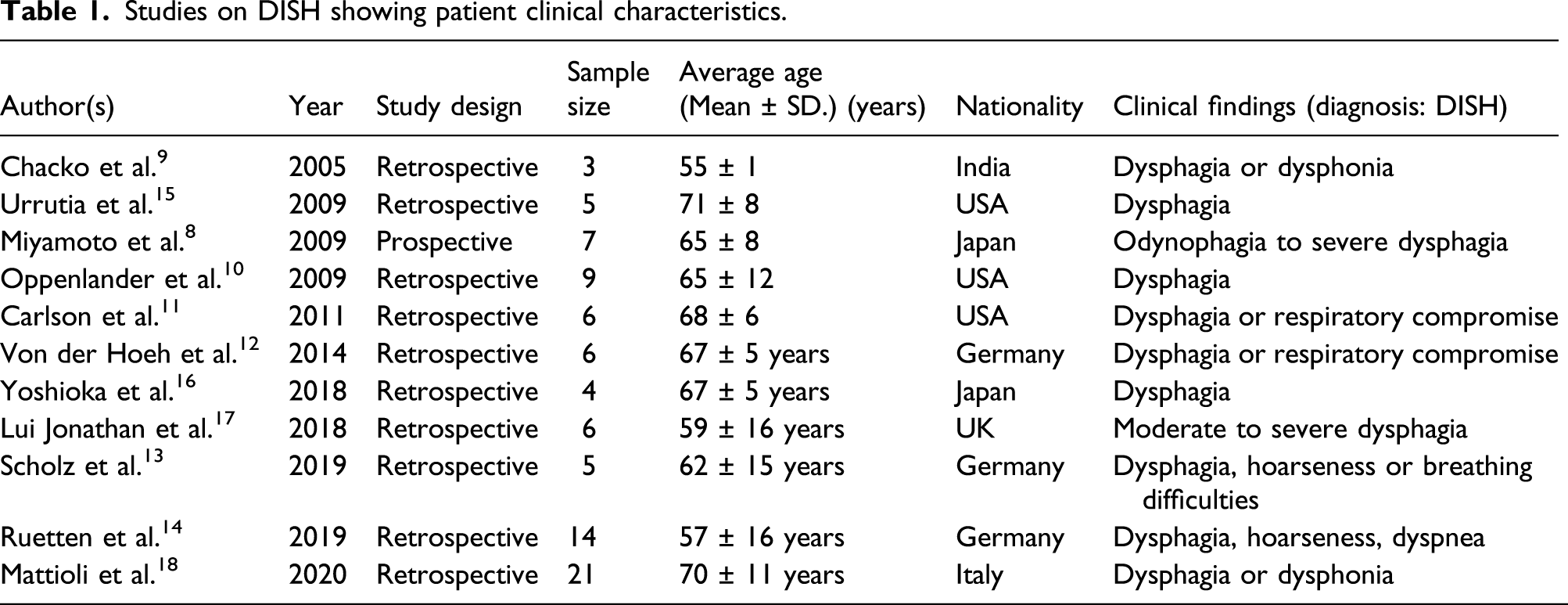
Studies on DISH showing patient clinical characteristics.
Study design
Ten studies were retrospective because DISH was asymptomatic; there were only a small number of patients with DISH-related dysphagia.5,6,9–16 There were no randomized controlled trial studies for this condition. Only the study of Miyamoto et al. had a prospective study design. 8
Age
All the studies found that elderly patients were associated with DISH with dysphagia5–15 and 3 reported this combined with respiratory compromise.9,10,13 The study by Chacko et al. 9 showed the lowest average age (55 ± 1 year), while Miyamoto et al. 8 and Oppenlander et al. 10 found that age >65 years was a strong factor in the development of DISH.
Nationality
All of the studies showed the nationality of the study for DISH with dysphagia5–15 and combined with respiratory compromise.9,10,13 The idiopathic cause of DISH was not related with nationality due to the small sample size.
Clinical findings associated with DISH.
The most common clinical presentation was dysphagia. Respiratory compromise associated with moderate to severe dysphagia was reported by Carlson et al., 11 Von der Hoeh et al., 12 and Scholz et al. 13 Other studies have shown an association between anterior cervical osteophyte causing secondary dysphagia with hoarseness, notably Scholz et al. 13 and Ruetten et al. 14
Surgical treatment and outcomes
Studies with different surgical treatments of DISH and outcomes.

Discussion
Comparison of surgical techniques for DISH anterior cervical osteophytes causing secondary dysphagia.

Recurrent cervical osteophytes were rare and it developed slowly in long-term follow-up over 10 years14,28–30 Routine additional fusion was therefore discussed not only due to possible operation induced instability, but also because segmental mobility can promote the further development of osteophytes.14,28–30 Surgical resection of cervical osteophytes was a sufficient method for treating spondylogenic dysphagia but prophylaxis of recurrent anterior cervical ossifications was limited experience and no precise guidelines. 14 However, prophylaxis treatment using indomethacin or radiation also appears to be an option.
DISH-related respiratory problems are rare.31–33 When present, it was believed to be due to compression of the airway by large hypertrophic anterior cervical osteophytes. 31 Reported clinical symptoms include hoarseness, stridor, and dyspnea to acute respiratory distress.31,32 Large osteophytes can potentially compress the posterior pharyngeal wall of the esophagus and trachea. Hypertrophic anterior cervical osteophytes at C4–C5 level was the narrowest region and felt to be the cause of the airway obstruction.31,33 The esophagus was the first affected structure. It was under direct compression and entrapment, resulting in dysphagia.31,34 Esophageal compromise can then be followed by compression of the trachea that can result in respiratory compromise due to the excessively large osteophytes. Large hypertrophic anterior cervical osteophytes can cause direct compression of the trachea, as well as entrapment and compromise of both laryngeal nerves with bilateral vocal cord immobility. 34 The result was dysphonia and stridor. Patients who have severe aspiration with acute respiratory distress may require urgent tracheotomy for airway management. 31 The surgical excision of the osteophytes in the reported case was successful and effective with improvement in the dysphagia and respiratory discomfort.
Anterior cervical osteophytes or DISH combined with cervical myelopathy requires spinal cord decompression.
35
The AO Spine guidelines (AO Spine North America) and the Cervical Spine Research Society (CSRS) suggest treatment options for CSM.36,37 They suggest anterior cervical osteophytectomy without fusion for patients with dysphagia without cervical myelopathy. For patients with DISH and cervical myelopathy, they recommend anterior cervical discectomy and fusion (ACDF) plus plating. The authors propose the treatment algorithm shown in Figure 1. Suggested algorithm for decision making and surgical treatment of dysphagia caused by DISH.
Overall post-operative complications after anterior cervical spine surgery in current systematic review 38 found dysphagia (5.3%), recurrent laryngeal nerve palsy (1.3%), infection (1.2%), hematoma (1%), CSF leak (0.5%), Horner’s syndrome (0.4%), vertebral artery injury (0.4%) and esophageal perforation (0.2%). 38 However, our review articles in DISH causing secondary dysphagia found less reported in the complications after anterior cervical osteophytectomy. In all patients whom diagnosed with DISH presenting by dysphagia or respiratory compromise, only the study by Chacko et al. 9 reported postoperative Horner's syndrome, which had spontaneous improvement at 6 months. Another study by Carlson et al. 11 showed post-operative stroke. Post-operative persistent dysphagia was improved during the duration of 3–70.3 months in our review.
All patients with DISH causing secondary dysphagia could be evaluated by internal medicine and ENT physicians for the risks to carry on surgery and conducted airway management before operation. Our recommendations for diminishing and preventing the post-operative complications are urging the surgeon to perform adequate surgical approach-incision, using microscope-assisted surgery for better visualization and decreasing the risk of adjacent structure injuries during anterior cervical osteophytectomy or discectomy such as airways, esophagus, vertebral artery, and CSF leakage. Patients with risk factors (DISH, OPLL, long operative time (more than 5 h), multi-level surgery (more than 3 levels), and therapeutic heparin administration) might relate to acute post-operative retropharyngeal hematoma and airway complications. 39 We highly recommended to check and stop the possible occult bleeding before closure. Effective intraoperative hemostasis after anterior cervical osteophytectomy was required to prevent post-operative retropharyngeal hematoma. 39
Clinical case
A 54-year-old female presented with DISH causing dysphagia with cervical radiculopathy. She had progressive dysphagia over 3 years. Her general physical examination was normal without respiratory compromise. She had positive Spurling’s test (bilateral dermatomal C5 and C6 radiculopathy). Plain radiographs demonstrated prominent anterior cervical osteophytes at C3–6 (Figure 2(a)). Sagittal MRI T2-weighted images showed prominent large anterior cervical osteophytes at C3–6 which compressed the pharyngoesophageal structure (Figure 2(b)). The axial images at C5–C6 (Figure 2(c)) and C6–C7 (Figure 2(d)) showed bilateral foraminal stenosis with C6–C7 nerve root compression. A 54-year-old female sustained DISH causing secondary dysphagia with cervical radiculopathy. Plain X-ray (a) and MRI T2-weighted sagittal view demonstrated large anterior cervical osteophytes (red asterisk) at C3-6 compressing the pharyngoesophageal structure. (b) Axial MRI images of C5–C6 (c) and C6–C7 level (d) showed foraminal stenosis compressing the corresponding nerve roots. Intra-operative finding demonstrated the large anterior cervical osteophytes (white asterisk). (e) Osteophytectomy C3–6 and discectomy C5–C7, (f) fusion with bone grafts (g) plus plate fixation were performed. Plain X-ray (h) at 3-years follow-up period.
We used the Smith–Robinson approach to expose the anterior cervical spine from C3 to C6. Large prominent anterior cervical osteophytes were found (Figure 2(e)). We performed an osteophytectomy from C3 to C6, discectomy C5–C7 (Figure 2(f)), and fusion with iliac autogenous bone graft (Figure 2(g)) plus plate (Figure 2(h)). There were no iatrogenic neurovascular injuries, and the alignment was acceptable. Complete bony union was achieved at 6 months post-operatively. The patient had significant improvement clinically and radiographically (Figure 2(h)) without recurrence of dysphagia at 3-years follow-up.
A previous study by Liawrungrueang et al. 40 reported on an 81-year-old patient with a “giant beak-like lesion” from DISH causing dysphagia. The osteophytic lesion was anterior to the C3 and C4 vertebrae, causing compression of the pharyngoesophageal segment. Patient refused anterior cervical osteophytectomy. He had progressive dysphagia and recurrent aspiration pneumonias, impacting his quality of life.
In summary, we examined the current evidence on surgical management of large bridging osteophytes of the anterior cervical spine secondary to DISH. We found that surgical intervention appears to be safe, effectiveness and halts the progression of disease. We believe that our algorithm will guide surgeons in their decision-making process. We fully expect that this algorithm will be modified and revised in the future, as more knowledge and novel treatments regarding this condition becomes available.
Conclusion
We conclude that large osteophytes due to DISH can cause dysphagia, but it remains unclear why some with such osteophytes remain asymptomatic, whereas others with smaller osteophytes are symptomatic. Surgical intervention with anterior cervical osteophytectomy has the advantage of improved outcomes. Cervical spine motion is likely to be impacted if a fusion is also performed. However, the fusion may prevent a recurrence of the osteophytes. Further randomized controlled studies and studies with long-term outcomes are required to determine the optimal procedure for anterior cervical osteophytectomy with or without fusion.
Footnotes
Acknowledgements
The authors would also like to express our thanks to the Research Unit, Department of Orthopaedics, Faculty of Medicine, Chiang Mai University for their support.
Author Contributions
K. Daniel Riew and Torphong Bunmaprasert: Supervision, Writing - Review & editing; Jakkrit Keeratiruangrong and Nantawit Sugandhavesa: Resources, Data curation; Wongthawat Liawrungrueang: Corresponding author, Conceptualization, Methodology, Visualization, Writing-original draft , Review & editing. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.