
Abstract
Study Design
Retrospective multicenter study.
Objective
The purpose of this study was to compare the prognosis of elderly patients with injuries related to cervical diffuse idiopathic skeletal hyperostosis (cDISH) to matched control for each group, with and without fractures.
Methods
The current multicenter study was a retrospective analysis of 140 patients aged 65 years or older with cDISH-related cervical spine injuries; 106 fractures and 34 spinal cord injuries without fracture were identified. Propensity score–matched cohorts from 1363 patients without cDISH were generated and compared. Logistic regression analysis was performed to determine the risk of early mortality for patients with cDISH-related injury.
Results
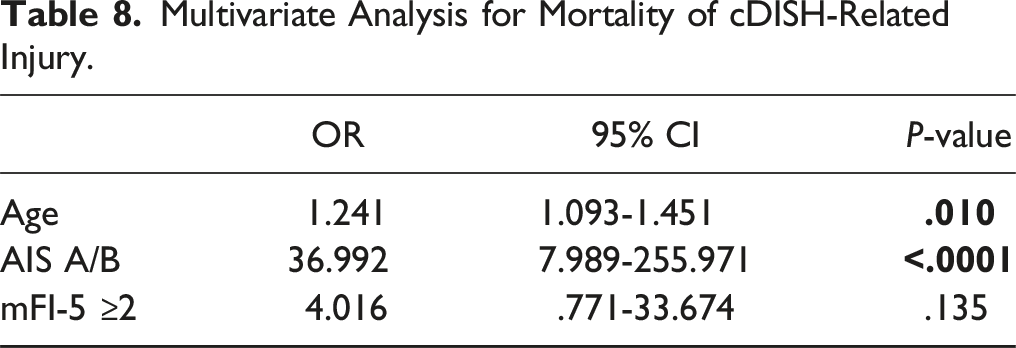
Patients with cDISH-related injuries with fracture did not differ significantly in the incidence of each complication and ambulation or severity of paralysis compared to matched controls. In patients with cDISH-related injury without fracture, those who were nonambulatory at discharge comprised 55% vs 34% of controls, indicating significantly poorer ambulation in those with cDISH-related injuries (P = .023). There was no significant difference in the incidence of complications and ambulation or paralysis severity at 6 months as compared with controls. Fourteen patients died within 3 months. Logistic regression analysis identified complete paralysis (odds ratio [OR] 36.99) and age (OR 1.24) as significant risk factors for mortality.
Conclusions
The current study showed no significant differences in the incidence of complications, ambulation outcomes between patients with cDISH-related injury with fracture and matched controls, and that the ambulation at discharge for patients with cDISH-related injury without fractures were significantly inferior to those of matched controls.
Keywords
Introduction
The catastrophic consequences of diffuse idiopathic skeletal hyperplasia (DISH)–based spinal fractures have come to the forefront of attention in recent years because of the increasing prevalence of DISH secondary to the aging of the general population worldwide.1,2 DISH can occur in the entire spine, and ossification occurs primarily in the anterior longitudinal ligament. 3 The resulting fused spinal segment becomes a long lever arm that is subject to traumatic forces. Thus, not only do traumatic impacts that would not result in injury in a normal flexible spine cause complex disability for the DISH spine, but fractures at the DISH fusion site also have greater instability as long bone fractures. As a result, this injury is prone to neurologic deficits,4–6 and even if paralysis is avoided immediately after injury, there is a high risk of delayed neurologic problems. 2 Thus, DISH-related spinal injuries have a distinctive character.
The subgroup of cervical DISH (cDISH) fractures is difficult to treat. Patients are not only older by nature but also have more medical comorbidities. 7 Conservative treatment carries a risk of delayed palsy, and perioperative complications are common. 7 Furthermore, mortality is high in patients with DISH cervical spine injuries.4,6,8,9 In a previous report, Ozpinar et al 2 performed surgical treatment for a DISH fracture and reported the largest surgical cohort of 48 patients. They showed that preoperative American Spinal Injury Association (ASIA) grade and American Society of Anesthesiologists score were risk factors for inability to walk at discharge, and the subaxial injury classification score was a risk factor for increased 30-day mortality. Katoh et al 5 compared 84 cDISH fractures with 201 thoracolumbar DISH fractures and found that more cDISH fracture cases were associated with ossification of the posterior longitudinal ligament (OPLL), disc-level fracture, a higher rate of spinal cord injury (SCI), and a higher mortality rate. Thus, patients with cDISH injuries represent a high-risk population for treatment.
However, it is unclear to what extent older adults with cDISH-related injuries are at higher risk compared with the general elderly population. In addition, previous studies have focused on fractures of the DISH mass itself, ignoring SCI without fractures. SCI without fracture is a clinically important subgroup of cervical spinal cord injuries, especially in elderly individuals. DISH-based SCI without fracture can be as severe as that with fractures because of the instability resulting from a long lever arm. However, there have been no reports examining non–bone-injury cervical spinal cord injuries associated with cDISH. Therefore, we investigated not only patients with cDISH fractures but also SCI without fractures and compared them with the general elderly population. The purpose of the current study was to provide an overview of the characteristics and clinical course of elderly patients with cDISH-related injuries compared with a matched cohort of patients with non–cDISH-related injuries. The analyses were performed on groups of patients with and without fractures, respectively.
Methods
Patient Population
The current multicenter study was based on a retrospective database of patients aged 65 years or older hospitalized for cervical spinal cord and/or cervical spine injuries between 2010 and 2020, conducted by the Japan Association of Spine Surgeons with Ambition (JASA) group. 10 Thirty-three medical institutions participated in data collection. The study was approved by the Institutional Review Board (No. 3352-1) and each of the 25 representative institutions. Because this was a retrospective study, informed consent was not required for submission. The optout of this study was posted on a website (https://web.sapmed.ac.jp/orsurg/guide/hj0g2h00000007ax-att/pgsps60000000g3l.pdf), and we did not receive any inquiries.
A total of 1512 patients were entered into the database, and 149 patients with cDISH were identified. Excluding 9 of these patients, 140 cDISH-related injuries were included in the analysis; 106 cDISH-related injuries with fracture and 34 injuries without fracture were identified. Propensity score–matched cohorts from 1363 patients without cDISH for each control were generated and compared (Figure 1). Because of the relatively small number of patients with cDISH-related injury without fracture, corresponding controls were selected following a 1:2 ratio. In addition to these, logistic regression analysis was performed to determine the risk of early mortality for patients with cDISH-related injury. Flowchart of patient inclusion.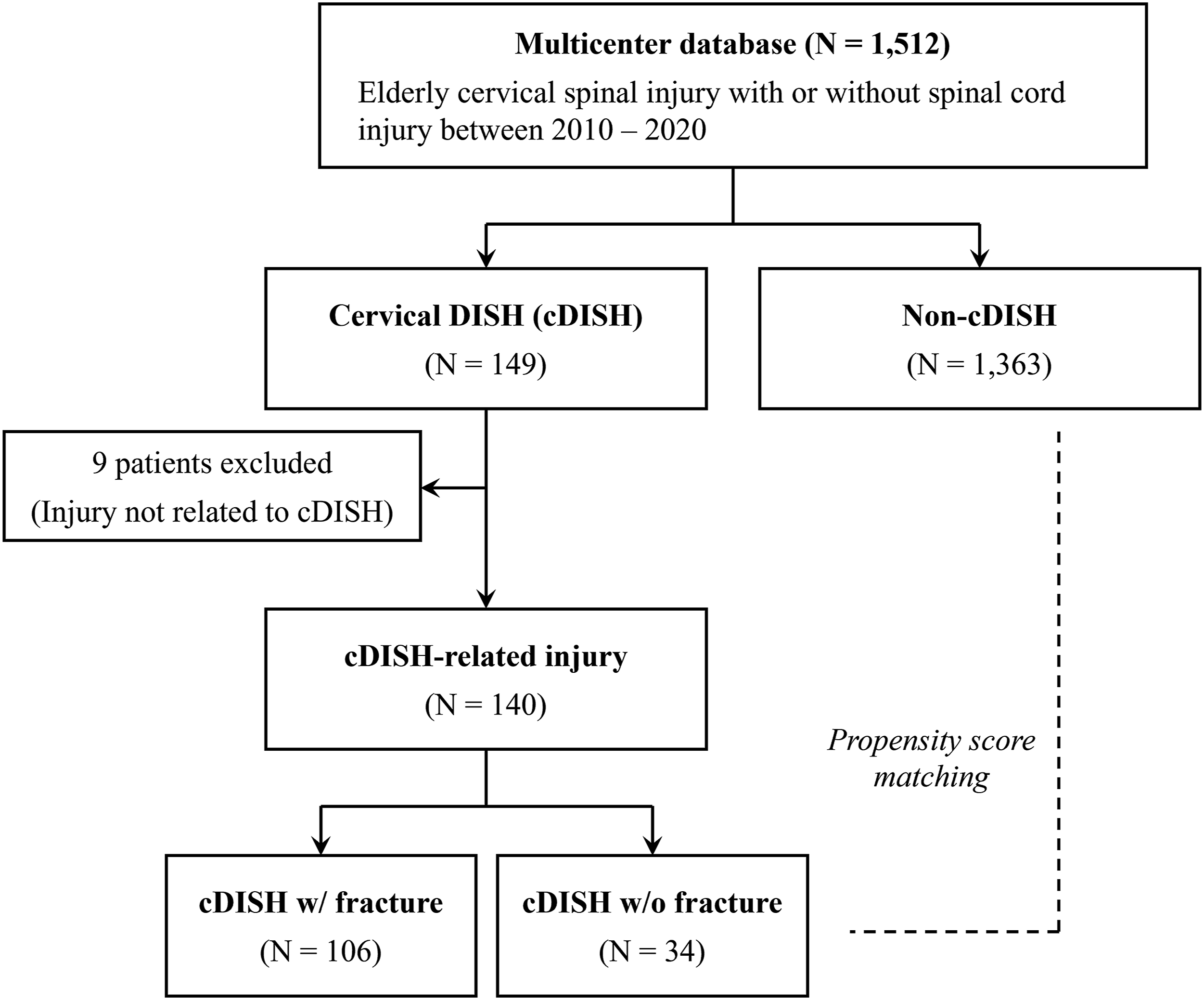
Cervical Diffuse Idiopathic Skeletal Hyperostosis
DISH was diagnosed as the presence of calcification or ossification in at least 4 consecutive vertebrae on computed tomography (CT) images, relatively preserved disc space in the affected region, and no findings suggestive of disc degeneration such as osteosclerosis of the vertebral margins. cDISH was defined as the presence of DISH involving the cervical level. Therefore, patients with DISH in the thoracolumbar spine but with no fused vertebrae in the cervical spine were excluded from the group of cDISH patients.
cDISH-Related Injury
We defined a cDISH-related injury as a fracture in the fused segment due to cDISH and an SCI between the cDISH segment and the next level. Fractures were identified by CT or magnetic resonance imaging (MRI). The SCI level was confirmed by MRI. Fractures occurred in segments that were fused due to DISH. Nine patients with cDISH whose injury levels were distant from cDISH were excluded, as previously described. This population included 1 Hangman fracture, 1 Anderson type III odontoid fracture, and 7 cervical spinal cord injuries without fractures, all more than 1 level away from cDISH.
Patient Demographic and Operative Data
Age, sex, comorbidities, ambulation before injury, cause of injury, presence of OPLL/fracture/dislocation/motor paralysis, and ASIA Impairment Scale (AIS) were recorded, and the 5-Item modified Frailty Index (mFI-5) was determined. In addition, we recorded whether surgery was performed, the surgical procedure, perioperative and postoperative complications during hospitalization, and ambulatory ability at discharge and 6 months later as well as AIS score 6 months later.
Statistical Analysis
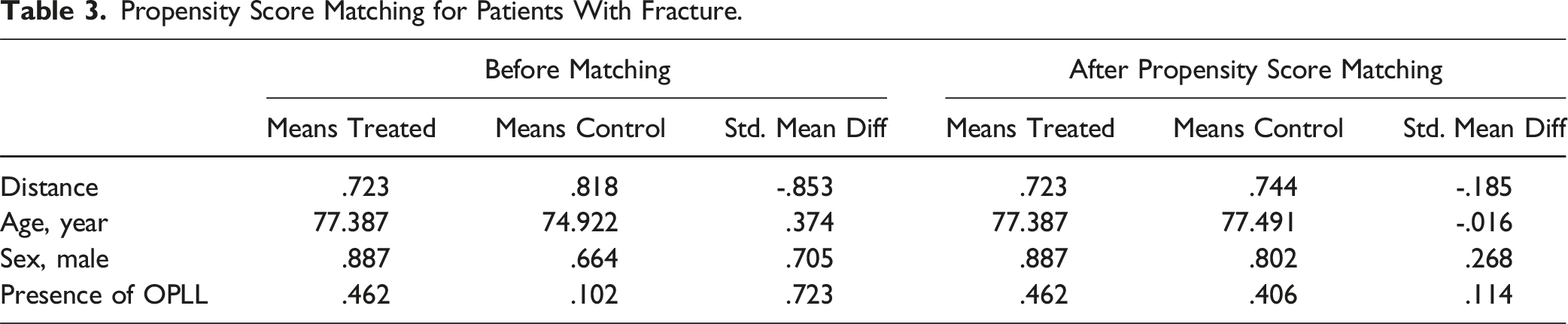
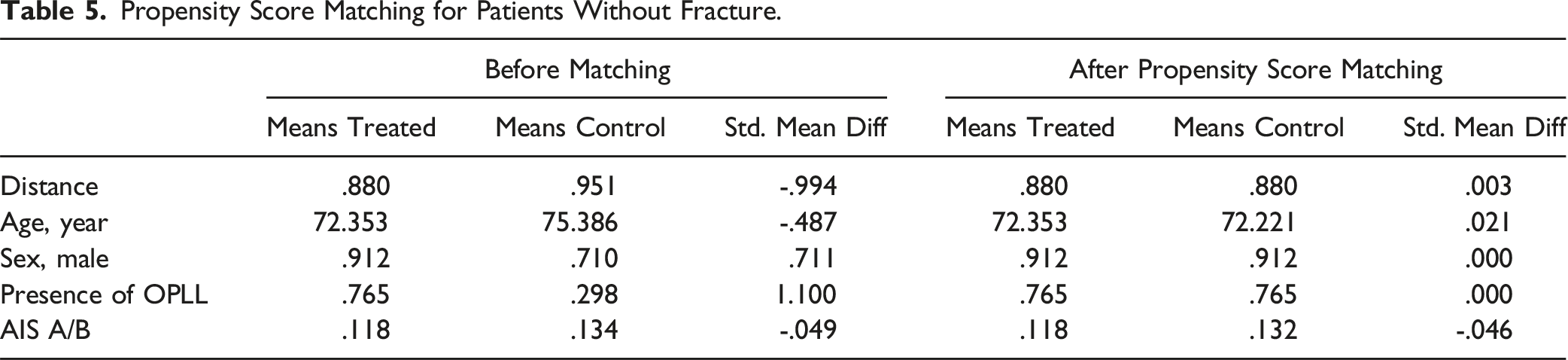
Data are presented as means ± standard deviations for continuous variables and as number and percentage for categorical data. We performed statistical analyses using R version 4.2.1 (http://www.R-project.org) on Wilcoxon rank-sum test, Fisher exact test, and Pearson chi-squared test. A P value <.05 was considered a significant difference. We performed propensity score matching using the MatchIt package (https://cran.r-project.org/web/packages/MatchIt). The following items were selected to adjust for patient background: age, sex, and presence of OPLL. Patients with upper cervical fractures were excluded from the control group because there were no patients with upper cervical fractures in patients with cDISH-related injuries with fractures. Paralysis severity (complete paralysis or not) was added to the adjusting items for the group with cDISH-related injury without fracture.
Results
Patient Demographics.
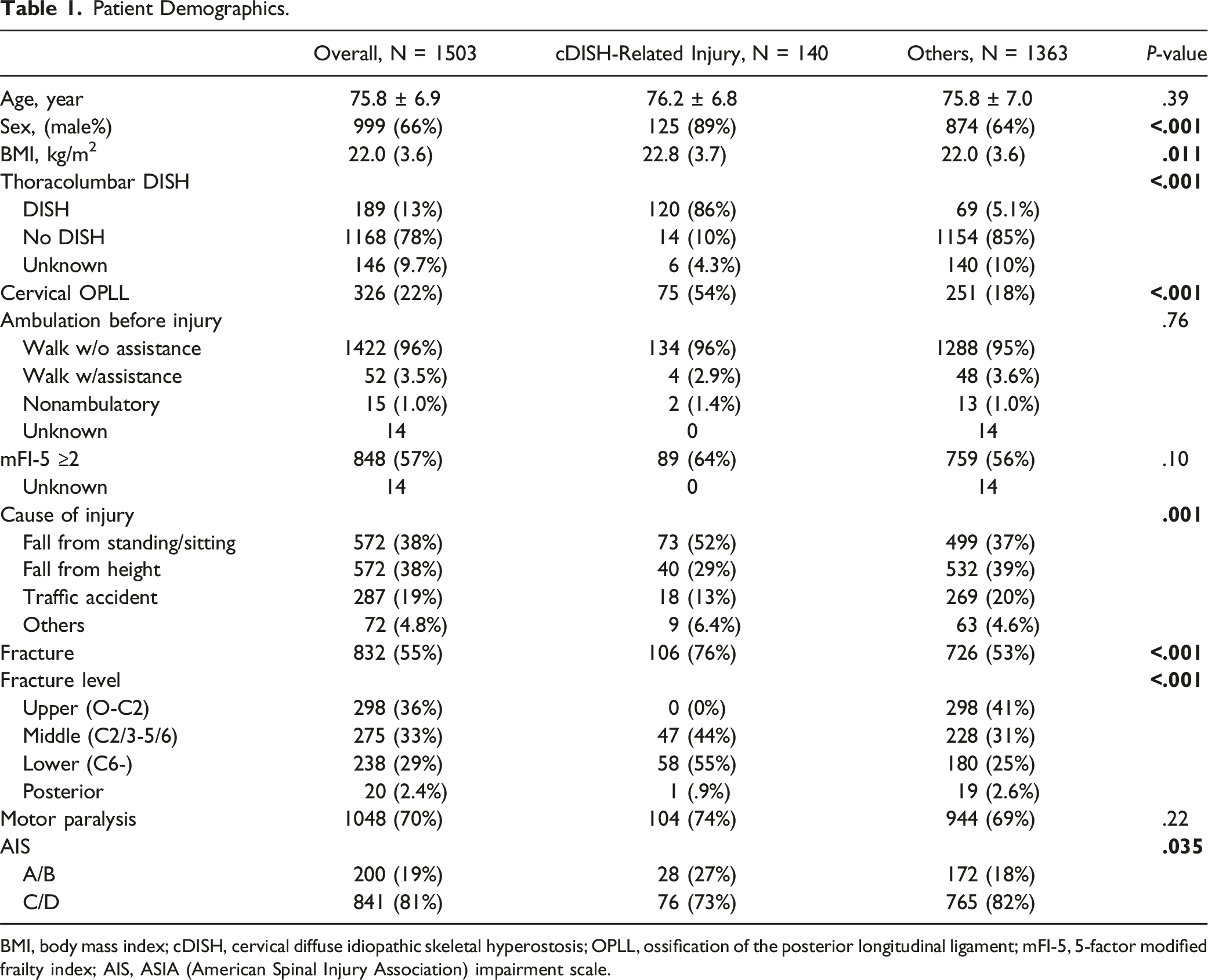
BMI, body mass index; cDISH, cervical diffuse idiopathic skeletal hyperostosis; OPLL, ossification of the posterior longitudinal ligament; mFI-5, 5-factor modified frailty index; AIS, ASIA (American Spinal Injury Association) impairment scale.
cDISH Range.

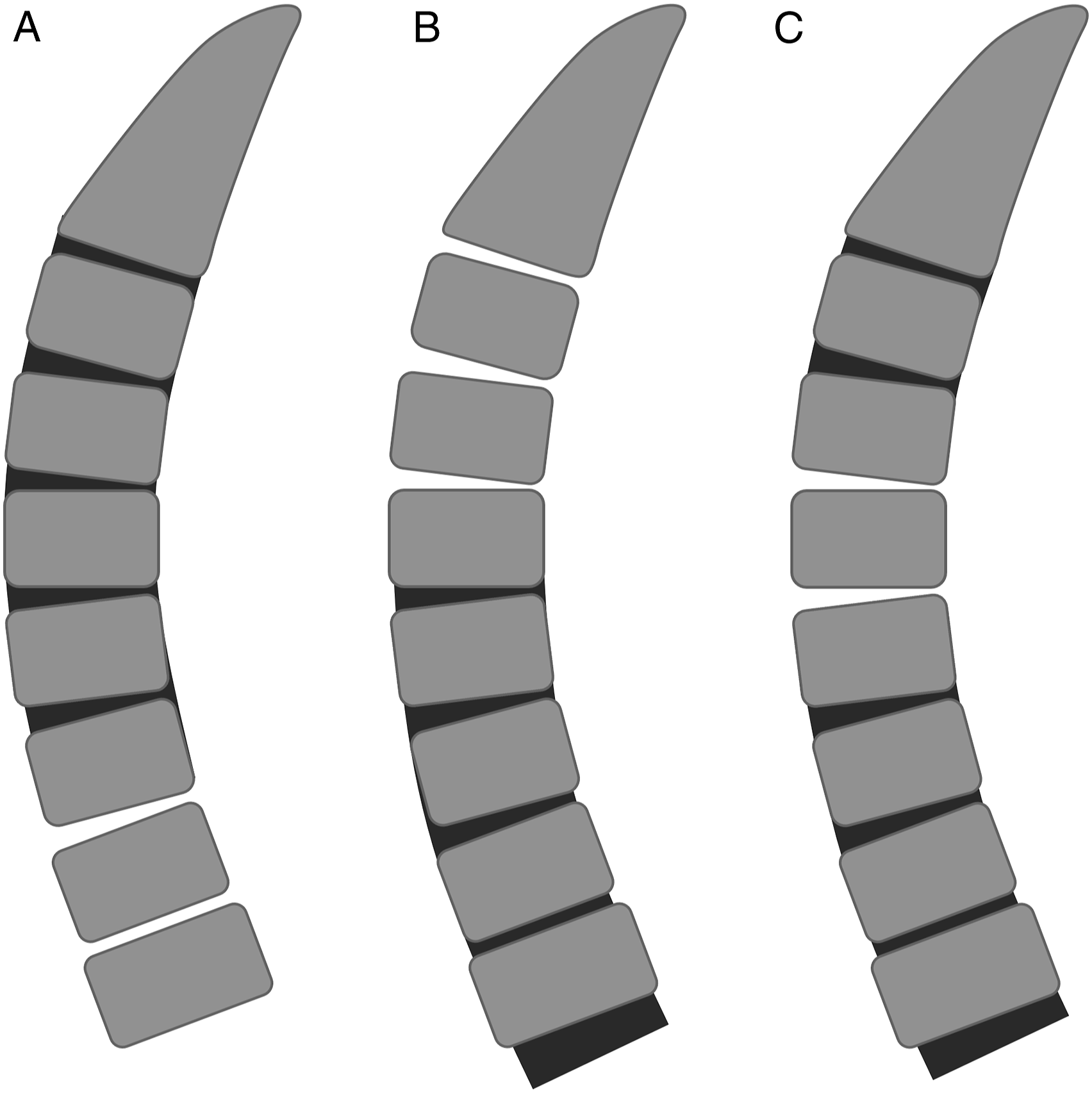
cDISH range. (A) cervical; (B) cervicothoracic; (C) others.
cDISH-Related Injury With Fracture
Propensity Score Matching for Patients With Fracture.
Matched Cohort Analysis for Patients With Fracture.
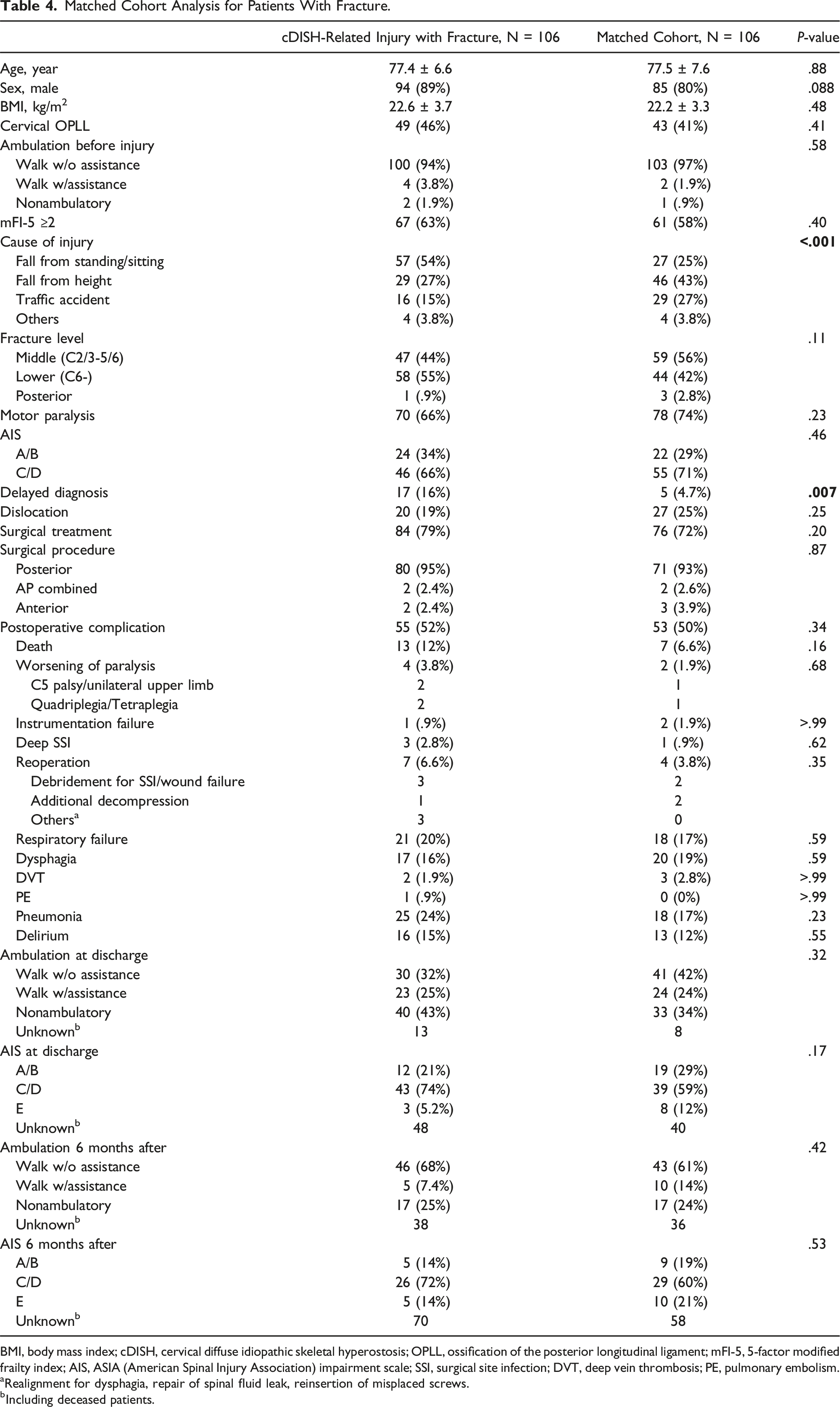
BMI, body mass index; cDISH, cervical diffuse idiopathic skeletal hyperostosis; OPLL, ossification of the posterior longitudinal ligament; mFI-5, 5-factor modified frailty index; AIS, ASIA (American Spinal Injury Association) impairment scale; SSI, surgical site infection; DVT, deep vein thrombosis; PE, pulmonary embolism.
aRealignment for dysphagia, repair of spinal fluid leak, reinsertion of misplaced screws.
bIncluding deceased patients.
cDISH-Related Injury Without Fracture
Propensity Score Matching for Patients Without Fracture.
Matched Cohort Analysis for Patients Without Fracture.
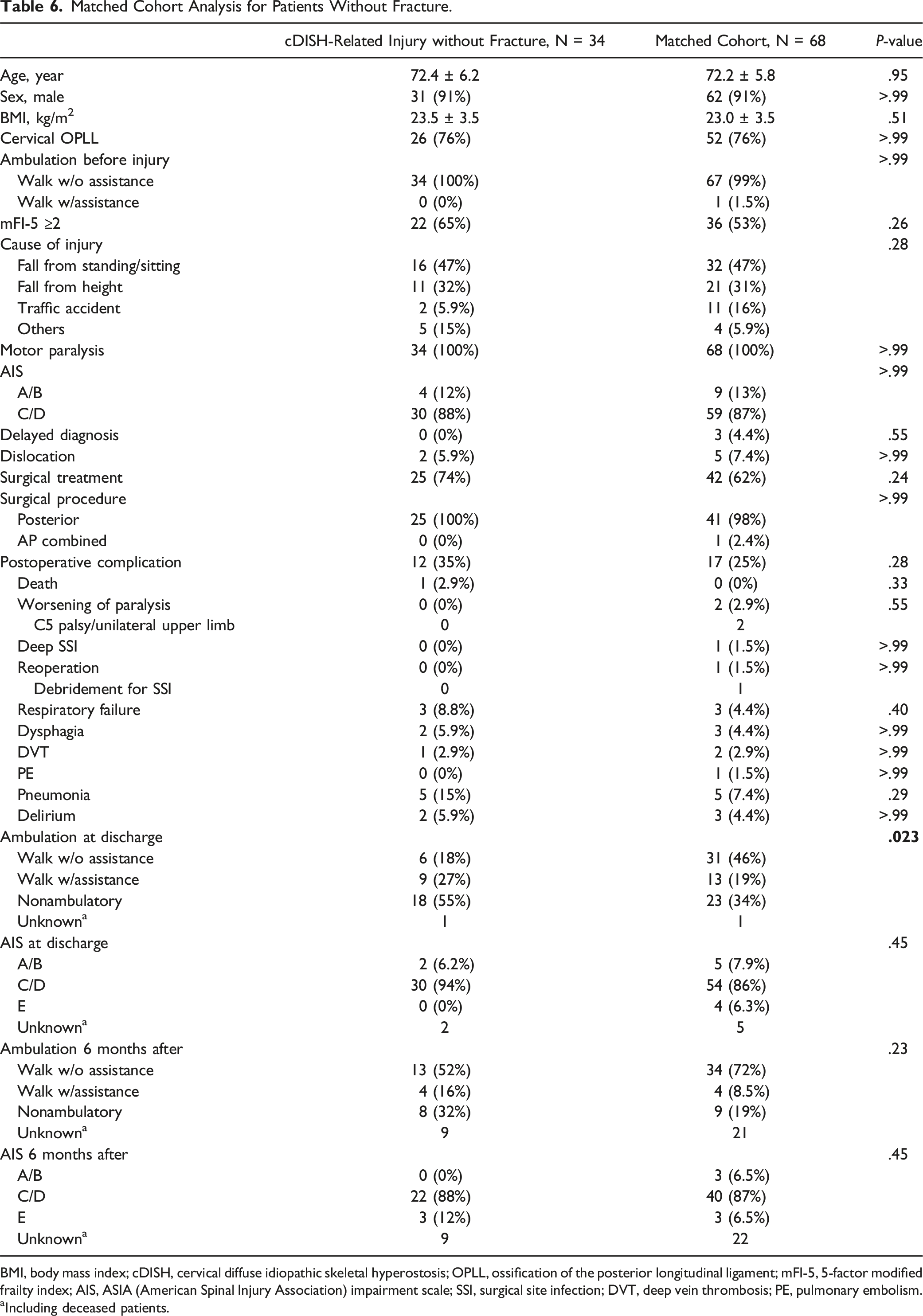
BMI, body mass index; cDISH, cervical diffuse idiopathic skeletal hyperostosis; OPLL, ossification of the posterior longitudinal ligament; mFI-5, 5-factor modified frailty index; AIS, ASIA (American Spinal Injury Association) impairment scale; SSI, surgical site infection; DVT, deep vein thrombosis; PE, pulmonary embolism.
aIncluding deceased patients.
Univariate Analysis for Mortality of cDISH-Related Injury.
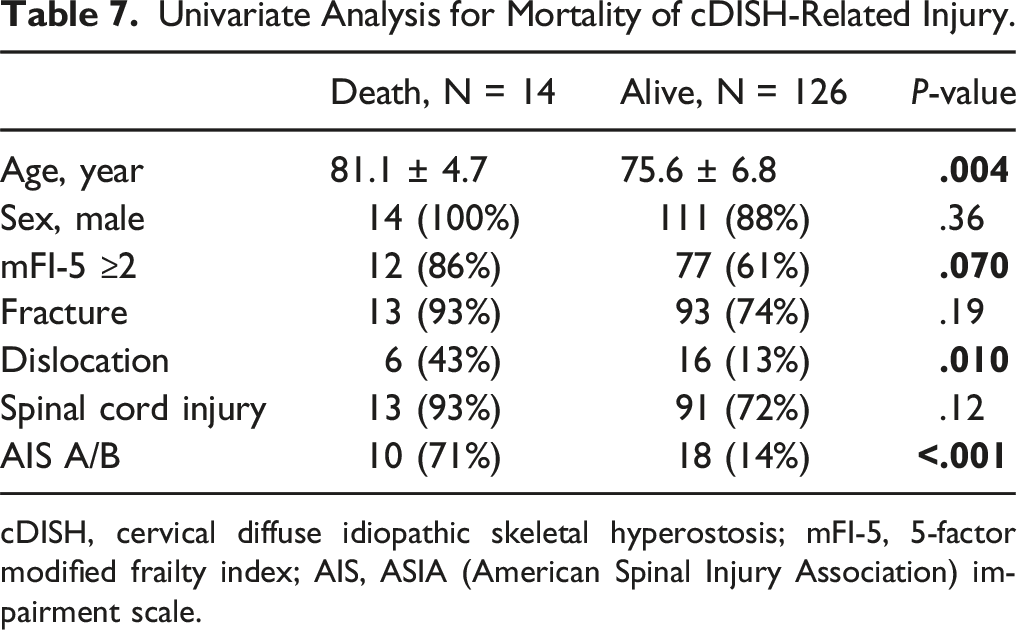
cDISH, cervical diffuse idiopathic skeletal hyperostosis; mFI-5, 5-factor modified frailty index; AIS, ASIA (American Spinal Injury Association) impairment scale.
Multivariate Analysis for Mortality of cDISH-Related Injury.
Discussion
This study is the largest-scale retrospective study of elderly patients with cDISH. We analyzed a total of 140 patients with cDISH-related injuries, focusing not only on 106 fractures but also on 34 SCI without fracture. In contrast to previous reports, we found that elderly patients with cDISH-related injury with fractures did not differ significantly from matched controls in the incidence of complications, ambulatory outcomes, or severity of paralysis. Furthermore, patients with cDISH-related injuries without fractures mainly had incomplete motor paraplegia, and although the incidence of complications was not significantly different compared with the controls, these patients had significantly worse ambulation at discharge than the matched controls did.
We used a large database not only to analyze the largest ever group of elderly cDISH patients but also to compare the results with those of a well-matched group of subjects selected by matching from a concurrently collected group of elderly patients with cervical spine and cervical SCI. Westerveld et al 4 compared patients with DISH (40 patients) and AS (14 patients) injury to 111 other patients. They found that patients with DISH or AS had significantly higher complication and mortality rates. However, the study had weaknesses in that the patient population was diverse, including thoracolumbar as well as cervical spine injuries, and the controls were not matched. Schoenfeld et al 11 also compared patients with DISH (27 patients) and AS (16 patients) with matched controls. They found no significant difference in the risk of mortality between the DISH group and the controls, but their sample size was limited. Therefore, when limited to elderly patients with cervical spine injuries, the prognostic impact of the presence or absence of DISH is unknown.
In the present study, there were no statistically significant differences in neurologic or life outcomes of elderly patients with cDISH-related injuries as compared with patients without cDISH. Originally, the elderly patients were more frail,12–14 and recovery in the group of elderly patients with SCI was poor and mortality was high compared with younger patients.15,16 Therefore, when it comes to cervical spinal cord injuries in older adults, the influence of the presence or absence of DISH on the fate of patients may be limited. It should be noted, however, that the mortality rate of patients with cDISH-related injury with fracture was almost double that of controls. Furthermore, DISH not only leads to osteoporosis, but also increases the risk of falls due to impaired trunk flexibility and compromised balance. In the present database, patients with cDISH suffered the same degree of spinal injury as the group of patients without DISH from a minor fall. DISH is a systemic disease and is associated with abnormal conditions such as metabolic syndrome, 17 which adversely affects life expectancy. We cannot rule out the possibility that the still insufficient number of patients in the present study might have led to erroneous statistical determinations; cDISH fractures may remain a potential factor in worsening life outcome. 8
Next, we focused our attention not only on fractures but also on SCI without fractures. SCI without fracture is common in patients with preexisting conditions such as cervical spondylosis, OPLL, and canal stenosis (ie, older adults) when they experience minor trauma without bone damage.18,19 Most cDISH-related injuries without fracture occurred at the margin of the cDISH. Most patients had incomplete motor paralysis, and there was no significant difference in complication rates compared with matched controls. On the other hand, interestingly, patients with cDISH-related SCI without fracture had significantly poorer ambulatory ability at discharge (the short-term outcome) compared with controls; however, neurologic outcomes at 6 months were not significantly different between the groups. Because ankylosing spine negatively affects trunk stability and balance, 20 patients with DISH have poor activity. This might have led to differences in the results of short-term rehabilitation.
Patients with cDISH-related injury with fracture are often overlooked, leading to the subsequent occurrence of paralysis or more severe paralysis.4,21–23 We found that the increased risk of mortality in patients with cDISH-related injuries was influenced by older age and the occurrence of complete paralysis. Therefore, to reduce the risk of mortality, the delay in diagnosis must be reduced. Our results showed a significantly higher diagnostic delay (16%) in patients with cDISH-related injuries compared with the control group. However, the total mortality rate was 10%, which is comparable or lower than in previous reports, 21 considering that the mean age of the patient population in previous reports was younger than that in the current study. Although recent improvements in the knowledge of DISH might have reduced diagnostic delays and indirectly contributed to the lower mortality rate, the reduction is insufficient. Therefore, there is a need for continued efforts to educate health care providers about the diagnostic difficulties of this injury.
The current study had several limitations. First, the retrospective nature of this research might have led to selection bias. Second, although cDISH was determined by skilled spine surgeons based on imaging findings, it is not clear whether the ossification extends to the posterior elements and is a complete fusion or only ossification of the anterior longitudinal ligament. Therefore, it is unclear whether the results of the present study represented cDISH as an ankylosed spine, and future analysis based on the severity of ossification of DISH is needed. Third, the findings regarding the sacroiliac joint used for a rigorous DISH diagnosis were not confirmed in all cases. However, because the number of AS patients in Japan is small, it can be assumed that the present data set consists of DISH patients. Thus, this study included data from a wide area and allowed for the evaluation of outcomes in elderly patients with cDISH.
Conclusion
In this study, which is the largest retrospective study of elderly patients with cDISH-related injuries, there were no significant differences in the incidence of complications, ambulation outcomes, or severity of paralysis in patients with cDISH-related injury with fracture as compared with matched controls, and although most patients with cDISH-related injury without fractures had incomplete paralysis, their ambulation outcomes at discharge were significantly inferior to those of the matched control group.
Footnotes
Acknowledgments
We thank all members of the Japan Association of Spine Surgeons with Ambition (JASA) for collecting the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Thirty-three health care facilities were included in the database. The study protocol was approved by the Institutional Review Board (no. 3352-1) of each of the 25 representative institutions.