
Abstract
Introduction
Stability and soft tissue balance are crucial in producing a positive outcome for total knee arthroplasty (TKA). 1 –3 Of the causes for revision TKA, instability is responsible for up to 18.7% of cases. 4 In order for surgical intervention to achieve balance and stability, we need to understand the starting point of the soft tissue envelope of the knee so that TKA can successfully preserve or correct this envelope.
Published values for the medial and lateral laxity of healthy knees have been documented in various age groups and positions including maximum knee extension and 20°, 70°, 80°, and 90° of knee flexion. The study cohorts have ranged between 20 and 62 subjects. 5 –9 These studies measure medial and lateral displacement from the individual resting position of the knee. In the healthy population the hip-knee-ankle-angle (HKAA) varies between −8° (varus) and +5° (valgus) and it is displacement from these varied starting positions that has been used to establish the medial and lateral laxity of the healthy knee. 10 In the healthy population, the weight-bearing axis of the lower limb passes through the center or near center of the knee. 11 In this position, the femoral and tibial mechanical axes will achieve an HKAA of 0° when the center of the tibia and femur match at the knee and the bone, and soft tissue structures allow the axes to become colinear. More typically, however, as documented by Bellemans et al., 10 the lower limb axes (limb, femoral, and tibial mechanical) will be near colinear due to bone and/or soft tissue restriction and the HKAA will approach, but not necessarily equal, 0°. We can reproduce this circumstance in the osteoarthritic (OA) knee by manipulating the weight-bearing axis of the lower limb to pass through the center of the knee. Similarly, the HKAA in this position will not necessarily be 0°.
The medial and lateral laxity of the varus OA knee and symptomatic OA knees (without definition of varus or valgus alignment) has been previously documented in the literature in varied degrees of knee flexion in study cohorts of 20, 35, and 72 subjects. 8,12,13 The medial and lateral laxity of the valgus OA knee has been described subjectively. 14,15 To our knowledge, no study has objectively documented medial and lateral laxity parameters for the valgus OA knee.
The coronal plane laxity of the valgus OA knee has been described by The Société d’Orthopédie de l’Ouest (Western France Orthopedics Society—SOO) group in 2003 and by Ranawat et al. 14,15 These grading systems focus on whether the coronal plane tissue in extension is either contracted or normal laterally and the combination of this with normal or abnormally lax medial tissues. These are subjective grading systems that lack defined objective measures for the degree of coronal plane laxity found within each of their subgroups.
The primary aim of this study is to use computer navigation, immediately prior to TKA, to place the weight-bearing axis of the lower limb through the center of the knee, and to measure medial and lateral laxity of the valgus OA knee as maximal displacement from this point in maximum extension, 20° and 90° of knee flexion.
Material and methods
Thirty subjects undergoing unilateral computer-assisted surgery (CAS) TKA were included in the study. Inclusion criteria were patients with valgus, degenerative OA of any degree scheduled for primary TKA. Patients were excluded if they had undergone previous ligament reconstruction surgery, knee osteotomy, suffered other trauma likely to distort the periarticular soft tissues including extra-articular deformities, and patients who declined consent or where intraoperative placement of navigation pins were considered high risk due to poor bone stock or soft tissue integrity. Ethical approval was obtained from the relevant institutional review board, and written informed consent was obtained preoperatively for all subjects.
The measurement technique has been previously described for measurement of coronal laxity in the varus knee. 12 A medial para-patellar approach to the knee was undertaken. Femoral and tibial navigation pins were inserted. All landmarks were identified and registered in the navigation system for calculation of the mechanical axes of the femur, tibia, and lower limb and generation of an individualized 3-D model of the patient’s anatomy using computer navigation software (BrainLab, Munich, Germany). The status of the anterior cruciate ligament and posterior cruciate ligament was recorded. Osteophytes were left in situ to assess the knee as close to its pathological OA state as possible. The anterior horn of the medial meniscus was left intact. Given the valgus alignment of the subject’s knees, release of the deep band of the medial collateral ligament was not required to attain accurate navigation registration.
The patella was reduced, and the degree of fixed flexion deformity or hyperextension was recorded in maximum knee extension. The mechanical axis of the limb was corrected to the center of the knee by observing CAS displays. The femoral and tibial mechanical axes were manipulated to be as colinear as possible to the limb axis at this position. Figure 1 demonstrates the principles of the technique and why the neutral position for each knee may not equate exactly to 0°.
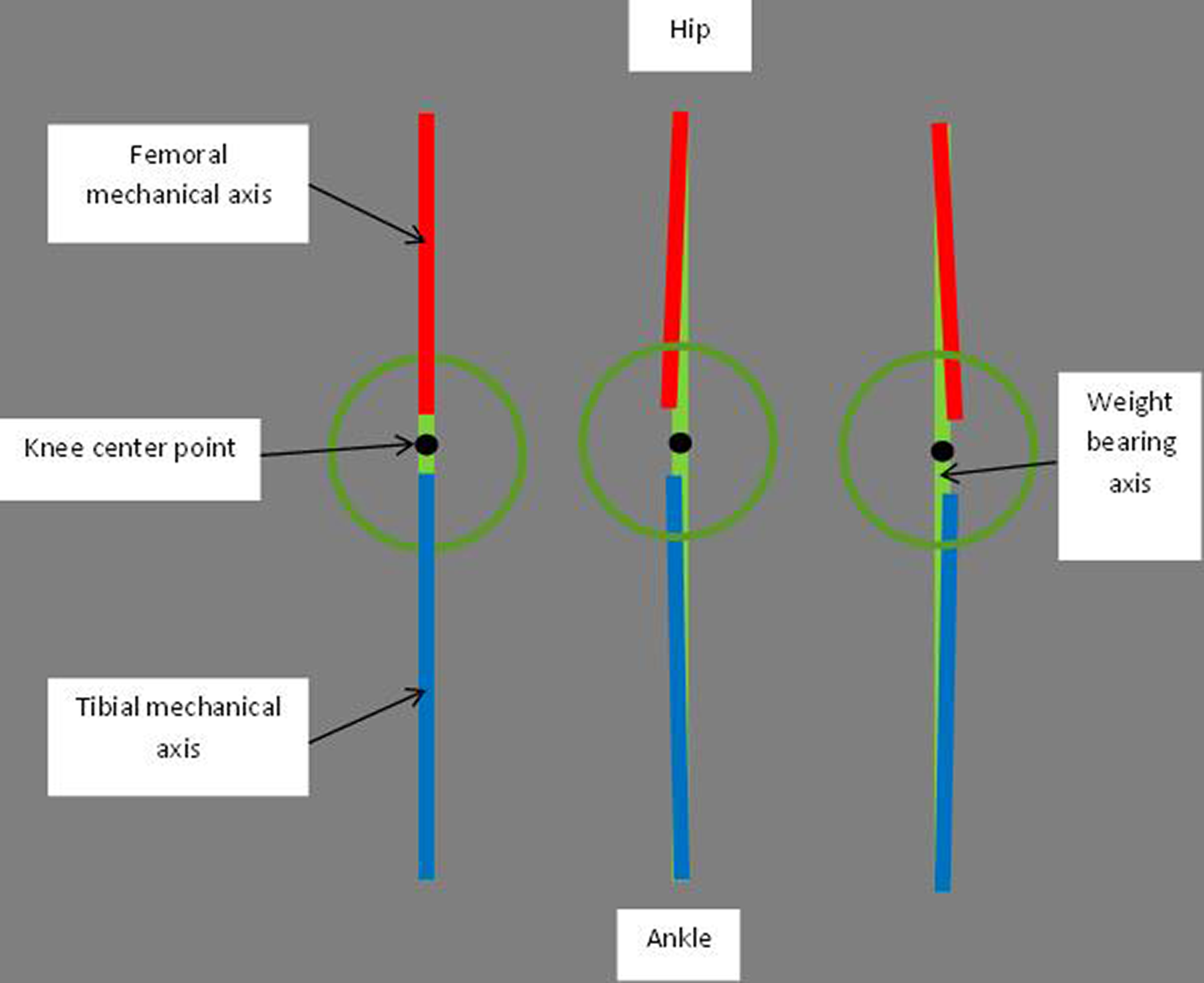
Demonstration of how an HKAA of 0° will be achieved when the femoral and tibial mechanical axes match at the knee center while the weight-bearing axis of the lower limb passes through the knee center as well. A more typical situation in the healthy population is a slight mismatch in the femoral and tibial axes at the knee center; the axes will not be parallel when the limb weight-bearing axis passes through the center of the knee meaning the HKAA will approach, but not be 0°. HKAA: hip-knee-ankle-angle.
These methods produced a limb position acting to define a neutral, corrected alignment for each knee consistent with prior literature. 10,11 The HKAA was recorded at this point. The knee was moved through a medial–lateral arc via manual force from this corrected position. Measurements were defined by medial and lateral deviation from the corrected axis point, in degrees, as indicated by the navigation software. Direct observation of the joint was undertaken during measurements to prevent subluxation and ensure congruency in all planes (Figure 2). These measurements were undertaken in maximal knee extension and 20° of knee flexion. The point of maximum valgus deformity or the “loaded HKAA” was recorded.

Demonstration of the correction of the mechanical axis to an individualized neutral point for each knee. (Medial and lateral laxity was measured in maximum extension and 20° flexion as deviation from this point.)
In 90° of knee flexion, neutral rotation and colinearity of the femoral, tibial, and limb axes were attained via CAS displays with observation of the joint again used to ensure congruency. Laxity was measured as medial and lateral displacement, in degrees, from this neutral point via the weight of the limb and manual force consistent with prior techniques (Figure 3). 7,9,12

Demonstration of correction of the limb axes in 90° flexion. (Medial and lateral laxity was measured as deviation from this point).
Modern navigation systems have been validated for these measurements. 13 Measurements were defined to allow for matching to prior subjective descriptions. An irreducible coronal plane lateral contracture was considered present when the weight-bearing axis of the lower limb could not be manipulated to pass through the knee center. As these knees could not attain a “zero” point, medial and lateral laxity values could not be definitively defined for these subjects. A reducible coronal plane lateral contracture was considered present when the weight-bearing axis of the lower limb could be manipulated to pass through the knee center. However, further displacement of the lateral tissues allowing movement beyond this point within previously documented physiological ranges for elderly controls was not present. 5 In these circumstances, lateral laxity was recorded as zero. Medial laxity was considered abnormal when it exceeded 7°. 5 –7 Once the data was recorded, a CAS TKA was performed. In all cases, the procedure and measurements were performed by a single, high volume arthroplasty surgeon (MJM) at a single center. All data were prepared and analyzed using Prism 5 for Mac OS X Version 5 (GraphPad Software Inc. La Jolla, California, USA). Statistical comparisons were made using one-way analysis of variance with Tukey’s multiple comparison tests.
Results
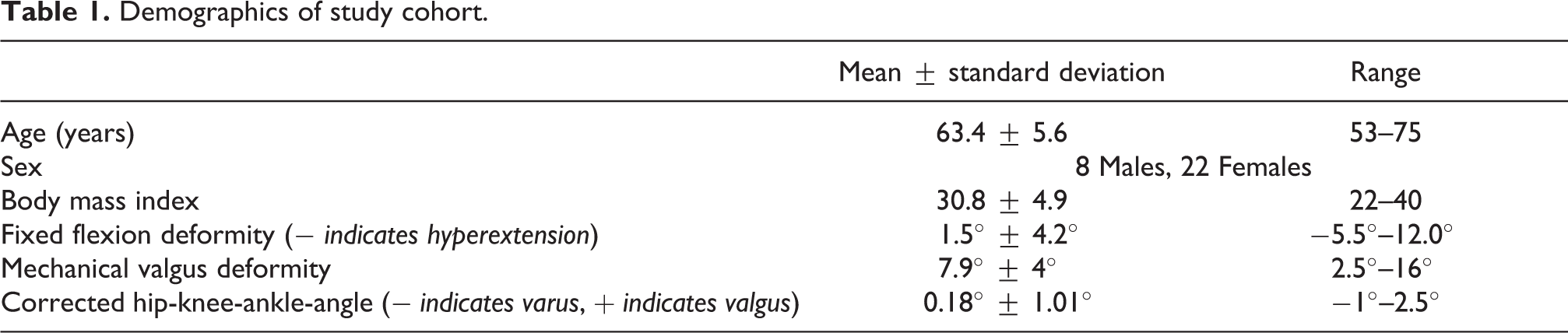
Thirty patients contributed 30 TKA’s to the study. Table 1 illustrates the demographics of the study population.
Demographics of study cohort.
In maximum extension, individual medial and lateral coronal laxity values were able to be recorded in 27 patients. In three subjects, the mechanical axis of the limb could not be manipulated to pass through the center of the knee. Therefore, no neutral point was attained and thus no medial and lateral laxity values were recorded. These subjects were important to the study as being representative of irreducible laterally contracted tissue. They were all female and had valgus deformities of 8.5°, 16°, and 16°.
In 20° of knee flexion, individual medial and lateral coronal laxity values were able to be recorded in 29 patients. In one subject, the mechanical axis of the limb could not be manipulated to pass through the center of the knee. This subject was a female with 16° of valgus deformity who also had an irreducible lateral contracture in maximum knee extension.
In 90° of flexion, individual medial and lateral coronal laxity values were recorded in all 30 subjects.
On the medial side, there was a statistically significant (p < 0.0001) decrease in mean laxity when comparing maximum knee extension and 90° of knee flexion (Table 2). The opposite finding was present on the lateral side where there was a statistically significant (p < 0.0001) increase in mean laxity when comparing maximum knee extension and 90° of knee flexion. In the 27 knees that had individual laxity measurements at full knee extension, we examined the difference in medial laxity at maximum extension versus 90° of knee flexion and found a mean difference of 3.96 ± 3.3°. For the same measurement, on the lateral sided, there was a mean difference of 5.53 ± 3.13°.
Medial and Lateral Laxity Measurement in degrees of displacement (mean ± SD) from each neutral test position.

Six different coronal laxity findings were demonstrated in maximum extension. Laxity values were referenced against previous medial and lateral coronal plane laxity values published for healthy subjects.
Type 1: Normal subjects
Fifty percentage (15/30) of subjects had medial and lateral laxity measures within limits previously recorded for healthy subjects. Within this subject group, mean medial laxity was 4.4° (range 1–7°), mean lateral laxity was 3.4° (range 1–8°), and the mean mechanical valgus deformity was 4.9° (2.5–7.5°).
Type 2: Lateral contracture
An irreducible or reducible lateral contracture was present in 26.6% (8/30) of subjects and, with the exception of one subject, contracture corresponded to the presence of abnormal medial tissue laxity. 10% (3/30) of subjects had an irreducible lateral contracture. Valgus deformity in these subjects was 8.5°, 16°, and 16°. 13.3% (4/30) of subjects had a reducible lateral contracture. These subjects had abnormally lax medial tissue laxity with measures of 9°, 11°, 15°, and 15° with valgus deformities of 8°, 11°, 15°, and 15.5°. 3.3% (1/30) of subjects had a reducible lateral contracture and medial coronal tissue laxity of 7° which is at the upper limit of healthy parameters.
Type 3: Medial laxity without lateral contracture
20% (6/30) of subjects had lateral laxity measures within limits previously recorded for healthy subjects and abnormally lax medial tissue. For this group, medial laxity was 8°, 8.5°, 9°, 10°, 11°, and 11.5°. Lateral laxity was 1°, 1°, 1.5°, 2°, 2°, and 3.5°. Valgus deformity was 7.5°, 7.5°, 9.5°, 10.5°, 10.5°, and 11°. 3.3% (1/30) of subjects had both abnormally lax medial and lateral tissue. This subject had medial tissue laxity of 12.5° and lateral tissue laxity of 10°. They had a valgus deformity of 13.5°.
In total, abnormally lax medial tissue was present in 46.6% (14/30; type 2A and B; type 3A and B) of subjects.
In summary, a valgus deformity of ≥8° was associated with abnormal medial laxity in extension. However, a lateral contracture was only present in 50% of subjects with valgus deformity of ≥8°.
Discussion
The coronal plane laxity of the healthy and varus OA knee has been previously described in the literature. 5 –13 Hohman et al. documented the total coronal arcs of motion in 45 valgus knees in 10° of knee flexion. They used computer navigation as a measurement tool and examined the association between valgus deformity and corresponding radiological parameters. They did not specifically isolate medial or lateral laxity values. 16
We are, to our knowledge, the first to provide objective measures for the medial and lateral coronal plane laxity of the valgus OA knee. This was undertaken in varying positions: maximum extension, 20° and 90° of knee flexion. These objective measures provide insight into the differing laxity patterns of valgus OA knees requiring TKA. They highlight the potentially complex surgical planning issues for TKA in the valgus knee, particularly regarding the soft tissue envelope and that the valgus OA knee is not a homogenous entity. Further to this, our results allow comparable assessment to previously described subjective grading systems for the valgus OA knee. 14,15
Before considering our results in detail, it is important to understand our reasoning for the “zero” points from which measurement was undertaken. The reference point used to measure medial and lateral laxity from is achieved when the weight-bearing axis of the lower limb passes through the center of the knee while the femoral mechanical axis and the tibial mechanical axis are aligned as close to colinear as possible. Due to individual soft tissue and bone anatomy variation, when the weight-bearing axis remains passing through the center of the knee, small deviations from an HKAA of 0° are evident. This variation is shared by previous studies and in fact only a small percentage of healthy knees have an HKAA of exactly 0°. 10,13,16 This position is also relevant to TKA as mechanical alignment theory aims to have the weight-bearing axis of the limb through the center of the knee and the femoral and tibial mechanical axes colinear within a deviation of 3°.
While an HKAA of 0° does provide a standardized reference point from which to measure medial and lateral laxity, it is not typical of the healthy knee. Our HKAA “zero” points, or the points at which we measured our medial and lateral laxity from, ranged from −1 (varus) to 2.5 (valgus). This is a small yet fundamentally important difference compared to simply utilizing an HKAA of 0° as the origin of laxity measurement. The reason for this is the medial and lateral laxity found in the healthy knee has been reported as 2.3 ± 0.9 and 2.8 ± 1.3°, respectively. 5 Therefore, the small differences in the starting points for each of our individual subject’s laxity measurements will significantly affect comparison of the measured medial and lateral laxities to those documented for healthy subjects. By utilizing the method described, we have produced a circumstance that is both individual to each knee and more closely resembling the healthy knee. 10,11
Our findings highlight the complexities of the soft tissue envelope around the valgus knee. Valgus deformity of ≥8° is associated with abnormal laxity of the medial soft tissues but only 50% of subjects with this level of deformity will also display a lateral contracture. We have demonstrated statistically significant differences when comparing values for the mean medial and lateral laxity in varying degrees of knee flexion and also for mean laxity measured in maximum knee extension versus 90° of flexion on both the medial and lateral sides of the knee. The mediolateral and flexion–extension variation makes overall knee balancing potentially difficult. These results mean it is vital to undertake careful examination of each knee prior to and during the initial phases of surgery to assess individual laxity patterns and prepare for challenges in soft tissue balancing during TKA.
These findings are directly applicable to TKA. Surgical release of soft tissues to achieve a balanced knee should focus on tissues that predominantly effect knee extension and any release of soft tissue structures that may heighten the relative laxity of the lateral side of the knee in flexion should be approached with caution. 17 Bone resections that place the knee in a small degree of valgus will help the laxity differential between the lateral and medial sides seen in extension but may heighten lateral flexion laxity. Maximizing the external rotation of the prosthesis will help diminish the effect of any lateral flexion laxity that is inherent or increased with a valgus resection. The deficient lateral femoral condyle that is often present in the valgus OA knee may also contribute to the laxity imbalances that we have documented. 18 This anatomical characteristic will be addressed by the non-deficient lateral condyle of the TKA prosthesis which will also help diminish lateral flexion laxity. Care should also be taken during balancing to avoid releasing lateral tissue to match abnormally lax medial tissue. The discussion of medial soft tissue reconstructive procedures is very limited in the orthopedic literature. Our results suggest that they may well be important to the overall TKA balancing algorithm given that medial laxity (46.6%) is a more consistent feature than lateral contracture (26.6%) in the valgus OA knee. 19
Previous studies of the varus OA knee have found that the soft tissues are less disturbed in flexion. The soft tissue envelope of the knee becomes more correctible, balanced, and registers laxity values close to those seen in the healthy knee at 90° of flexion. 12,20 If our values measured at 90° of flexion were also indicative of more native tissue tension, then they might serve as a potential primary reference point for acceptable soft tissue tension and balance in the individual valgus knee. Given the lack of specific data around laxity in the healthy and OA valgus knee, this area would require further study.
Roth et al., in a cadaveric study, found mean laxities on the medial side of the healthy knee to be 1.0 ± 0.5° greater in 90° of flexion compared to 0° and on the lateral side, for the same measurement, 2.5 ± 0.8° greater. They discuss in detail the potential difficulties this may pose for gap balancing and its potential to alter soft tissue parameters during arthroplasty relative to the native knee. 21 In our subjects, we found the mean difference between medial laxity at 0° and 90° was 3.96 ± 3.3° and the mean difference between lateral laxity at 0° and 90° was 5.53 ± 3.13°. These even greater differences mean significant surgical alterations in the soft tissue envelope are likely to be required in many valgus knees if a strict gap balancing approach is applied.
Analysis of our objective measurements in maximum extension identified six coronal plane laxity patterns. This allowed for comparison and analysis of the two previous subjective valgus OA knee grading systems which are based on whether the preoperative coronal plane tissue in extension is either contracted or normal laterally and the combination of this with normal or abnormally lax medial tissues. 14,15 Table 3 demonstrates these comparisons. Ranawat et al. described three types of valgus knees. Type 1: minimal valgus and medial soft tissue stretching; type 2: fixed valgus with medial soft tissue stretching; and type 3: post osteotomy. This last type is not relevant to this study as prior surgery was an exclusion criteria in our study, given its potential to alter laxity measurements. The Ranawat system does not allow for normal tissue parameters. The SOO grading is more detailed: type 1: noncontracted lateral tissue and normal medial soft tissue; type 2: irreducible or reducible lateral tissue contracture with normal medial tissues; type 3: reducible contracture with abnormal medial soft tissues; and type 4: irreducible contracture with medial laxity.
Comparison of objective laxity patterns compared to current grading systems.

The abovementioned variability between both grading systems and the six objective patterns of valgus knee laxity in maximum extension found within this study suggests that the grading system for valgus knees is more complicated than previously suggested. Our results have shown a number of important valgus OA knee laxity patterns. It is common to retain normal coronal plane tissue laxity. Irreducible contracture is relatively rare and that most contractures when present are small (reducible but lacking movement beyond neutral). Contracture is almost always associated with medial laxity but medial laxity is often present without lateral contracture. Our objective measures increase the surgeon’s awareness to the potential soft tissues patterns that may in fact be encountered at the time of TKA.
We acknowledge the limitations of our study. The patient group was predominantly Caucasian and their selection for TKA may not be indicative of other surgical series. However, their mean age of 63.4 ± 5.6 is similar to the mean age of patients in the Australian National Joint Replacement Registry of 68.6 years and the mean deformities in Hohman et al., Cooke et al subjects, and ours are also similar measuring 9 ± 4°, 6.44 ± 5.99°, and 7.9 ± 4°, respectively. 11,16,22 Therefore, we believe our results are applicable to the valgus knee population undergoing TKA with deformity up to 16° of mechanical valgus. However, it is also important to appreciate that, given our relatively small study cohort, the distribution of laxity patterns may alter or further laxity patterns may become apparent in larger cohorts. Manual stress testing was performed to assess coronal plane laxity which is typical of in vivo studies. While an experienced surgeon performed this, some degree of variability in the forces exerted during testing is inevitable. Mitigating this is the fact that ligaments are viscoelastic structures, and measurements were recorded at maximal displacement. This should correspond to the plateau of the tension/length curve minimizing any effects of variation in force. 7 Our testing methods were consistent with previously described techniques. 7,9,12,13,16 It is not possible in an in vivo setting to utilize the same invasive techniques with multiple controlled parameters and measurements that are utilized in cadaver studies given the ethical implications of prolonging surgery particularly in relation to infection and fracture risk. Such studies utilize load application systems requiring fixation screws, intramedullary rods, and multiple transections around the knee. 21
Conclusion
We have demonstrated, for the first time, objective values for laxity in the valgus OA knee in multiple positions of knee flexion and maximum extension. We have demonstrated that significant imbalance in both the mediolateral plane and between flexion and extension is present prior to the commencement of TKA. We have documented six distinct patterns of the valgus OA knee based upon lateral and medial laxity combinations in the extended knee. Our work suggests that the laxity patterns are more complex than those previously described subjectively by the SOO and Ranawat grading systems. An awareness of these findings will assist the surgeon during TKA to optimally balance the soft tissue envelope of the knee.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.