
Abstract
This study aims to evaluate the 2-year post-operative clinical outcomes of patients undergoing total knee arthroplasty (TKA) with computer-assisted surgery (CAS) using the pinless BrainLAB® VectorVision® Knee 2.5 Navigation System versus standard CAS. A retrospective case–control study of 200 patients who underwent TKA with CAS from 2008 to 2012 was conducted. Patients in the pinless arm underwent a shorter duration of surgery compared to the standard CAS arm with 72 ± 13 min and 83 ± 11 min, respectively (p < 0.001), with improvement in Oxford Knee Score from 34 ± 8 to 18 ± 5 and 34 ± 9 to 18 ± 5, respectively, without statistically significant differences in clinical outcomes at 2 years.
Introduction
The use of computer-assisted navigation is increasingly favoured by orthopaedic surgeons in total knee arthroplasty (TKA) because of reported advantages in literature including increased precision of individual component placement, 1 correlation with better knee function and quality of life 2 as well as a reduced number of outliers in obtaining neutral mechanical alignment. 3 Initial navigated systems used separate femoral and tibial diaphyseal reference tracker pins which resulted in the occurrence of tracker pin-associated complications 4 in addition to a longer duration of surgery. 5 Pinless navigation systems were thus developed to harness the advantages in mechanical alignment of a computer-navigated TKA while essentially eliminating tracker pin-associated complications. The differences in surgical setup between a pinned versus pinless computer-assisted surgery (CAS) setup in TKA surgery is illustrated in Figures 1 and 2.

Pinned CAS TKR setup. CAS: computer-assisted surgery. Source: Knee Navigation Application. Digital image. BRAINLAB AG. Web 12 June 2016 < https://www.brainlab.com/en/surgery-products/orthopedic-surgery-products/knee-navigation/>.

Pinless CAS TKR setup. CAS: computer-assisted surgery. Source: Knee Navigation Application. Digital image. BRAINLAB AG. Web 12 June 2016 < https://www.brainlab.com/en/surgery-products/orthopedic-surgery-products/knee-navigation/>.
The current literature comparing pinless-navigated TKA with CAS with conventional TKA revealed improved lower limb alignment and placement of components 6 without significant difference in early post-operative function and range of movement, 7 although a longer duration of surgery was required. 8 Although systemic reviews of TKA with CAS assisted by tracker pins have revealed no difference in clinical outcomes when compared to conventional TKA, there is a paucity of data describing the clinical outcomes in patients who underwent TKA with CAS using pinless navigation.
This study aims to evaluate the clinical outcomes of patients who underwent TKA with CAS using a pinless navigation system (BrainLAB® VectorVision® Knee 2.5 Navigation System, Brainlab, Munich, Germany) with a follow-up period of 2 years.
Materials and methods
A retrospective case–control study using clinical data of patients who underwent primary TKA with CAS by a single senior surgeon was conducted for consistency of surgical technique and post-operative care. The study included 100 consecutive patients who received primary TKA with CAS using pinless navigation between November 2008 and October 2012, compared with 100 patients who underwent tracker pin-guided standard CAS in the same period to maintain a 1:1 ratio of case to control. All patients included in the study had severe tricompartmental osteoarthritis demonstrated by clinical and radiological findings. Patients with preoperative varus or valgus deformity of more than 15° were excluded from the study. Patients who had undergone previous knee joint surgery or who could not be treated with an unconstrained TKA with a short stem were also excluded. The inclusion and exclusion criteria are described in Table 1.
Inclusion and exclusion criteria.

TKA: total knee arthroplasty.
The software used for the tracker pin-guided standard CAS was Ci Mi TKR Version 2.0 by BrainLAB/DePuy Orthopaedic Inc. (Johnson and Johnson, Leeds, UK). Anatomical landmarks were registered through the use of dual 3 mm unicortical pins drilled into the femur and tibia at a distance from the surgical approach as well as a pointer with passive infrared reflectors. The tibial cut was made first, followed by bone morphing of the femur and ligament balancing. Soft tissue release was performed to achieve a rectangular gap at 0° extension and the space between the distal femur and proximal tibia was stored. The knee was then brought to 90° flexion and the space between the posterior femoral condyles and proximal tibia recorded. The size and the position of the femoral component were adjusted on a computer model to achieve equal flexion and extension gaps. The planned femoral component was then rotated to achieve a rectangular flexion space at 90° flexion. Following this, the navigated anterior and distal femoral bone cuts were performed to within 1 mm as planned. The femoral chamfer cuts and tibial preparation were completed, followed by trial of the tibial and femoral components with a tibial insert. Further soft tissue release was made if necessary to obtain rectangular and equal flexion and extension gaps. Subsequently, the appropriately sized tibial and femoral components were implanted with cement, the final flexion and extension gaps recorded.
In the pinless navigation group the BrainLAB VectorVision Knee 2.5 Navigation System (Brainlab) was employed for navigation. The pinless-navigated TKA was performed with the use of a stand-alone computer with infrared camera coupled with proximal tibia and distal femur reference arrays comprising four passive infrared reflector spheres. The distal femur cutting block was orientated using the conventional femoral intramedullary rod for TKA. The distal femur reference array was then rigidly inserted into the cutting block slot and the alignment verified with navigation. Femur registration was performed by acquiring the femoral head centre, femoral mechanical axis and rotational references. Tibia registration was performed by acquiring malleolar points, tibial mechanical axis and anterior–posterior direction. If the alignment was more than 2° from the mechanical axis of the femur, the cutting block was adjusted to within 1° of the mechanical axis. The proximal tibia cut was performed and the process was repeated for the distal femur cutting block.
All surgeries were performed using the standard medial parapatellar quadriceps splitting approach with patella eversion under tourniquet control at 300 mmHg with prostheses from DePuy Synthes Sigma® Fixed Bearing Knee system (Warsaw, Indiana, USA), a posterior cruciate retaining system and closure of wounds was performed in a standard manner.
Clinical outcomes were evaluated prospectively with the Knee Society Score (KSS), 9 SF-36 questionnaire 10 and the Oxford Knee Score (OKS) 11 at 6-month and 2-year intervals in addition to preoperative demographic data including body mass index (BMI), age and gender. The study was approved by our Institutional Review Board.
Statistical analysis
Power analysis was done prior to the conduct of this study, based on the difference in post-operative Knee Society Knee Score (KSKS). To detect a difference of 10 from a mean score of 88 at the author’s institution, a sample size of at least 95 patients in each group would be required to achieve a power of 0.95. This calculation was done for a two-sided test with a type I error of 0.05. After including all the patients who underwent computer-assisted TKA by a senior adult reconstruction surgeon between November 2008 and October 2012, there were 100 patients in both the pinless and the CI groups.
Statistical analysis was carried out in consultation with the in-house biostatistician, using SPSS® 19.0 (IBM, Armonk, New York, USA). Statistical significance was defined as a p value of ≤0.05. The Student’s unpaired t-test was used to compare the two groups for continuous variables (age, BMI, duration of surgery, Knee Society Function Score, KSKS, OKS, Physical Component Score (PCS) and Mental Component Score (MCS)), while the Pearson’s χ 2 test was used for the analysis of categorical variables (gender and side of operated knee). Paired t-test was used to evaluate the improvement in clinical outcomes at 2-year follow-up compared to preoperative values.
Results
There was no difference in age, BMI, gender or site of surgery between the pinless and tracker pin-guided navigation group (Table 2). However, the duration of surgery was shorter in the pinless group at 72 ± 13 min compared to 83 ± 11 min in the tracker pin-guided navigation group (p < 0.001). The knee range of motion of both groups was similar preoperatively.
Patients’ demographics and range of motion.
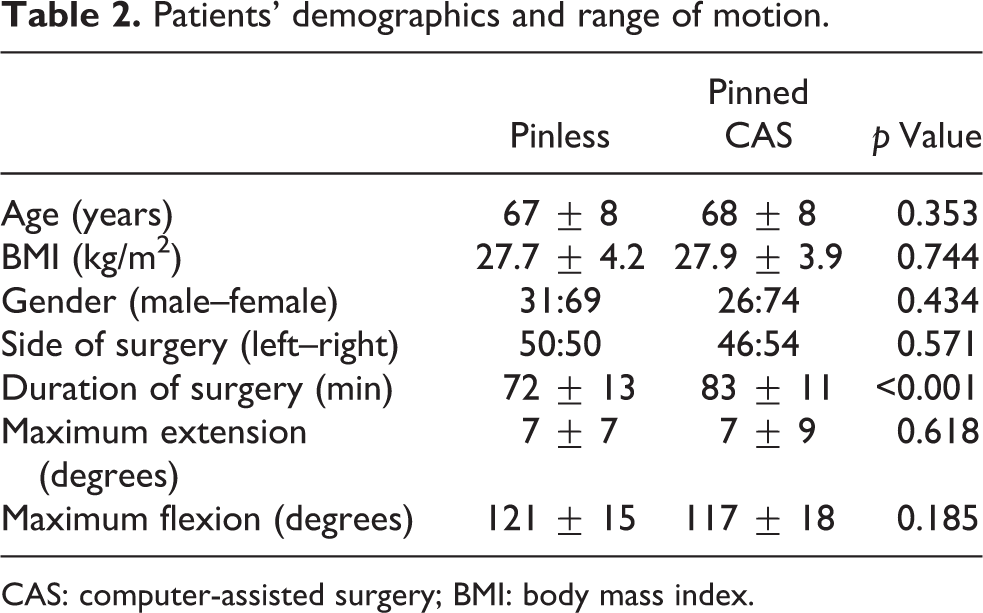
CAS: computer-assisted surgery; BMI: body mass index.
There was a significant improvement in both the function and the knee subcomponent scores of the KSS in the pinless navigation group from 55 ± 19 to 77 ± 18 (p < 0.001) and 39 ± 16 to 87 ± 10 (p < 0.001), respectively. This improvement was similarly reflected in both the PCS of the SF-36 questionnaire and the OKS from 33 ± 10 to 49 ± 8 (p < 0.001) and 34 ± 8 to 18 ± 5 (p < 0.001), respectively. The patients in the tracker pin-guided navigation group experienced similar statistically significant improvement in clinical outcomes as detailed in Table 3. Although there was a statistically significant difference in KSS knee subcomponent score and SF-36 MCS between the groups at 6-month follow-up, the difference was not apparent at 2-year follow-up.
Functional outcome scores.

CAS: computer-assisted surgery.
The proportion of varus knees undergoing TKA was similar in both groups with an average of 2 ± 7° and 3 ± 6° varus in the pinless and pinned CAS group respectively as reflected in Table 4. Both groups had significant correction of varus to a valgus tibio-femoral angle of 5°. Neutral lower limb mechanical axis correction was achieved in both groups.
Radiological measurements.

CAS: computer-assisted surgery.
With regards to complications, there was one case of superficial wound infection requiring wound debridement and one case of loose cement body requiring arthroscopic removal in the pinless group. One case of superficial wound haematoma was noted in the standard CAS group. There was no occurrence of pin tract-related complications in the tracker pin-guided standard CAS group.
Discussion
The study revealed a shorter duration of surgery in TKA with CAS using pinless navigation versus standard CAS which corresponds to an earlier study by Chen et al. 6 CAS TKA conventionally led to a longer mean duration of surgery of 23% 5 when compared to conventional TKA largely due to time expenditure in placement of additional reference landmarks including the tibial and femoral tracker pins. Pinless navigation circumvents the surgical time spent on the drilling and removal of tracker pins, reducing the duration by 11 min using the navigation system described in this study.
Previous studies have demonstrated that pinless navigation achieves satisfactory post-operative mechanical leg axis alignment and no significant difference in coronal alignment in both tibial and femoral component placement when compared with conventional TKA. 12 In addition, Chen et al. have found that pinless navigation is an effective tool for reducing the proportion of outliers of normal alignment. 13 However, whether the satisfactory alignment or decreased proportion of outliers translated to any detectable differences in clinical outcomes was not previously described. Previous studies have demonstrated that good placement of the implants within 3° of the mechanical axis of the lower limb reduces the wear of the implants and prevents implant failure. 14,15 This study has demonstrated that pinless navigation results in significant improvement in clinical outcomes at 2-year follow-up which is comparable to the improvement in patients who underwent standard tracker pin. A randomized comparative trial by Cip et al. demonstrated no difference in clinical outcome parameters between computer-assisted arthroplasty and conventional TKA after 5 years of follow-up. 16
Although there was no occurrence of pin tract-associated complications in this study, literature describes the incidence of pin tract-related femoral and tibial fractures at 1.3% and 1.4%, respectively. 17 The incidence of pin site pain and infection was also reported at 0.5% and 1.2%, respectively. 18 Bonutti et al. 19 described additional potential problems from femoral and tibial tracker placement including referencing mistakes, tracking errors and soft tissue morbidity from tracker placement.
The evidence presented in this study and current literature does suggest that pinless navigation provides similar clinical improvement at 2 years compared to tracker pin-guided navigation in TKA without the undesired risks of pin-associated complications. However, the surgeon must be cognizant of inability to account for soft tissue balancing and rotational alignment of the femoral component as described by Maderbacher et al.8 and the inability to target implant sizing in the pinless navigation described in this study. In this study, the implant sizes were decided using the same techniques employed in conventional surgery.
The limitations of this study include the inability to generalize the results for other pinless navigation systems, such as the Stryker® eNdtrac Articular Surface Mounted Knee Navigation System (Stryker Navigation, Kalamazoo, Michigan, USA) investigated by Keyes et al., 7 because of inherent differences in workflow. A longer duration of follow-up is also necessary to detect complications such as implant revision or incidence of peri-prosthetic fracture. The lack of randomization also impairs the ability to detect bias in patient selection and thus influencing outcomes analysis.
Conclusion
Pinless navigation in computer-assisted TKA achieves significant improvement in clinical outcomes at 2 years of follow-up that is comparable to the results achieved in standard tracker pin-guided navigation in CAS. This is coupled with a shorter duration of surgery as well as elimination of pin-related complications. A longer follow-up study will be crucial in determining whether this improvement is sustained and detecting differences in long term complications after arthroplasty.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.