
Abstract
Purpose:
There is direct literature conflict regarding coronal plane contracture or laxity in the end-stage varus osteoarthritic knee. Understanding the preoperative soft tissue status is important for optimizing the soft tissue envelope during total knee arthroplasty (TKA).
Methods:
The lower limb was manipulated using computer navigation, prior to surgical releases, to allow the limb weight-bearing axis to pass through the knee centre in maximum extension and 20° of flexion. Coronal plane laxity was measured in 78 varus (−7.7° ± 2.8°) knees as medial and lateral displacement from this point and compared to published values for healthy subjects.
Results:
Medial contracture was present in 12.8% (10/78) of the knees. Of these 10 knees, 5 displayed abnormal lateral laxity. Knees with a contracture in maximum extension also displayed a significant decrease (p < 0.0001) in medial laxity at 20° of flexion compared to non-contracted knees. In maximum extension, 19.2% (15/78) of knees had abnormally increased lateral laxity, 10 did not have a medial contracture. The remaining five knees with increased lateral laxity or 6.4% (5/78) of the total cohort also displayed a medial contracture. Lateral laxity increased significantly with increasing varus deformity. Medial laxity did not significantly decrease when comparing varus deformity of 5–10° versus >10°.
Conclusion:
The majority of varus knees with deformity of up to 15° have neither a medial contracture nor abnormal lateral laxity when referenced to the individualized neutral axis of the knee. Surgical releases during TKA should be uncommon. Medial contracture when present is influenced by both posterior and medial structures. Lateral laxity is a more consistent feature of the varus knee. The patterns of contracture and laxity are variable with limited correlation to deformity.
Introduction
Surgical releases advocated for medial contractures in the varus knee are well-documented. 1 The orthopaedic literature is inconsistent regarding the presence or degree of medial contracture in the varus osteoarthritic (OA) knee. 2 –5 Understanding the soft tissue envelope of the knee prior to total knee arthroplasty (TKA) is important for optimal surgery.
Bellemans et al. and Hohman et al. utilized computer navigation as a measuring device and both suggested medial contracture to be present with varus deformity greater than 10. 2,3 Matsumoto et al. found increased soft tissue disturbance in knees with greater than 20° of preoperative varus deformity but as they did not examine the amount of resected bone, it may be their measured gaps were due to the amount of bone resected rather than soft tissue disturbance. 4 In a similar study, Okamoto et al. measured both the intraoperative gaps and amount of resected bone to determine medial and lateral soft tissue laxity. They found the medial tissue to be non-contracted and increased lateral laxity in the varus knee with greater than 20° of deformity. 5 Therefore, the orthopaedic literature contains directly conflicting evidence for the effect of osteoarthritis on the coronal plane knee tissues.
These studies examine the knee in maximum extension, which means the posterior capsule and osteophytes may influence measures of coronal plane laxity. 2 –5 No study to date that we are aware of has examined the varus OA knee in both maximum extension and 20° of flexion in the same patient group.
The primary purpose of the study was to determine the overall effect of the OA process on coronal plane laxity of the varus knee at maximum extension and 20° of flexion. The secondary aim was to identify any deformity parameters associated with pathological tissue laxity. Given the conflict in prior literature, our null hypothesis was that medial contractures would not be present in the varus OA knee when referenced to the corrected, neutral axis of each knee.
Materials and methods
Seventy-two computer-assisted surgery (CAS) TKA patients contributing 79 knees were included in the study. Inclusion criteria were patients with varus degenerative osteoarthritis of any degree scheduled for primary TKA who had not undergone previous ligament reconstruction surgery, knee osteotomy or suffered other trauma likely to distort the periarticular soft tissues. Exclusion criteria were patients who declined consent or where intraoperatively placement of navigation pins was considered high risk due to poor bone stock or soft tissue. Ethical approval was obtained from the relevant institutional review board and written informed consent was obtained preoperatively for all patients. The measurement technique utilized has been previously described. 6
A prestudy power calculation was undertaken. Based on prior literature, to detect a difference in medial and lateral laxity of 1° between healthy and OA with a power of 80% and significance set at 0.05, we required 16 subjects and using the same parameters to detect a difference in neutral alignment of 1° between our subjects and previously published population normative values required 68 subjects.
A medial para-patellar approach to the knee was undertaken. Femoral and tibial navigation pins were inserted. All landmarks were identified and registered in the navigation system for calculation of the mechanical axes of the femur, tibia, lower limb and generation of an individualized 3D model of the patient’s anatomy using computer navigation software (BrainLab, Munich, Germany). The status of the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) was recorded. The ACL and PCL were left intact during laxity measurements. Osteophytes were left in situ to assess the knee as close to its pathological OA state as possible. The anterior horn of the medial meniscus was left intact. If required for accurate navigation registration, release of the deep band of the medial collateral ligament was limited to 5 mm by sharp dissection in order to maintain the state of medial soft tissues as close to the preoperative state as possible similar to the methods of Bellemans et al. 2 The patella was reduced and the degree of fixed flexion deformity (FFD) or hyperextension was recorded in maximum extension. The mechanical axis of the limb was corrected to the centre of the knee by observing CAS displays. The femoral and tibial mechanical axes were manipulated to be as colinear as possible to the limb axes at this position. These methods produced a limb position acting to define a neutral, corrected alignment for each knee consistent with prior literature. 7,8 The hip knee ankle angle (HKAA) was recorded at this point. The knee was moved through a medial–lateral arc via manual force from this corrected position. Measurements were defined by medial and lateral deviation from the corrected axis point in degrees as indicated by the navigation software. Direct observation of the joint was undertaken during measurements to prevent subluxation, rotation and ensure congruency (Figure 1). These measurements were undertaken in maximal extension and 20 degrees of flexion to remove the influence of the posterior capsule and osteophytes. The point of maximum varus deformity or the ‘loaded HKAA’ was recorded and this degree of deformity (0–5; 5–10; >10°) was used to group subjects for comparison of whether there was a significant alteration in medial and lateral laxity as varus deformity increased.

Demonstration of the correction of the mechanical axis to an individualized neutral point for each knee. Medial and lateral laxity was measured in maximum extension and 20° flexion as deviation from this point.
Modern navigation systems have been validated for these measurements. 2 A medial coronal plane contracture was considered present when the knee could not be aligned to its neutral, corrected axis (irreducible contracture) or when the knee did not correct beyond its neutral axis displaying movement within previously documented physiological ranges for elderly controls (reducible contracture). 9 In these circumstances, medial laxity was recorded as zero. Lateral laxity was considered abnormal when it exceeded 8°. 2,9,10 Once the data were recorded, a CAS TKA was performed. In all cases, the procedure and measurements were performed by a single, high-volume arthroplasty surgeon. All data were prepared and analysed using Prism 5 for Mac OS X Version 5 (Graphpad Software Inc, La Jolla, California, USA). Statistical comparisons were made using one-way analysis of variance with Tukey’s multiple comparison tests.
Results
Seventy-two patients contributed 79 TKAs. Five males and two females underwent bilateral TKAs. Table 1 demonstrates the demographics of the study population.
Patient demographic details.

BMI: body mass index; FFD: fixed flexion deformity; SD: standard deviation.
Seventy-eight knees were available to examine individual patterns of medial and lateral laxity. In one subject, the mechanical axis of the limb could not be manipulated to pass through the centre of the knee to attain a corrected, neutral axis in maximum extension or 20° of flexion (irreducible contracture). Therefore, no neutral point was attained from which to begin measuring and thus no medial and lateral laxity values could be recorded. This subject was a 54-year-old female with an FFD of 0.5° and a varus deformity of −13.5°. This patient was important to the study as a contracted knee. A medial contracture was present in 13.9% (11/79) of knees. Table 2 displays the patterns of contracture and laxity in the remaining 78 patients compared to published values in healthy knees.
Distribution of the laxity patterns in 78 subjects with individual laxity assessment.a
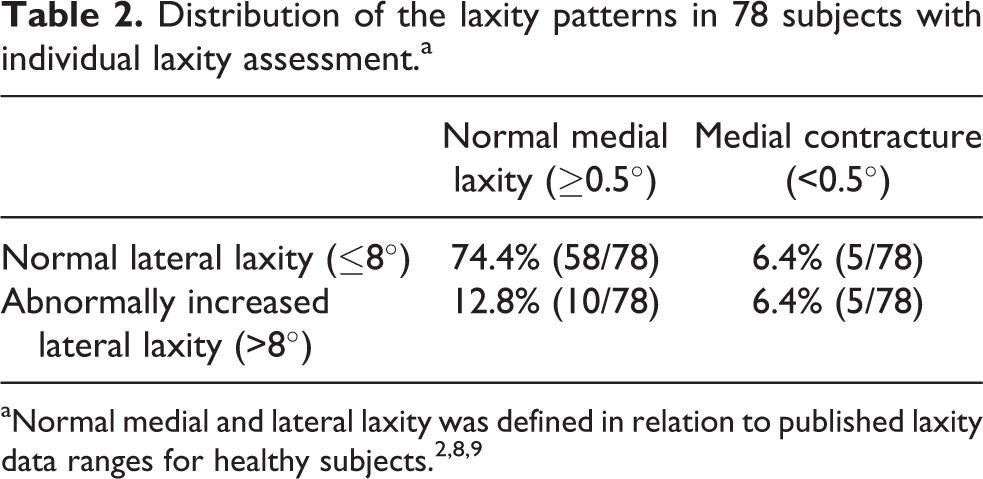
The majority of subjects (74.4%) recorded coronal laxity parameters within limits previously published for healthy knees. We then examined those subjects with medial contractures, abnormal lateral laxity and the relationship between varus deformity and soft tissue alteration in more detail.
The neutral, corrected HKAA in the 10 patients with a medial contracture who could be manipulated to but not beyond their corrected neutral axis point within physiological laxity ranges was −1.5° ± 0.9°. There was no significant difference between the neutral, corrected HKAA of these 10 contracted knees and the neutral, corrected HKAA of the 68/78 non-contracted knees (p = 0.819). A significant difference 2.3° ± 0.9° (p = 0.015) was seen between the mean maximum varus (loaded axis) of contracted (−9.7° ± 0.8°, −14.5° to −6.5°) and non-contracted knees (−7.4° ± 0.3°; −15° to −2°).
In 20° of flexion, a significant mean difference of 2.2° ± 0.5° (p < 0.001) in medial laxity persisted between contracted and non-contracted knees. Two of the 10 contracted knees were still unable to be manipulated in 20° of flexion beyond their neutral, corrected HKAA within physiological ranges. In these knees, medial laxity was recorded as 0. The other eight knees now displayed medial laxity within ranges previously published for healthy knees.
Contracted knees were laxer laterally. A significantly increased difference in the mean lateral laxity of contracted versus non-contracted knees in maximum extension of 2.2° ± 0.8° (p = 0.01) and 20° of flexion of 2.4° ± 0.9° (p = 0.008) was recorded (Table 3).
Laxity data in degrees for all knees, with comparison of contracted (those attained a neutral point but not move beyond this point with laxity consistent with prior published values for healthy knees) versus non-contracted knees.

We then examined the entire cohort for changes in medial and lateral laxity by grouping subjects according to their maximum varus deformity and comparing laxity parameters between these groups. Medial laxity decreased as the varus deformity of the limb increased. Figure 2 demonstrates a statistically significant mean difference in medial laxity between 0–5° versus 5–10° but non-significant for 5–10° versus > 10° in both maximum extension and 20° of flexion.

Medial laxity compared to subjects grouped by the maximum varus deformity.
Lateral laxity increased as the varus deformity of the limb increased. There was a highly significant increase (p < 0.001) in laxity between each group of increasing varus deformity in both maximum extension and 20° of flexion (Figure 3).

Lateral laxity compared to subjects grouped by maximum varus deformity.
We analysed the soft tissue parameters in maximum extension and 20° of flexion to confirm that a true difference existed between these two measurement positions. We found the coronal soft tissues to have a total medial–lateral coronal arc at 20° of flexion (9.7° ± 2.4°) that was significantly greater (p < 0.001) compared with the arc demonstrated at maximum extension (7.7° ± 2.3°). Both medial and lateral laxity for 20° flexion versus maximum extension was significantly increased with mean differences of 1.4° (p < 0.001) and 0.6° (p = 0.007).
We also identified unexpected patterns of laxity. More medial laxity than lateral laxity at full extension was recorded in 6/78 (7.6%) knees. Five of these six knees maintained the same pattern at 20° of flexion, while six other knees displayed greater medial than lateral laxity at 20° of flexion. Therefore, at 20° of flexion, 14.1% (11/78) of knees had greater medial than lateral laxity.
Discussion
The effect of OA on the knee soft tissues still requires comprehensive definition and is important for intraoperative TKA decision-making. Studies to date have examined the coronal plane tissues of the knee in a single position preoperatively, varied positions intraoperatively after bony resection or post-operatively without reference to initial soft tissue parameters. 2 –5,10 –13 The preoperative studies have reported directly contrasting findings as to the presence of coronal plane tissue abnormalities and the influence of deformity on these parameters. 2 –5 These differences may reflect varied study techniques, especially the ‘zero’ point from which measurements occur. By individualizing the initial ‘zero’ point with the use of the limb mechanical axes, our results help reconcile these differences.
The purpose of this study was to define the effect of end-stage OA on the coronal plane medial and lateral laxity of the knee prior to TKA. In each knee, we individualized the initial point from which measurements were taken and compared these subsequent measurements to published values for healthy subjects to assess the impact of OA on the coronal plane laxity of the knee. In the healthy knee, medial and lateral laxity is measured as deviation from the resting point of the knee. This point is not constant between subjects and is typically not 0°. Therefore, it is illogical to measure OA knees all from a single standardized point. Studies of healthy knees demonstrate mean HKAA values between −1° and −1.3° and standard deviations in these studies between 2 and 2.8. 7,8,14 –17 The laxity measures documented from these resting positions in normal subjects are displayed in Table 4. 9,10,18 –21
Literature review of in vivo coronal plane laxity in the normal and OA knee.a

OA: osteoarthritic; CAS: computer-assisted surgery.
aMean with standard deviation data.
OA alters the initial position of the knee and lower limb. If we cannot return the knee to its predisease position, it makes it problematic to determine any medial and lateral distortion of the soft tissues by OA. Previous studies have used differing techniques to address this issue. Bellemans et al. and Hohman et al. both determined contracture to be present based on whether a knee could be realigned to an HKAA of 0°. One study removed osteophytes prior to measurement, one did not. 2, 3 The healthy knee has a mean HKAA of −1.33° ± 2.34°. 7 The mean medial and lateral laxity in extension has been reported in the elderly healthy knee to be 2.3° ± 0.9° and 2.8° ± 1.3°, respectively. 9 An OA knee that had a predisease HKAA of −4° (varus) is unlikely to realign to an HKAA of 0° whether or not a medial contracture is present. Therefore, whether a varus knee can attain an HKAA of 0° is not definitive evidence for the presence or absence of a medial contracture.
Other studies have assessed the absolute gap with tensor devices after bone resection, with or without the consideration of the amount of bone resected. 4,5 This approach measures gaps after alteration of both the bony and ligamentous anatomy of the knee and equalization of pressure on the medial and lateral sides of the knee. It does not account for the initial position of the limb or the fact that medial and lateral laxity is typically different in in vivo studies, confirmed by a recent cadaver study. 9,10,18 –22
To address these concerns, we utilized CAS to place the mechanical axis of the limb through the centre of the knee, while ensuring congruency of the joint under direct vision and made the femoral and tibial mechanical axes as colinear as possible. This created a corrected or neutral HKAA position for each knee that is consistent with prior literature and allowed the measurement of laxity to occur from an individualized point for each subject. 7,17 It is important to note in this circumstance, an HKAA of 0° will only occur when the tibial and femoral axes match at the knee and they are both colinear with the mechanical axis of the limb. More commonly, the neutral HKAA will approach 0° as seen in Figure 1. In our subjects, the mean corrected HKAA in maximum extension was −1.4 ± 1.3 with a range of 1.5 to −5.5. This is similar to the mean HKAA and varus range in the healthy population. 7 We believe these factors mean our neutral point from which we measured medial and lateral laxity in each knee is a close approximation of the predisease alignment of that knee. This method addresses many of the issues demonstrated in previous studies that have sought to examine the alteration of coronal plane knee tissues by OA without seeking to individualize the position from which measurements were undertaken. 2 –5
Our results have demonstrated the variable nature of laxity patterns in the coronal plane of the varus OA knee with up to 15° of deformity. Our findings support both the findings of contracture and laxity by previous authors but place them in a more individual context and help reconcile the conflicting prior findings in the orthopaedic literature. 2 –5 The ‘classic’ pattern of contracted medial tissue and lax lateral tissue was only recorded in 6.4% (5/78) of patients. Medial contracture and lateral laxity also exist in isolation with normal tissue laxity found on the opposite side of the joint in many patients. The majority of patients in this study had medial and lateral laxity measurements within ranges previously described for healthy subjects. 9,18 –21
We found a medial contracture to be present in 13.9% (11/79) of patients in maximum extension. As no significant difference was found between the neutral corrected HKAA of contracted and non-contracted knees, initial alignment did not appear to contribute to deformity and contracture. Hohman et al. and Bellemans et al. found contractures were likely with varus deformity beyond 10°. In our subjects, knees with contracture had a significantly higher mean maximum deformity value than non-contracted knees but displayed a range of maximum deformity of −6.5° to −14.5°. In the cohort as a whole, we found a non-significant decrease in medial laxity comparing subjects with 5–10° of deformity to >10° of deformity. Our results mean increased varus deformity is often present with contracture but deformity of >10° is not a reliable proxy marker for the presence of contracture. When contractures are present, they have both a posterior and medial contribution as demonstrated by the significant difference in medial laxity between contracted and non-contracted knees at both maximum extension and 20° of flexion. The influence of posterior structures is also demonstrated by the fact that of the 11 subjects with contracture in maximum extension, only three met the same criteria for contracture in 20° of flexion.
The mean medial laxity in our subjects at maximum extension was 1.6° ± 1.0°, this compares to reported ranges in the healthy population between 2.3° and 3.6°. 9,10,19
These findings have disproved our null hypothesis that medial contracture is not present in the varus OA knee when referenced to the corrected, neutral HKAA of each knee. Importantly, contracture is relatively uncommon, not clearly related to the degree of varus and when present typically small. Furthermore, given that laxity measurements were performed with osteophytes in situ, the presence and degree of contracture in the medial tissue are likely to be even smaller than we documented once osteophytes are removed during the operative process.
Studies of healthy knees have shown mean lateral laxity in either maximum extension or 10° of flexion varying between 4.1° and 4.9°. 9,10,19 In a study utilizing similar investigative techniques to ours, Jenny found a range for lateral laxity in maximum extension in healthy subjects of 2–8°, similar findings are seen in other studies. 2,9,10 Our subjects had a mean lateral laxity of 6.1° ± 2.5°. In our subjects, 19.2% (15/78) of knees had lateral laxity of more than 8° (8.5–11.5°) in maximum extension. We found a significant increase in laxity as varus deformity increased. Therefore, we would agree with the findings of Hohman et al. who described lateral laxity in the varus knee with more severe deformity. 3 We have been able to better quantify the individual degree and patterns of increased laxity showing it can exist in isolation or combined with a medial contracture.
Counter intuitively given the varus alignment of our subjects, 6/79 (7.6%) knees in extension and 11/79 (13.9%) knees in 20° of flexion showed an unexpected pattern of increased medial versus lateral laxity. This has not been previously reported.
These findings have direct relevance to TKA. Surgeons should not assume laxity patterns based on deformity or that abnormality in the coronal plane of the knee on one side of the joint correlates to abnormality on the opposite side of the joint. The ‘releases’ that occur as part of the approach to the knee during TKA and resection of osteophytes will likely address the degree of medial contracture we have demonstrated in the majority of cases with a varus deformity of up to 15°. 21 Therefore, if an extensive medial release is required, it may represent an uncommon clinical situation or reflect errors within the surgical procedure. If a contracture is present, then both a medial and posterior cause should be sought given the decreased laxity we demonstrated in contracted knees in both maximum extension and 20° of flexion. In patients with abnormal lateral laxity, the surgeon should not release medial tissue to attain balance based on abnormal lateral tissue and careful surgical technique should avoid any further increase in lateral laxity to potentially problematic levels. The potential issues associated with this are well addressed by Matsuda and Ito. 23
We would acknowledge the limitations of our study. The patient group was predominantly Caucasians and their selection for TKA may not be indicative of other surgical series. The principle of constitutional varus is well established within the orthopaedic literature. 7 While we attempted to individualize our measurements, this factor may have contributed to those knees determined to have contracture, particularly an irreducible contracture. Our study is consistent with described in vivo techniques for measuring coronal plane laxity and our subjects had flexion and varus deformity parameters similar to previously examined OA knee groups in the literature. 2,3,7 –9,18,19,24,25 Many studies define coronal plane knee laxity by a total arc of movement at 20° of flexion and our findings are consistent with these prior studies. 18,24,25 Therefore, we believe the findings of our study are valid in the OA knee with varus deformity of up to 15°.
The testing method is operator dependent; however, a number of steps were undertaken to minimize variation. Manual stress testing in a manner consistent with prior studies was performed to assess coronal plane laxity. 2,10 While an experienced surgeon performed this, some degree of variability in exerted forces is inevitable. Mitigating this is the fact that ligaments are viscoelastic and measurements were recorded at maximal displacement. This should correspond to the plateau of the tension/length curve minimizing any effects of variation in force. 10 It is not possible in an in vivo setting to utilize the same invasive techniques with multiple controlled parameters and measurements seen in cadaver studies given the ethical implications of prolonging surgery. 22
We cannot know that the corrected, neutral HKAA was the best starting point from which to measure medial and lateral coronal laxity but believe it valid for the following reasons. Our corrected, neutral HKAA range of 1.5° to −5.5° is consistent with the varus HKAA range demonstrated by Bellemans et al. in the healthy population of 0° to −8°. 7 Our measurements were non-weight bearing. Studies show increased varus alignment with weight bearing of 1.6–2°. 26 An increase in varus alignment would have acted to further normalize our HKAA range and medialize the initial corrected, neutral point. The effect of measuring displacement from a more varus starting position would have been to increase the medial and decrease the lateral laxity measured further normalizing our results and confirming the fundamental findings of our article.
In conclusion, we have demonstrated a method of individualizing the measurement of medial and lateral laxity in the OA knee. We have shown medial contractures referenced to the individual corrected, neutral axis of the varus OA knee with up to 15° deformities are uncommon. When present, they are relatively small and occur via contributions from both medial and posterior structures. Increased lateral laxity is a more common finding but the patterns of coronal plane laxity alteration in the end-stage OA knee at the time of TKA are highly variable, have not been previously documented and correlate poorly with the initial or subsequent varus deformity of the limb. Our findings help reconcile the previous conflict in the orthopaedic literature. Given our findings that many knees can be placed in an alignment where medial and lateral tissue laxity is consistent with laxity found in healthy subjects, this may help minimize the inevitable distortion of the soft tissues by TKA and may be a means of improving patient-based outcomes. An awareness of these findings will assist the surgeon during TKA to optimally balance and normalize the coronal plane soft tissues.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.