
Abstract
Background:
Joint gap unbalancing during total knee arthroplasty (TKA) induces flexion contracture. Flexion contracture is one of the most serious complications of TKA. When flexion contracture is found during surgery, intraoperative manipulation is often empirically performed. We evaluated the effects of intraoperative manipulation on joint gap and postoperative flexion contracture.
Materials and methods:
TKA was performed for 136 knees. Intraoperative manipulation was performed for flexion contracture in 61 knees. Joint gap changes before and after manipulation were measured at six positions from extension to 120° of flexion. Manipulation was not performed for 75 knees. The extension angle was measured radiographically immediately after surgery, at 3 months, and 6 months postoperatively. Extension angles with manipulation and without manipulation were compared.
Results:
Joint gap changes (mm) before and after manipulation were 0.1, 0.0, −0.2, −0.3, −0.1, and −0.3 at 0°, 30°, 45°, 60°, 90°, and 120° of flexion, respectively, indicating that manipulation could not change joint gaps significantly. Extension angles (°) with and without manipulation were −4.0 ± 4.6 and −3.8 ± 3.9 immediately after surgery, −5.3 ± 6.7 and −5.5 ± 6.2 at 3 months postoperatively, and −2.7 ± 6.0 and −3.8 ± 5.8 at 6 months postoperatively. No statistically significant difference existed between the values with or without manipulation during all periods.
Conclusion:
Intraoperative manipulation does not enlarge the gap or resolve postoperative flexion contracture. Developing the new surgical technique is required to achieve perfect balance at TKA.
Introduction
Joint gap balancing during total knee arthroplasty (TKA) is important for ensuring postoperative joint stability and range of motion. 1 –3 Many reports have described postoperative joint instability as one of the most important reasons for revision surgery. 4 –7 Ideally, the joint gap should be balanced to ensure joint stability. However, it is not easy to achieve perfect balance during TKA. For example, the prominent posterior condyle of the femoral component will tighten the posterior capsule, resulting in a smaller extension gap (compared to the flexion gap). 8,9 In addition, the flexion gap tends to be larger than the extension gap after posterior-stabilized TKA because the posterior cruciate ligament resection selectively enlarges the flexion gap. 10 –13 Therefore, a tibial insert with the same thickness as the flexion gap is typically selected to avoid flexion laxity. However, this relative extension gap shortening can induce flexion contracture. 14,15 When flexion contracture is found during surgery, many surgeons empirically manipulate the knee with flexion contracture to achieve full extension (Figure 1); however, there is little quantitative data regarding this method. This study aimed to investigate the effects of intraoperative manipulation on the joint gap and postoperative extension angle in living patients who underwent TKA.

Intraoperative manipulation was empirically performed to force the flexion contracture knee to reach full extension. (a) Before manipulation. (b) At manipulation.
Materials and methods
Between July 2013 and December 2015, TKA was performed for 136 knees using Vanguard PS system (Biomet, Inc., Warsaw, Indiana, USA). The patient population comprised 118 women and 18 men with a mean age of 78.0 years (range, 62–88 years). All study participants provided informed consent, and the study design was approved by the appropriate ethics review board. Two surgeons at one hospital performed all TKA procedures with a medial parapatellar approach and using the following measured resection method. Osteotomy of the distal femur was performed perpendicular to the mechanical axis, with external rotation of 4° to the posterior condylar axis. Osteotomy of the proximal tibia was performed perpendicular to the mechanical axis, with a 3° posterior slope and rotation along the line connecting the center of the attachment of the posterior cruciate ligament to the medial one-third of the tibial tuberosity.
All measurements of the joint gap were performed with a special tensor (TRUE TENSOR; Biomet Japan, Inc., Tokyo, Japan) with the same design as a total knee prosthesis to reproduce conditions after implantation 16 (Figure 2). The tensor was set and fixed, and the femoral and patellar trial components were mounted. The patellofemoral joint was reduced and repaired temporarily with two stitches. Then, we loaded the joint distraction force (130 N) several times until the joint gap remained constant to reduce the error that can result from creep elongation of the surrounding soft tissues. Joint gaps were measured at six positions from extension to 120° of flexion (0°, 30°, 45°, 60°, 90°, and 120° of flexion).

The tensor consists of three parts: an upper seesaw flat platform with an attachment that is shaped to match the articular surface of tibial insert, a lower flat platform plate, and an extra-articular main body.
The joint gap was measured immediately after bone resection. If the extension gap was 2 mm smaller than the flexion gap at 90°, the manipulation was performed as follows (manipulation group; 61 of 136 knees). First, all trial components were mounted. Second, we inserted a tibial insert 2 mm thicker than the extension gap measured by TRUE TENSOR. For example, extension gap at 0° was 10 mm and flexion gap at 90° was 12 mm. A tibial insert with 12 mm thickness was inserted. Third, we stretched the knee completely (flexion angle was 0°) by holding the heel and pushing the knee and maintained the position for 10 min. Tourniquet was not released during manipulation. After manipulation, the joint gap was measured again. We examined the gap before and after manipulation and made comparisons. After all measurement, we checked the cut surface of proximal tibial and confirmed there was not collapse.
The remained 75 of 136 knees were not performed manipulation because the extension gap was not 2 mm smaller than the flexion gap at 90° (no manipulation group).
After all gap measurements, three surgeons agreed to select the thickness of the tibial insert with reference to the stability of knee motion. The final decision was made when two or all surgeons selected the same thickness. If each of the three surgeons selected different thickness, the intermediate thickness was selected.
We defined “Gap-difference” as the discrepancy obtained by subtracting the extension gap from the thickness of the tibial insert actually inserted (Figure 3). Patients in both groups (manipulation group and no manipulation group) were divided into four subgroups according to Gap-difference (subgroup 0, 0 mm; subgroup 1, 1 mm; subgroup 2, 2 mm; and subgroup 3, 3 mm). We compared the extension angle of the manipulation group with that of the no manipulation group for each Gap-difference.
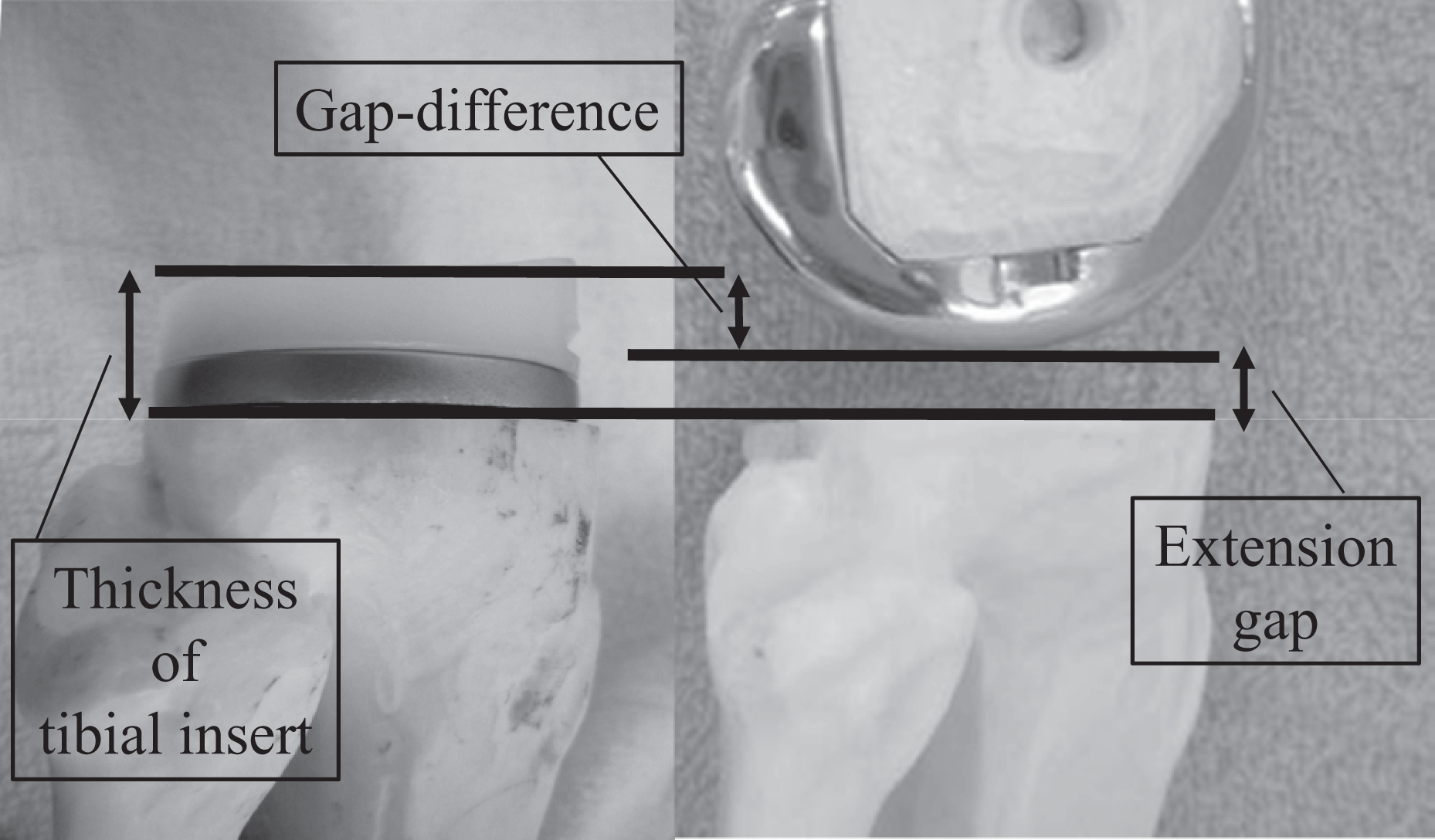
“Gap-difference” was defined as discrepancy obtained by subtracting the extension gap from the thickness of the polyethylene insert actually inserted.
The extension angle was measured preoperatively, immediately after surgery, and at 3 and 6 months postoperatively. The extension angle was measured between the axis of the distal femur and proximal tibia on the lateral radiograph with gravity. The positioning of both components was assessed using the Knee Society TKA roentgenographic evaluation. 17
Knee Society Score (KSS) and Knee Society Functional Score (KSFS) were recorded preoperatively and at 6 months postoperatively.
A paired t-test was performed to compare the differences in gaps before and after manipulation. An unpaired t-test was performed to compare the extension angle of the manipulation group with that of the no manipulation group for each Gap-difference. The results were analyzed using the statistical software package Statview 5.0 (Abacus Concepts Inc., Berkeley, California, USA). The level of significance was determined at p < 0.05.
Results
Characteristics of the patients in both groups were comparable (Table 1). The mean age, preoperative femorotibial angle, preoperative extension angle, operative time, blood loss, KSS, KSFS, and position of both components did not differ among the two groups.
Patient characteristics.

FTA: femorotibial angle; KSS: Knee Society Score; KSFS: Knee Society Functional Score.
In the manipulation group (61 of 136 knees), the mean joint gaps before manipulation were 10.0 ± 1.2 (mean ± standard deviation (SD)) mm, 11.9 ± 1.5 mm, 12.2 ± 1.5 mm, 12.3 ± 1.5 mm, 12.2 ± 1.4 mm, and 11.0 ± 1.2 mm at 0°, 30°, 45°, 60°, 90°, and 120° of flexion, respectively. After manipulation, the mean joint gaps were 10.1 ± 1.5 mm, 11.9 ± 1.5 mm, 12.0 ± 1.5 mm, 12.1 ± 1.4 mm, 12.0 ± 1.4 mm, and 10.6 ± 1.2 mm at 0°, 30°, 45°, 60°, 90°, and 120° of flexion, respectively (Figure 4). The joint gap changes with manipulation were 0.1 ± 0.5 (mean ± SD) mm, 0.0 ± 0.7 mm, −0.2 ± 0.8 mm, −0.3 ± 0.7 mm, −0.1 ± 0.5 mm, and −0.3 ± 1.0 mm at 0°, 30°, 45°, 60°, 90°, and 120° of flexion, respectively. Intraoperative manipulation did not enlarge the intraoperative joint gap.

Manipulation did not significantly enlarge the joint gap for all ranges of motion.
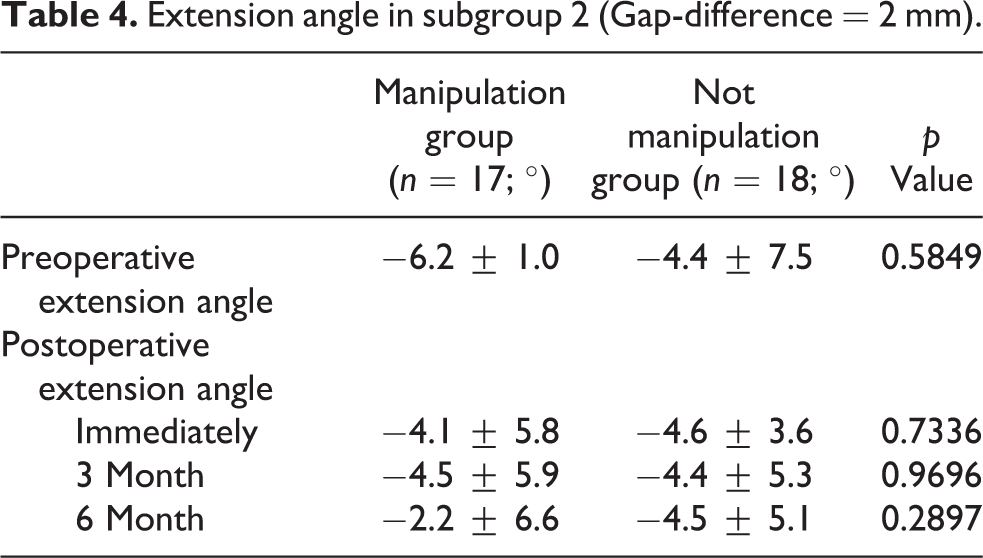
In subgroup 0, the extension angles (°) with and without manipulation were −2.2 ± 3.9 (mean ± SD) and −0.9 ± 4.9 immediately after surgery, −1.9 ± 7.6 and −3.9 ± 6.9 at 3 months postoperatively, and −1.2 ± 5.2 and −0.9 ± 5.3 at 6 months postoperatively. There was no statistically significant difference with or without manipulation during all periods (Table 2). In subgroups 1, 2, and 3, there were no statistically significant differences with or without manipulation during all periods (Table 3 to 5).
Extension angle in subgroup 0 (Gap-difference = 0 mm).

Extension angle in subgroup 1 (Gap-difference = 1 mm).

Extension angle in subgroup 2 (Gap-difference = 2 mm).
Extension angle in subgroup 3 (Gap-difference = 3 mm).

Discussion
Intraoperative manipulation has been empirically performed to achieve full extension during surgery; however, the findings of the present study indicated that intraoperative manipulation did not enlarge the gap and did not resolve the postoperative flexion contracture.
Perfect balancing during TKA is ideal. In those cases with perfect balancing, an insert with the same thickness as extension gap would be selected because all gaps at all flexion angles are same. But perfect balancing at all flexion angles is impossible. In posterior-stabilized TKA, there is no stabilizer for the anterior–posterior translation in the mid-flexion range. Minoda et al. reported that instability in the mid-flexion range is unavoidable in posterior-stabilized TKA. 18,19 In the present study, an insert with the same thickness as the extension gap was selected for only 21%. In the case of not-perfect balancing, we tend to choose a thicker insert to avoid joint instability; therefore, existence of the Gap-difference was inevitable. We compared the extension angle of the manipulation group with that of the no manipulation group for each Gap-difference. In each subgroup, there were no differences during all periods.
When flexion contracture occurs during TKA, the most reliable intraoperative method for resolving it is additional bone resection at the femoral distal plane and additional release of the posterior soft tissue. 20 These methods are troublesome because they involve resetting some instruments for bone cutting and soft tissue release and removal and resetting of trial components. Intraoperative manipulation has been empirically performed due to its simplicity. It is expected to tear the posterior joint capsule when the knees are forced to reach full extension. Although manipulation was often performed empirically, little quantitative data are available and its effects on the postoperative extension angle are unknown.
Previous studies have reported that postoperative manipulation is effective for resolving flexion contracture by releasing arthrofibrosis. 21 –23 However, intraoperative flexion contracture is not introduced by arthrofibrosis, but rather by the relatively small extension gap. Therefore, it appears that the mechanistic effects of intraoperative and postoperative manipulation are different. There is only one report about intraoperative manipulation that did not indicate a change in the joint gap. 24 However, it was a cadaveric study and did not mention the postoperative extension angle. To the best of our knowledge, this is the first report to quantitatively analyze the effects of intraoperative manipulation and postoperative flexion contracture. However, the findings of the present study indicate that intraoperative manipulation does not enlarge the gap and does not resolve the postoperative flexion contracture.
During this study, manipulation was performed for 10 min to create an extra 2-mm gap extension. More aggressive or longer manipulation might have resolved the flexion contracture. However, aggressive manipulation is dangerous because it could also cause collapse of the resection surface and supracondylar fracture in the osteoporotic bone. 25 Longer manipulation prolongs operative time. Ten minutes of manipulation is ideally suited for this procedure because surgeons must wait approximately 10 min for the cement to harden when they are placing pressure on the cement interface (e.g. via knee extension manipulation). Therefore, although longer manipulation time might increase the joint gap, it would also increase the operative time.
The current study had some advantages. First, we used a specially designed tensor device with the same design as a total knee prosthesis to reproduce the conditions after implantation. The precision of this tensor has been evaluated in the previous studies. 16,18,26,27 Second, the extension angle was measured radiographically. Many reports have already indicated that radiographic measurements are more accurate than those obtained using a goniometer. 28 –30
In addition, the present study had some limitations. First, this study investigated only a posterior-stabilized type of prosthesis, and the results likely cannot be generalized to a cruciate-retaining type of prostheses. However, for the cruciate-retaining type of prostheses, relative shortening of the extension gap is rare because flexion gap tightness is often induced by the posterior cruciate ligament. Second, a 6-month follow-up period might be inadequate. As the postoperative period elapses, the influence of intraoperative factors decreases. The extension angle after a long postoperative period would be strongly influenced by postoperative factors. The impact of intraoperative manipulation on postoperative flexion contracture would be small years after surgery.
Conclusion
In the present study, intraoperative manipulation did not change the joint gap. Therefore, if flexion contracture occurs during TKA, then additional bone cutting and soft tissue release are likely more appropriate than manipulation. Developing the new surgical technique is required to achieve perfect balance at TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.