
Abstract
Background
The improvement of flexion contracture is important in knee arthroplasty since residual flexion contracture postoperatively is associated with decreased quality of life and patient satisfaction. In this study, we investigated the effect of bi-cruciate stabilized (BCS)-type total knee arthroplasty (TKA) as compared to posterior stabilized (PS)-type TKA on osteoarthritic primary knees with flexion contractures.
Methods
59 TKAs from January 2014 to December 2020, of which 30 were PS-type TKAs (NexGen LPS-flexⓇ; 76.3 years, BMI 27.5) and 29 BCS-type TKAs (Journey IIⓇ; 72.5 years, BMI 28.6), were performed for knee osteoarthritis with preoperative flexion contracture of 15° or greater. Full extension was obtained intraoperatively during all TKAs. Clinical outcomes, radiological evaluations, and the amount of additional distal femoral osteotomy during TKA were evaluated in a retrospective study design.
Results
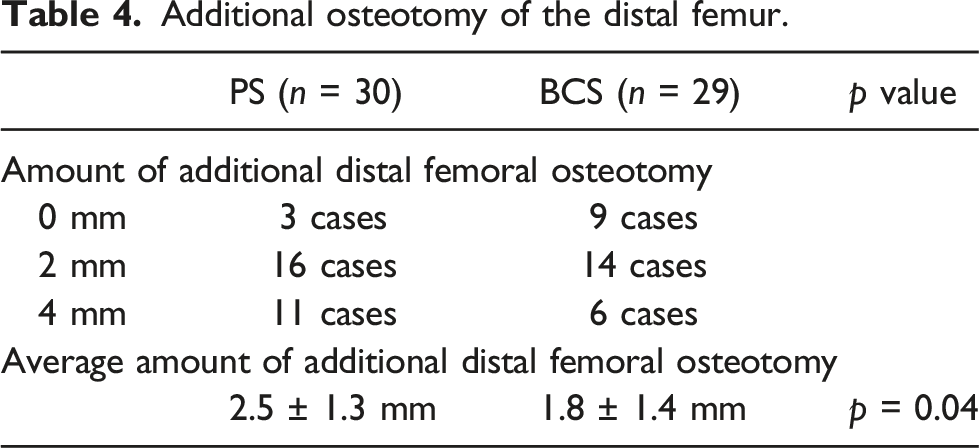
The range of motion improved in the both groups. Postoperative flexion contracture was significantly improved in the BCS group. Knee Society Score improved significantly in both groups, with no difference between the two groups. The amount of additional distal femoral osteotomy was 2.5 ± 1.3 mm for the PS group, and 1.8 ± 1.5 mm for the BCS group, showing a significant difference (p = 0.04).
Discussion
The BCS-type TKA significantly improved preoperative flexion contracture and reduced the amount of additional distal femoral osteotomy compared to PS-type TKA. This is attributed to the anterior cam in the BCS-type TKA, which leads to a smaller amount of protrusion of the posterior femoral condyle from the posterior margin of the tibial component in the BCS-type in knee extension, as compared to the PS-type.
Introduction
Residual flexion contracture after total knee arthroplasty (TKA) leads to a decrease in quality of life and patient satisfaction.1,2 Although various treatments are employed to achieve full extension intraoperatively, preoperative flexion contractures tend to persist postoperatively.1,3,4 Ritter et al. 1 reported that 8.5% of preoperative severe flexion contractures of 20° or more had residual contractures of 10° or more, and 5.4% of preoperative moderate flexion contractures of 6–19° had residual contractures of 10° or more after TKA. One of the causes is the large posterior protrusion of the femoral implant. Mitsuyasu et al. mentioned that the selection of a larger posterior femoral condyle implant increases posterior soft tissue tension. The resulting small extension gap makes full extension difficult, requiring additional distal femoral osteotomy or excessive soft tissue release. 5 Onodera et al. 6 reported that femoral implants with a larger posterior offset lead to relative shortening of the posterior soft tissues and are prone to flexion contractures. In addition, the posterior protrusion of the femoral implant may affect the ability to achieve full extension, especially in knees with preoperative flexion contractures as compared to knees without flexion contractures. Therefore, the posterior protrusion of the femoral implant need to be further reduced in TKA of knees with flexion contractures.
On the other hand, the anterior cruciate ligament (ACL) remains detached and uncompensated for in conventional TKA, which is a factor for poor TKA results. In 2005, Bellemans et al. developed a bi-cruciate stabilized (BCS)-type TKA that can compensate for this function and induce normal knee motion, medial pivot, and femoral roll-back.
7
The BCS-type TKA tibial post makes contact with the anterior-cam of the femoral component to compensate for ACL function, allowing this model to guide the femur forward in knee extension, a feature that lacks in models without an ACL compensating mechanism, such as PS-type TKA (Figure 1).8,9 We hypothesized that using a BCS-type TKA in a flexion-contraction knee would reduce the posterior protrusion of the femoral implant during knee extension and facilitate full extension after surgery. Based on the above background, the purpose of this study was to investigate the results of BCS-type TKA for flexion-contraction knees as compared to PS-type TKA. (a) Normal knee, (b) Conventional TKA, (c) BCS-type TKA (Provided by Smith and Nephew).
Materials and methods
Patient selection and methods
Six hundred and 44 primary TKAs were performed by an experienced orthopedic surgeon at the Department of Orthopedic Surgery, Japanese Red Cross Kyoto Daiichi Hospital, from January 2014 to December 2020. Inclusion criteria were as follows: medial osteoarthritis of the knee, preoperative flexion contracture of at least 15°, and full manual extension of the knee intraoperatively. The exclusion criteria were cruciate retaining and constrained type, and failure to follow up due to death during the course of the study. Fifty-nine patients were finally included in the study (Figure 2). Method of patient selection.
Characteristics of patients with preoperative flexion contracture knee of 15° or greater.

Surgical technique
The medial parapatellar approach and measured resection technique were used for all TKAs. After resection of the proximal tibia and distal femur from the lateral side with minimal cartilage degeneration according to the thickness of the implant, medial soft tissue release, medial osteophyte removal, and release of the soft tissue from the posterior joint capsule were performed to secure the extension gap. The femoral implant was positioned using the anterior referencing technique and ensured to be parallel with the surgical trans-epicondylar axis with reference to the preoperative epicondylar view (X-ray kneeling view), from which the condylar twist angle was measured.10,11 The tibial implant was positioned with reference to the Akagi line. 12 If full extension was not obtained after insertion of the trial components, an additional resection of the distal femoral condyle was performed. The amount of additional distal femoral osteotomy (2–4 mm) was defined as the amount of distal femoral osteotomy greater than the distal thickness of the femoral implant. Intraoperative additional distal femoral osteotomy volume was compared between the two groups.
Clinical outcomes and radiological evaluations
Clinical outcomes were investigated in terms of the Knee Society Score (KSS) and joint range of motion (ROM) at preoperative and final observation. One orthopedic surgeon evaluated the ROM on an examination table using a goniometer. Radiological evaluation of the standing femorotibial angle (FTA) pre- and postoperatively, the femoral and tibial component positions,
13
and the posterior condylar offset (PCO) pre- and postoperatively were performed.
14
The posterior offset ratio
6
was measured for 12 patients in the PS group and 12 patients in the BCS group, which were available among all patients. ‘Posterior offset ratio’ was defined as follows. The maximal protrusion of the posterior condyle, posteriorly to the extension line parallel to the tibial shaft from the edge of the posterior tibial component was measured on the true lateral radiographs (x). Antero-posterior diameter of the tibial component was also measured (y). ‘Posterior offset ratio’ was obtained by dividing ‘x’ by ‘y’ (Figure 3).
6
Radiographic images (lateral view of knee in extension after surgery), (a) PS-type TKA, (b) BCS-type TKA. The posterior offset ratio was obtained by dividing ‘x’ by ‘y’.
Statistical analysis
Radiographic evaluations were measured twice by one observer at different times to determine intra-observer reliability, and blindly and independently by two observers to determine inter-observer reliability using intra-class correlation coefficients (ICCs). ICCs of the intra-observer reliabilities (standing FTA, 0.99; implant position, 0.86; and PCO, 0.96) and inter-observer reliabilities (standing FTA, 0.98; implant position, 0.76; and PCO, 0.96) were satisfactory. Measurements are expressed as mean ± standard deviation. The Mann-Whitney U test was used to evaluate the statistical significance of differences in KSS. The other clinical and radiological evaluations were compared using paired t-tests. All data were analyzed using the R statistical software package. Data were compared by one-way analysis of variance, with p < 0.05 defined as statistically significant. ICCs were calculated with a two-way random model using SPSS (version 21.0 for Windows; IBM, Chicago, IL).
This work was conducted according to the guidelines as set forth by the ethics committee of the Japanese Red Cross Kyoto Daiichi Hospital (No. 1389). All patients gave informed consent prior to being included in this retrospective study performed in accordance with the Ethical Standards of the 1964 Declaration of Helsinki as revised in 2000.
Results
Clinical outcomes.

* < 0.05 vs pre TKA.
Radiographic evaluations.

Additional osteotomy of the distal femur.
Discussion
The most important finding of this study is that the BCS-type TKA is more useful for improving flexion contractures than the PS-type TKA since the femoral component is positioned anteriorly in the extended knee position.
Residual flexion contracture after TKA results in decreased patient satisfaction and reduced ability to walk.1,2 Preoperative flexion contracture is a risk factor for residual flexion contracture after TKA. Ritter et al. 1 reported that preoperative flexion contractures of 6° or more were 2.9 times more likely to cause postoperative flexion contractures, and preoperative flexion contractures of 20° or more were 5.8 times more likely to occur. Even if a fully extended position is achieved intraoperatively, postoperative flexion contracture is thought to occur after TKA because of preoperative posterior soft tissue contracture and decreased extensibility, 3 and Berend et al. 15 reported that flexion contracture remained in 33% of patients after TKA for knees with flexion contracture of more than 20°. In the present study, we investigated the outcomes of BCS-type or PS-type TKA for flexion-contracted knees with preoperative flexion contracture of 15° or more, and found that both groups had residual flexion contracture in some cases, but that the postoperative extension angle of the BCS group was significantly lower than that of the PS group, with more cases gaining full extension and fewer cases with residual flexion contracture of 15° or more. Since there was no difference in KSS scores between the two groups, we considered the BCS-type TKA to be more useful than the PS-type TKA in obtaining the desired postoperative extension position, although the BCS-type TKA has no advantage in knee joint function and pain in this study. Ritter et al. 1 reported that residual moderate flexion contractures of 6° or more and severe flexion contractures of 20° or more had significantly worse postoperative outcomes than flexion contractures of 5° or less, as assessed by objective measures. Koh IJ et al. compared flexion contractures after TKA above and below −10° using a patient-oriented evaluation and found the postoperative flexion contracture does not increase pain, but may be detrimental to quality of life. 16 In contrast, in this study, the degree and difference in flexion contracture between the two groups was only −5.5 and −2.8° compared to these reports, and it is also possible that significant differences were not obtained because the evaluation was objective, such as the KSS. We considered it necessary to conduct a patient-oriented evaluation in the future. In order to improve severe flexion contracture postoperatively, medial soft tissue release, osteophyte removal, soft tissue release from the posterior joint capsule, and additional resection of the distal femoral condyle should be performed sequentially to obtain full extension intraoperatively. 14 Continuous periosteal release from the posterior glenoid and intercondylar area can provide an average extension gap of 1.7 mm on the medial side and 2.3 mm on the lateral side. 17 provement of flexion contracture by distal femoral osteotomy is 10° (goniometer) and 5° (navigation) for every additional 2 mm, 18 but the amount of osteotomy is limited due to the elevated joint line and instability induced in the mid-flexion position. 19 Constrained implant is necessary when the gap balance is poor for both soft tissue processing and distal femoral additional osteotomy. 14 In this study, even though all patients in both the PS and BCS groups were treated up to the soft tissue release of the posterior joint capsule, an osteotomy of the distal femur was performed in both groups since there were cases of insufficient extension gap after trial implant placement. The amount of distal femoral osteotomy in this study was significantly less in the BCS group than in the PS group, suggesting that a BCS-type TKA would better facilitate the acquisition of an extension gap by reducing the amount of distal femoral osteotomy performed. We also thought that it might be possible to reduce the use of constrained implants.
Mitsuyasu et al. 5 stated that a large protrusion of the femoral posterior condyle increases posterior soft tissue tension, reducing the extension gap, and inducing the need for an additional distal femoral osteotomy. Onodera et al. defined the posterior offset ratio as the ratio of the posterior condyle of the femoral component protruding from the posterior margin of the tibial component to the anteroposterior diameter of the proximal tibia in knee extension on true lateral radiographs. The results showed an average of 5.63% for normal knees (Japanese) while the average for the five PS-type implants was 19.2%. The knees after PS-type TKA were reported to have significantly greater posterior femoral protrusion compared to normal knees, and are at risk of the development of postoperative flexion contractures. 6 Leie MA et al. reported that in knees with preoperative flexion contractures of 5° or greater, the selection of a cruciate retaining implant with a posterior condyle that is 2 mm thinner than the osteotomy of the posterior condyle, corrected intraoperative flexion contractures by an average of 3.5°, and that the posterior femoral protrusion is an independent variable in securing the extension gap. 19 On the other hand, unlike PS-type, BCS-type TKAs have an anterior cam as well as a posterior cam. Therefore, the anterior-posterior relationship between femur and tibia in BCS-type TKA approximates that of a normal knee (Figure 1). Tomite et al. 21 compared the posterior offset ratio of BCS-type and PS-type TKAs in the extended knee position in 30 cases respectively, and reported that the anterior-posterior positioning of the femur and tibia was close to that of a normal knee. Even though the present study showed the smaller posterior offset ratio of the BCS group and no change in PCO between the two groups pre- and postoperatively, the postoperative flexion contracture was less in the BCS group. This indicated that the amount of protrusion of the posterior femoral condyle from the posterior margin of the tibial component was smaller in the BCS-type TKA in the extended knee position than in the PS-type TKA in the present study (Figure 3), which may have affected the ability to obtain an appropriate extension gap.
Limitations of the study are as follows: non-randomized prospective study, the use of TKA implants varies with the time of surgery, the follow-up period and patient-oriented evaluation were not performed. The time of surgery and follow-up period in the two groups was quite different, and this might influence the results in this study. The osteotomy in this study was performed using a conventional method, which is less accurate than osteotomies using navigation systems or robotic-assisted systems.
Conclusion
There was no significant difference in KSS between the two groups, but postoperative flexion contracture was significantly improved in the BCS group. The BCS-type TKA was effective for improving preoperative flexion contracture with a smaller distal femoral osteotomy since the presence of the anterior cam reduced the protrusion of the posterior femoral implant in the extended knee position compared to the PS-type TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.