
Abstract
Purpose:
Tranexamic acid (TXA) is a commonly used compound that reduces postoperative blood loss. Periarticular injection of TXA is a recently reported procedure with some advantages such as cost-effectiveness and the ease of performance over an intravenous or topical administration. However, its association with functional recovery remains unclear. This study aimed to examine the effect of periarticular injection of TXA on early postoperative recovery of knee functionality after total knee arthroplasty (TKA).
Methods:
Eighty-four patients who underwent primary unilateral TKA from February 2013 to August 2016 were classified into two groups based on whether they received TXA injection (44 cases each in the TXA and control groups). Patients in the TXA group received periarticular injection of TXA (1000 mg) just prior to incision closure. Ten-meter walk test (s), pain visual analog scale, knee extension muscle force (N), range of motion (ROM) (maximum flexion angle, maximum extension angle, and motion arc), and blood loss (mL) were assessed.
Results:
The maximum flexion angle and maximal extension angle on postoperative day (POD) 4, POD7, POD10, and POD14 in the TXA group were significantly larger than those in the control group. The postoperative drained blood in the TXA group was significantly less than that of the control group (543.9 ± 464.3 mL and 814.9 ± 481.4 mL, respectively, p < 0.05). No significant difference was observed in the other parameters at any time point.
Conclusion:
Periarticular injection of TXA significantly promotes early recovery of knee ROM after TKA.
Introduction
Total knee arthroplasty (TKA) can effectively relieve pain, restore knee function, and improve the quality of life of patients with end-stage knee osteoarthritis. 1,2 The quality of rehabilitation early after TKA is closely tied to recovery of range of knee motion, pain, and muscle strength. Many patients experience unpleasant limited range of motion (ROM), muscle weakness as well as pain in the early postoperative period, which usually hinders early rehabilitation and reduces satisfaction. 3 –5 As the incidence of TKA increases in this era of value-based care and bundled payments, improving early outcomes has become an important. 6 However, there have been only limited measures improving range of knee motion, muscle strength, and pain for early functional recovery (e.g. early enhanced rehabilitation and pain control using multimodal analgesia). 7,8
Tranexamic acid (TXA) is often used as one of the countermeasures for postoperative blood loss, and many systematic reviews have demonstrated that intravenous, oral, and topical TXA use during TKA significantly reduced blood loss. 9 –16 There is also consensus that TXA does not increase the risk of deep vein thrombosis and pulmonary embolism because hemostatic control can be obtained without any adverse effects on coagulation. 17 –19
Periarticular injection of TXA is a recently reported procedure with some advantages such as cost-effectiveness and the ease of performance over an intravenous or topical administration. 20 It can effectively reduce blood loss and soft tissue swelling, which may consequently affect recovery of knee function after TKA. However, there is little information regarding the association between periarticular injection of TXA and functional recovery after TKA. The aim of this study was to examine our hypothesis that periarticular injection of TXA promotes early recovery of the range of knee motion.
Patient and methods
Patient selection
Data were prospectively collected from 116 consecutive patients who underwent TKA in our hospital. Eighty-eight consecutive primary unilateral TKAs were included in this study. Bilateral TKAs (n = 12) and revision TKAs (n = 16) performed during the study period were excluded (Figure 1). TXA was not used in the first 44 cases (control group) treated between February 2013 and March 2015 and was used in the latter 44 cases (TXA group) treated between April 2015 and August 2016. All surgical procedures were performed by two surgeons. All patients included in this study provided informed consent for the use of their medical information, and this study was approved by the Institutional Review Board of our university. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.

Flow diagram showing the inclusion and exclusion criteria for total knee arthroplasty.
Surgical procedure and periarticular injection of TXA
The knee joint was exposed via a medial parapatellar approach. The prosthesis was fixed with cement and the patella was resurfaced. The tourniquet was inflated during bone cut and cement fixation of the prosthesis, and the tourniquet was not deflated before skin closure. The prosthesis used was the posterior stabilized Vanguard Complete Knee system (Zimmer Biomet, Warsaw, Indiana, USA) in 52 cases and the JOURNEY Ⅱ Bi-Cruciate Stabilized Total Knee System (Smith & Nephew, Inc, Memphis, Tennessee, USA) in 36 cases. In the TXA group, 40 mL of 0.25% ropivacaine with 1:2000,000 epinephrine containing 1000 mg TXA (25 mg/mL of TXA) was injected into the area around the medial and lateral capsule, the quadriceps muscle tendon, and the infrapatellar fat pad just prior to incision closure; 40 mL of 0.25% ropivacaine with 1:200,000 epinephrine without TXA was used in the control group.
All patients received the same rehabilitation program. On the third postoperative day, patients began active ROM exercises and full weight-bearing walking with the use of a walker or rails. For postoperative pain control, patients received oral celecoxib at a dose of 200 mg/day for 1 week.
Assessment of blood loss and functional recovery of the knee
Perioperative blood loss (mL) was estimated by using the Gross formula based on hemoglobin and hematocrit value, 21 and 10-m walk test (s), pain visual analog scale (pain VAS, the minimum 0 to the maximum 100), knee extension muscle force (N), and maximum active flexion and active extension angles, and ROM arc assessed at postoperative days (POD) 4, 7, 10, and 14. Knee extension strength was measured using ISO force GT300 (OG GIKEN, Okayama, Japan) according to the previously validated method. 22 Ten-meter walk test was performed according to the previously validated method. 23 Ten-meter walk test and knee extension strength were shown as absolute values and recovery ratio compared with preoperative value: a recovery ratio = postoperative value/preoperative value.
Statistical analysis
The t-test was used for comparison of parameters between TXA and control groups. Tests for normality and distribution were performed using the Kolmogorov–Smirnov test. Student’s t-test was used to analyze parametric data. A post hoc power analysis was conducted using G*Power software (version 3.0.3) to compare the groups. A post hoc power analysis (effect size, 0.5) revealed that the comparison of the groups had a statistical power of 0.75. The threshold for significance was set at p < 0.05 for all analyses.
Results
Demographic data of the patients are summarized in Table 1. There was no significant difference in the mean age, gender, and body mass index between groups, while average operation time was significantly longer in the TXA group than in the control group. The estimated blood loss by either hemoglobin or hematocrit value in the TXA group was significantly lower than that in the control group (p < 0.001 and <0.01, respectively) (Table 2). Both maximum flexion angle and maximum extension angle at each time point (POD 4, 7, 10, and 14) were significantly larger in the TXA group than in the control group (Table 3; Figure 2(a) and (b)). There was no significant difference in pain VAS, 10-m walk test, recovery ratio, and absolute value of knee extension strength or recovery ratio and absolute value of 10-m walk test at any time point (Tables 4 –6; Figure 2(c) to (f)). There were no adverse events such as infection in all the cases in the study period. All patients functionally recovered to do daily living independently and discharged from the hospital within 3 weeks after surgery.
Demographic data of the patients.

TXA: tranexamic acid; BMI: body mass index; CTL: control.
Estimated blood loss (mL) by hemoglobin and hematocrit.

CTL: control; TXA: tranexamic acid; Hb: hemoglobin; Hct: hematocrit.
Comparison of the maximum flexion and extension angles between the groups.

CTL: control; TXA: tranexamic acid; POD: postoperative day; n.s.: not significant.
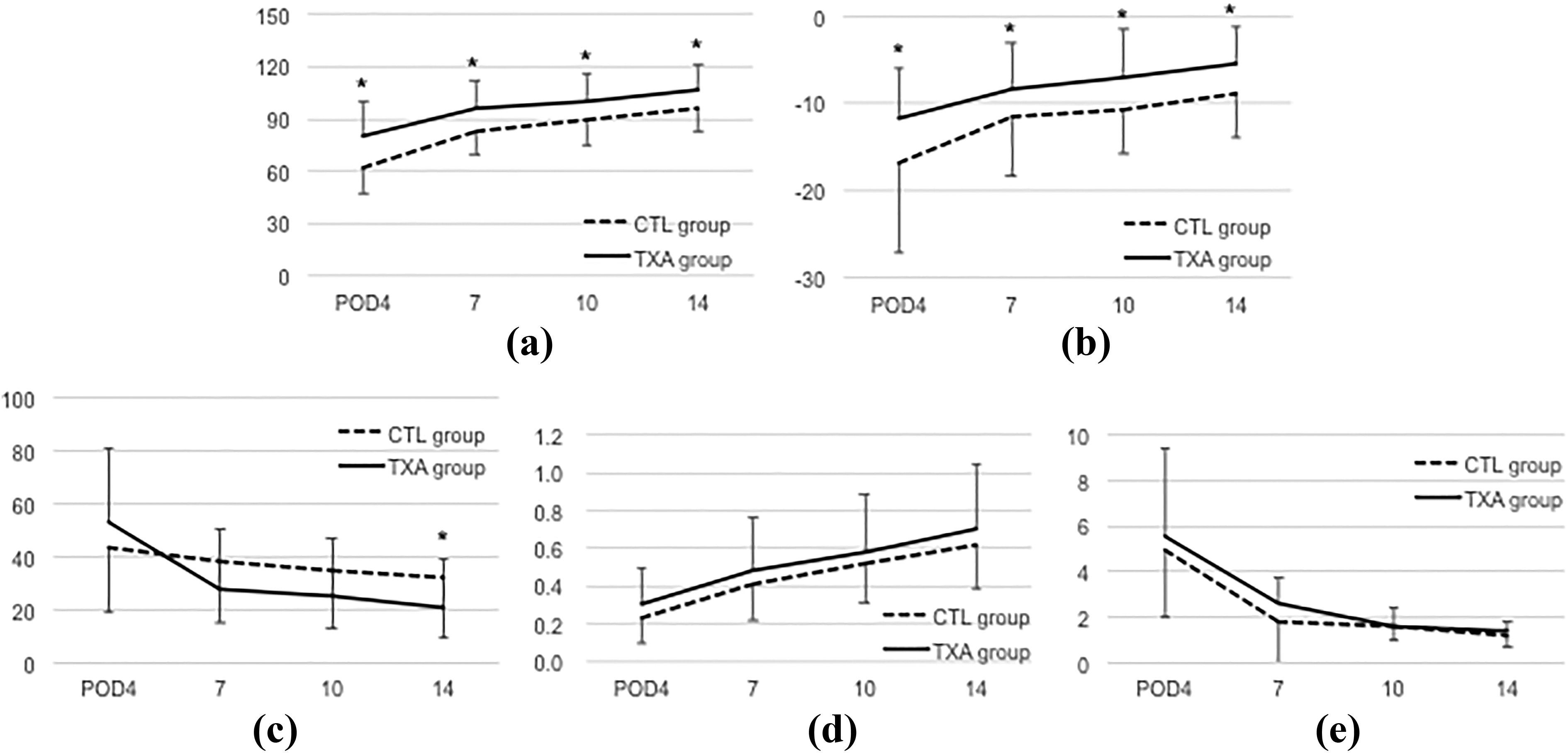
Comparison of each parameter between control and TXA groups. (a) Maximum flexion angle, (b) maximum extension angle, (c) pain VAS, (d) recovery ratio of knee extension strength, and (e) recovery ratio of 10-m walk test were compared between control and TXA groups. *p < 0.05 compared with the control group at the same evaluation point.
Comparison of pain VAS (mm) between the groups.

VAS: visual analog scale; POD: postoperative day; CTL: control; TXA: tranexamic acid; n.s.: not significant.
Comparison of the 10-m walking test (s) between the groups.
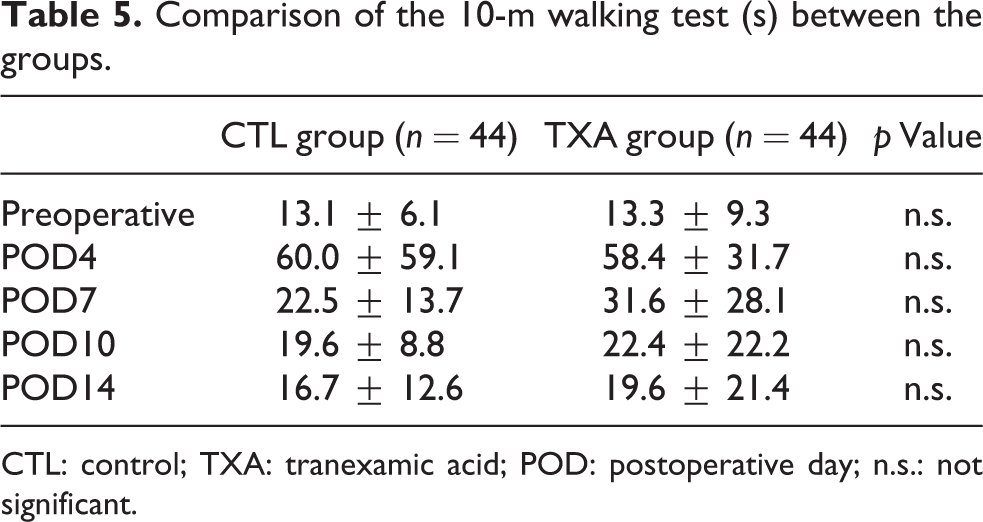
CTL: control; TXA: tranexamic acid; POD: postoperative day; n.s.: not significant.
Comparison of knee extension muscle force (Newton) between the groups.

CTL: control; TXA: tranexamic acid; POD: postoperative day; n.s.: not significant.
Discussion
The most important finding of this study was that periarticular injection of TXA during the surgery induces early recovery of knee ROM after TKA in addition to a hemostatic effect.
Yozawa et al. reported that periarticular injection of TXA is effective to reduce postoperative blood loss, and that this effect is comparable to intra-articular injection or intravenous administration in spite of relatively small dose of TXA (1000 mg). 10,20 In addition, in this study, although there were no significant differences in recovery in 10-m walk test, pain VAS, and knee extension muscle force, this periarticular injection displayed a significant effect on early recovery of the range of knee motion though there has been limited evidence that intervention other than physical rehabilitation could promote early functional recovery of the range of knee motion after surgery. There have a few reports regarding the beneficial effect of TXA on the recovery of knee function. Serrano Mateo et al. reported that topical administration of 3000 mg of TXA significantly promoted early functional recovery in 6-weeks follow-up. 24 Dorweiler et al. reported that intravenous and topical administration of more than 2000 mg of TXA improved early postoperative ROM. 25 A periarticular injection of TXA has some advantage over an intravenous or topical administration. For example, a periarticular injection does not principally limit the use of drainage as temporally drainage clamping. A periarticular injection was advantageous to effectively administer TXA around the knee with a relatively small amount of 1000 mg of TXA, which may result in less cost and complications. Also, it is easy to perform because 1 g TXA can be contained in analgesics cocktail injection for multimodal pain management.
Additional factors which affect restoration of knee ROM after TKA include pain, swelling, implant placement, and early rehabilitation, 26 –29 but little is known about the relationship between periarticular injection of TXA and functional recovery of the knee after TKA. Ishida et al. 10 found that intra-articular injection of TXA (2000 mg) reduces not only blood loss but also knee joint swelling after TKA. However, the authors did not demonstrate that intra-articular injection of TXA promotes significant functional recovery of the knee. 10 On the other hand, in the current study, it was found that periarticular injection of TXA (1000 mg) promoted recovery of the range of knee motion significantly earlier compared with cases without TXA. This discrepancy may be due to the difference in the mode of administration of TXA, namely intra-articular injection versus periarticular injection. TXA may remain locally around the knee in periarticular injection longer than in intra-articular injection to effectively reduce swelling and edema of the soft tissue around the knee, as evidenced by the fact that the effect of reduction in blood loss is comparative between periarticular injection of 1000 mg of TXA and intra-articular injection of 2000 mg of TXA. 10,20 Although there was a significant difference in operation time between the groups, there was no statistical significant correlation between operation time and the ROM (the maximum flexion and extension, data not shown), which imply that shorter operation time in the TXA group did not induce better recovery of the ROM. Although previous several studies have examined the effect of systemic versus intra-articular injection of TXA, few studies have investigated the effect of periarticular injection of TXA in TKA. A randomized controlled study comparing different routes of TXA administration, including periarticular injection, on postoperative functional recovery is warranted to validate the current results.
There were some limitations in the current study. First, postoperative swelling and edema around the knee were not evaluated, so direct evidence about the effect of periarticular injection of TXA on these complications remains unclear. Further studies evaluating the effect of periarticular injection of TXA on postoperative swelling and recovery of postoperative range of knee motion are warranted. Second, this was a retrospective, nonrandomized study, two kinds of implants used, and data for the two groups were collected at different times. This limitation may involve a bias in surgical techniques. However, the surgeons who participated in this study were well-experienced, senior specialists skilled in performing TKA, and surgical technique was consistent throughout the study period with the exception of TXA administration. In the future, a randomized controlled trial to examine which administrative route is more effective to reduce blood loss and promote early functional recovery after TKA should be conducted.
Conclusion
Periarticular injection of TXA achieved early recovery of the range of knee motion after TKA in addition to a hemostatic effect.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.