
Abstract
The majority of hip fractures in elderly patients are managed surgically with superior outcomes. However, for patients who refuse surgery or are deemed medically unfit, traction used to be the mainstay of nonsurgical treatment, which is associated with prolonged hospitalization and inpatient complications from immobility. This study, therefore, aims to evaluate the outcomes of an early wheelchair mobilization protocol as an alternative nonsurgical treatment option. This is a retrospective study of 87 elderly patients who were managed nonsurgically for their hip fractures over a 1-year period. The accelerated rehabilitation protocol did not have them on traction but were instead mobilized with assistance as soon as possible after admission. Variables collected electronically include patient demographics, fracture characteristics, inpatient mobilization milestones, inpatient complications, Modified Functional Ambulation Classification (MFAC), Modified Barthel Index (MBI) scores, and radiological findings. Patients who were younger, could sit up earlier and had a shorter length of stay, were able to ambulate better at 6 months (p value < 0.05). Patients with femoral neck fractures and shorter length of stay had better MFAC scores. A total of 58% of patients with radiological follow-up had displacement of their fractures with age, type of fracture, and length of stay as predictors (p value < 0.05) The Charlson’s score, day to sitting up, and day to transfer affect fracture healing (p value < 0.05). The mean length of stay was 17 days and the 1-year mortality was 18%. Surgical therapy remains the preferred choice of management for patients with hip fractures. Early wheelchair mobilization leads to a shorter length of stay compared to traditional traction methods and comparable 1-year mortality rates with operative management. Despite this, complication rates remain high and only 48% of patients achieved ambulation by 1 year, with healing in only 24% of fractures.
Background
The majority of hip fractures in elderly patients are managed surgically with superior outcomes. However, for patients who refuse surgery or are deemed medically unfit, traction used to be the mainstay of nonsurgical treatment. Due to local culture and lower educational status, the majority of elderly are also averse to surgery. Traction required prolonged hospitalization and could lead to many inpatient complications associated with immobility. We have developed an early mobilization protocol for our nonsurgical patients to avoid the problems with traction.
Objective
This study, therefore, aims to evaluate the outcomes of an early wheelchair mobilization protocol as an alternative nonsurgical treatment option by looking at both functional and radiological outcomes.
Methodology
This is a retrospective study of 87 elderly patients who were managed nonsurgically for their hip fractures (femoral neck and intertrochanteric fractures) over a 1-year period (October 2011 to October 2012). We excluded patients below the age of 65, with previous hip fractures and/or concomitant fractures and with pathological fractures.
The study was conducted in a tertiary level 1 trauma center with an established ortho-geriatric care-path for hip fracture patients. Our implementation of an accelerated rehabilitation protocol with early wheelchair mobilization is part of a multidisciplinary ortho-geriatric care where coordinators are employed to follow up with patients and family, and the data are collected prospectively for storage within a hip fracture registry.
We reviewed the electronic medical records of all elderly patients admitted for hip fractures and collected the patient demographics, Charlson’s comorbidities score, fracture characteristics, days needed to achieve the mobilization milestones as previously mentioned, and outcome measures; both functional scores such as Modified Functional Ambulation Classification (MFAC) and Modified Barthel Index (MBI) scores collected at 6 and 12 months post-discharge through telephone interviews conducted by our nurse clinicians.
Radiological findings on clinic follow-ups post-discharge were collected through electronic records. Nonunion was defined as radiological evidence of nonprogression of healing between two radiographs taken after 6 months. The radiographs were read manually by the senior author for subjective assessment of displacement. Standard anterior–posterior and lateral radiographs of the affected hip were performed during the patient’s scheduled follow-up visits according to a standardized protocol.
Ethical approval was obtained before the study is carried out.
The Charlson’s comorbidity index 1 predicts the mortality for a patient who may have a range of 22 comorbid conditions, such as heart disease, lung disease, or cancer. Each condition is assigned a score and scores are summed to provide a total score to predict mortality.
MFAC 2 is an instrument for categorizing gait ability. There are six categories, one and two being non-walkers, while three to six ranges from dependent walker to outdoor walker. The MFAC does not take into account walking aids.
MBI 3 is a measure of activities of daily living, which shows the degree of independence of a patient from any assistance. It covers 10 domains of functioning, and total scores may range from 0 to 100.
Patients who did not undergo surgery were placed on a nonsurgical hip fracture pathway and comanaged by both orthopedic and geriatric physicians. The accelerated rehabilitation protocol did not have them on traction, but were instead mobilized with assistance as soon as possible after admission. This was achieved with the help of physiotherapists and occupational therapists and mobilization milestones consist of bed mobilization initially, sitting up in bed, bed to chair transfer, and eventually wheelchair mobilization. These were performed as tolerated, up to 1 person moderate assistance, with adequate pain relief through oral and local analgesia in the form of nerve blocks or intra-articular steroid injections.
Statistical analysis was performed using IBM SPSS 19 software. Univariate analysis using paired t-test and McNemar’s test was performed with a p < 0.05 taken as level of significance. Data for continuous variables were reported as mean, range, and 95% confidence intervals.
Results
There were 110 elderly patients who were nonsurgically managed for their hip fractures over the study period (October 2011–October 2012). This was out of a total of 556 consecutive patients who were admitted for hip fractures in the study period. Twenty-three cases were excluded (two patients had incomplete inpatient case notes, five patients had insufficient data scores from follow-up, three patients had insufficient radiological follow-up, four patients transferred to another hospital while inpatient, two patients had bilateral hip fractures, four patients had previous hip fractures, one patient had pathological hip fracture, and two patients were below age of 65). A total of 87 cases were used for analysis.
Table 1 shows the patient characteristics of our study population. Of the 87 patients, 62 patients declined surgery despite counselling and 25 patients had complex medical issues with a high surgical risk. The mean age was 84 ± 1.89 years with a high Charlson’s comorbidity score of 6 ± 0.38. At a score of 6, the 10-year survival is 2.3%. 1 The average length of stay inpatient was 17 ± 3.98 days. There were no correlations between greater number of comorbidities (Charlson’s score) and length of inpatient stay.
Patient demographics and mobility milestones.
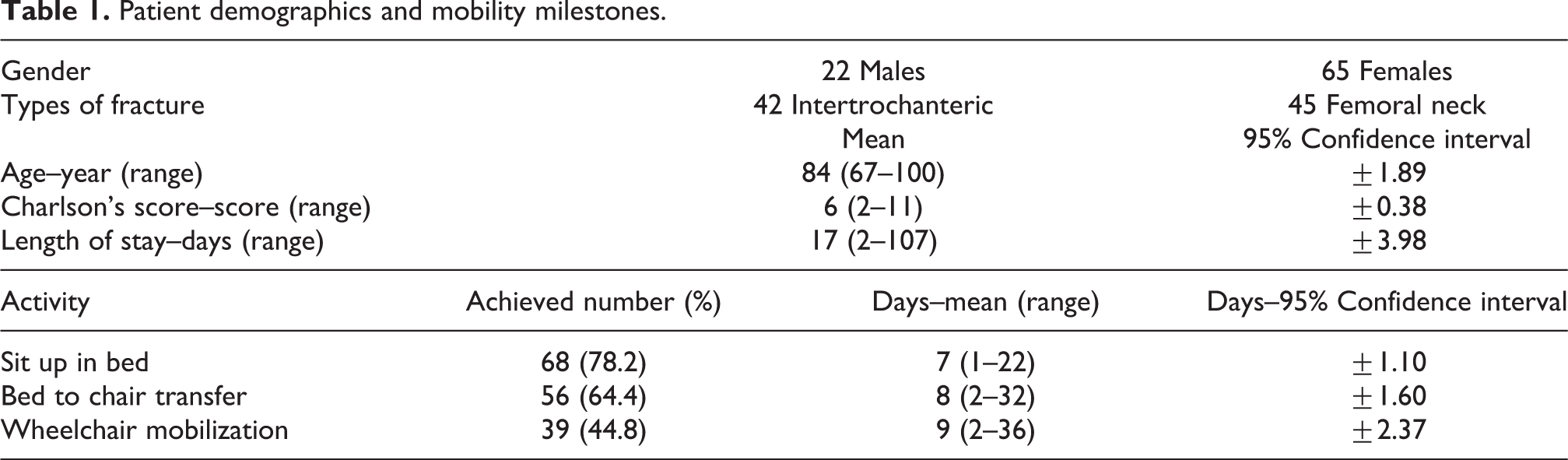
Close to half, 44.8% of the patients were able to achieve wheelchair mobilization by the end of their stay; 22.8% of patients remained unable to tolerate even sitting up in bed and remained bedbound during the inpatient stay. Sixty-three patients (72.4%) had persistent pain despite oral analgesia and required intra-articular steroid injections or peripheral nerve blocks. The physical therapy consists of stand and transfer protocols with wheelchair mobilization. Table 1 also shows the mobility milestones and number of days our patients took to achieve them.
There was a statistically significant increase in mean MBI score from discharge to 6 months (p value < 0.01), translating to a functional improvement in our patients at 6 months. There was no significant improvement between 6 months and 12 months. There was also a statistically significant difference in the proportion of walkers at admission and 6 months (p value < 0.01). At 6 months, 39% of previous walkers were able to walk. At 12 months, 48% of previous walkers were able to walk and 28 patients (32%) were ambulating on nonunited fractures.
We have identified factors contributing to ambulating after 6 months, as shown in Table 2. Younger age (p value = 0.02), shorter days to sitting up in bed (p value = 0.01), and a shorter length of stay (p value = 0.01) played a role in allowing patients to ambulate after a 6-month period. At 12 months, only younger age (p value = 0.02) remained a significant factor in ambulation of the patients. We did not find any correlation between fracture stability (p = 0.41) or fracture healing (p = 0.44) with the ability to return to mobility.
Factors contributing to mobility at 6 months.
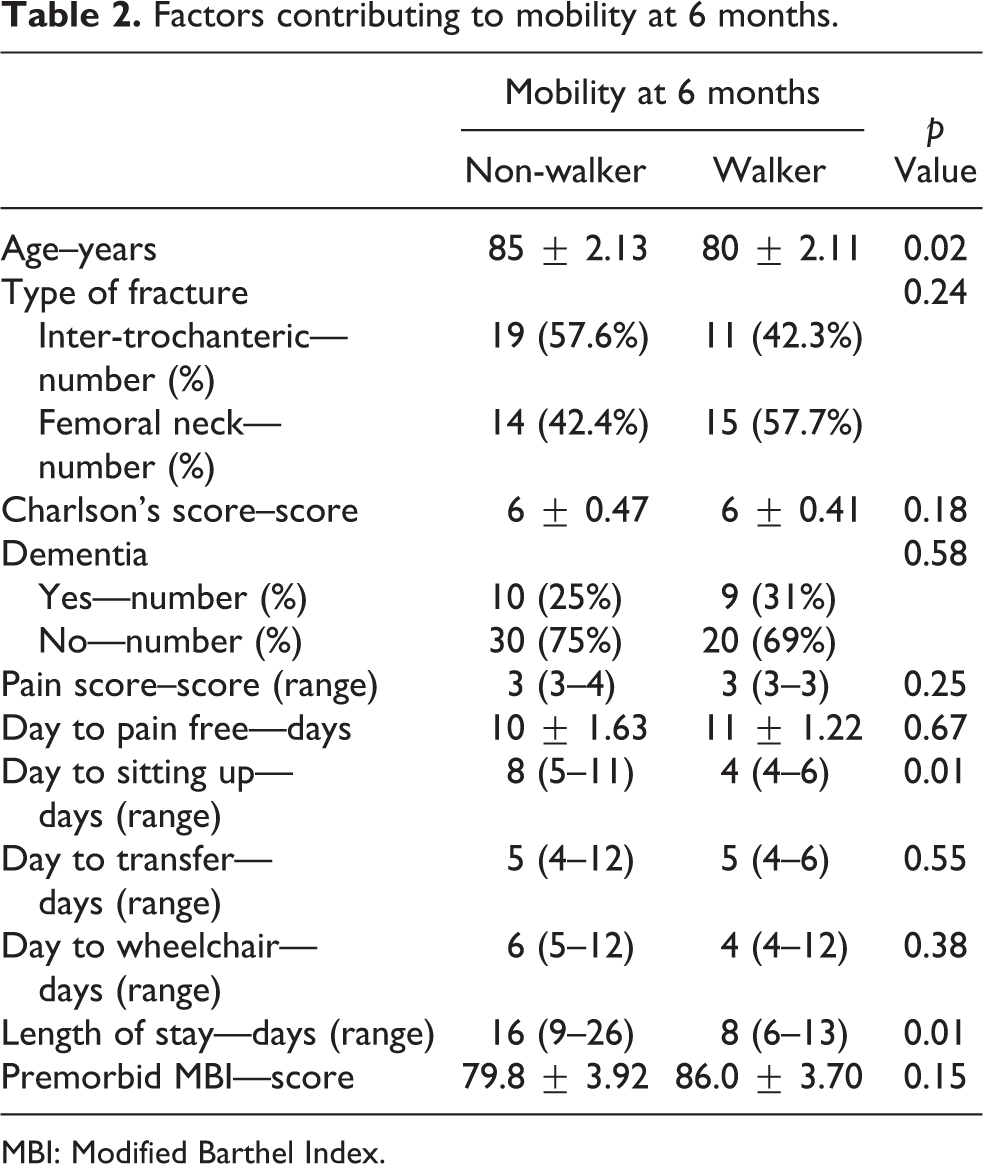
MBI: Modified Barthel Index.
Table 3 shows the factors contributing to higher MFAC scores at 6 months’ follow-up. Younger age (p value = 0.02), sustaining femoral neck fracture (p value = 0.03), and a shorter length of stay (p value = 0.04) led to patients having better MFAC scores at 6 months. At 12 months, only younger age (p value = 0.04) was a significant factor in having higher MFAC scores.
Factors contributing to improvement in MFAC scores at 6 months.

MFAC: Modified Functional Ambulation Classification; MBI: Modified Barthel Index.
Fifty-eight percentage of patients with radiological follow-up had displacement of their fractures. Table 4 shows the factors contributing to fracture displacement: older age (p value = 0.03) and a longer length of stay (p value = 0.02), and patients with a mean length of stay of 16 days had higher rates of fracture displacement than patients who stayed a mean of 9 days. Inter-trochanteric fractures (p value < 0.01) tend to displace more than femoral neck fractures, with 75% of inter-trochanteric fractures displacing compared to 38.7% of femoral neck fractures.
Factors contributing to fracture displacement.

MBI: Modified Barthel Index.
Only 24% of fractures eventually healed on radiological follow-up. Table 5 shows the factors contributing to fracture healing. Having a lower Charlson’s score (p value < 0.01), shorter days to sitting up (p value = 0.03), and shorter days to transfer (p value = 0.04) led to better healing of the fractures.
Factors contributing to fracture healing.
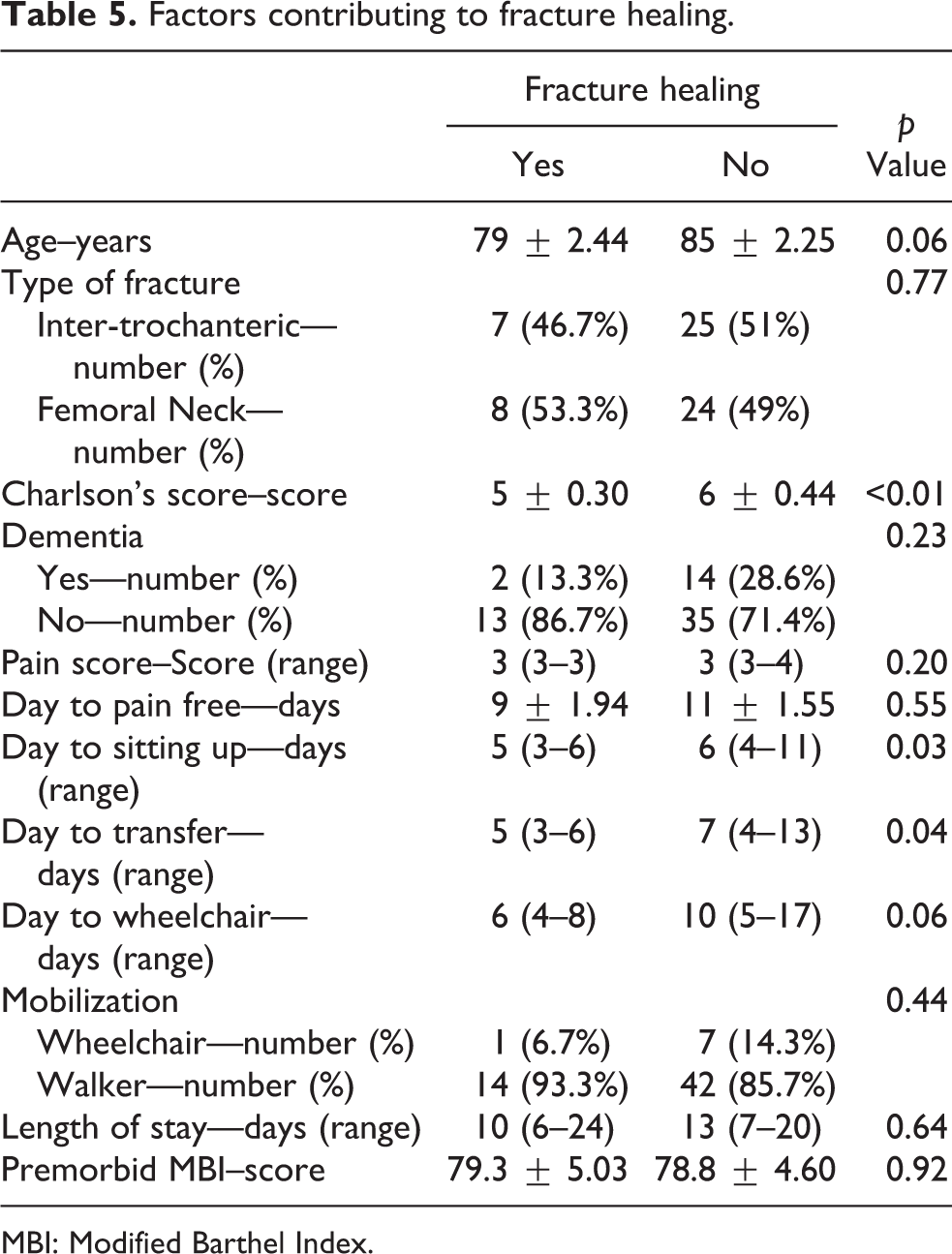
MBI: Modified Barthel Index.
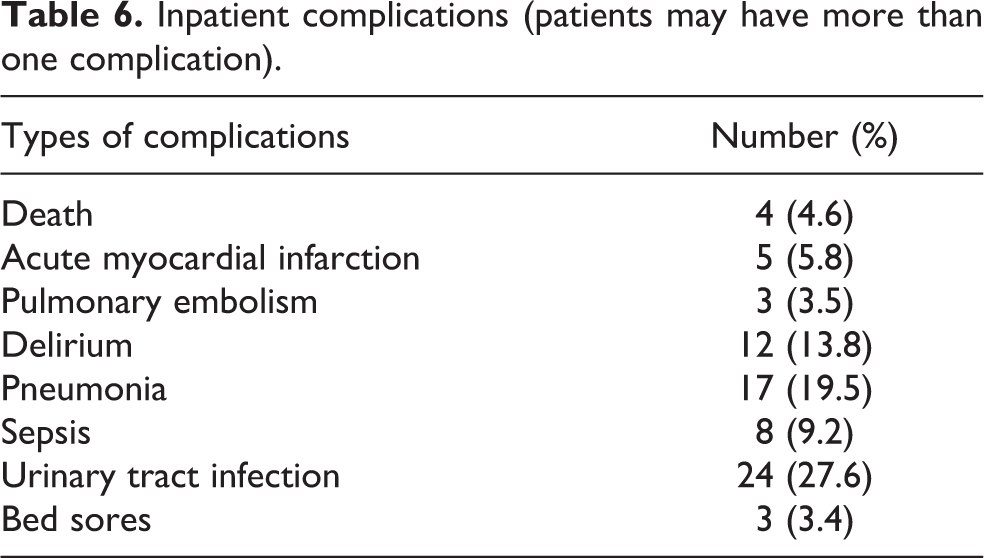
Our inpatient complication rates are shown in Table 6; 59% of our patients had at least one complication while inpatient, with four deaths (one due to acute myocardial infarction, one due to pulmonary embolism, and two due to pneumonia). Twenty-seven of 48 (56.3%) patients who did not achieve wheelchair mobilization developed inpatient complications, comparable to 24 of 39 (61.5%) patients who achieved wheelchair mobilization.
Inpatient complications (patients may have more than one complication).
Discussion
Many studies have shown that surgical management still leads to the best outcomes in patients with hip fractures, 4,5 with some studies showing non-inferiority of nonsurgical management as compared to surgery in low-grade fractures. 6,7 At our center, while surgery remains the mainstay of treatment for hip fracture patients, there remain a significant number of patients who are unsuitable for surgery due to multiple high-risk comorbidities. 8,9 There are also some patients or families who refuse surgery because of their fear of surgery or surgical risks, which may be attribute to local culture and the lower educational status of elderly patients.
This study was conducted in a rapidly developing Asian First World country. Recent progress in hip fracture care is contrasted against a backdrop of poorly educated aging population with their own cultural values and beliefs. A significant proportion of our patient cohort refused the surgical option despite counselling and optimization for surgery. We can only respect their patient autonomy in making that choice.
Age alone has been shown to be a poor prognostic factor for walking ability at discharge and survival, regardless of whether they underwent surgical or nonsurgical treatment. 10 In our cohort, older age and longer length of stay are the two main factors that affect both functional and radiological outcomes. We proposed that this can be explained by decreased musculature and strength required for ambulation due to a more advanced age and further deconditioning as an inpatient and not contributed by comorbidities and dementia as expected. It is shown that the Charlson’s comorbidity score only affected fracture healing and not ambulation status or MFAC scores. However, the use of Charlson’s score may limit our study as it is mainly used as a prognostication tool, and not all of the 22 conditions covered affect ambulation directly.
We also looked at dementia but did not find that it predicted for poorer outcomes. This is an unexpected finding as dementia has been shown to affect nutrition, wound care, and behavioral problems. These translate to further deconditioning from malnutrition and immobility, decreased participation in therapies, and a higher risk of developing inpatient complications like urinary tract infections due to urinary retention or aspiration pneumonia due to dysphagia. These may have been improved and prevented with a comprehensive ortho-geriatric pathway that covers a wide spectrum of patient care, as is the case in our center. However, we acknowledge that the study is limited by a small sample size and encourage future studies to look into how dementia can affect rehabilitation and mobilization.
Early mobilization for nonsurgically treated hip fracture patients is not new; it has been described as early as in the 1960s by Crawford, 11 and subsequently by Kanaujia and Alam, 12 both showing favorable results of early mobilization as compared to confining patients to bedbound status. Hansen and Solgaard 13 in the late 1970s have found in patients with subcapital and mid-cervical femoral fractures who are able to raise their straight leg in the supine position within the first 2 days of admission; around 80% will heal without further displacement.
In our study, patients who had better ambulation and radiological outcomes managed to achieve the three ambulation milestones earlier on during their stay, despite having similar pain scores and longer days to being pain free. The longer duration it took for them to be pain free could have been contributed from the therapy sessions and more ambulation. We recommend titrating the oral analgesia to a suitable level or the use of peripheral nerve blocks to achieve adequate participation in therapy sessions.
In the Asian context, Tanaka et al. 14 have shown union rates of up to 61% and Ohsawa et al. 15 managed to walk 12 of 13 patients. In our study, the patients were frailer, had poorer preambulatory status, and had poorer outcomes. We also included all grades of femoral neck and inter-trochanteric fractures in our study, whereas Tanaka et al. only included Garden stage 1 femoral neck fractures.
One-year mortality among the patients included in the study was 18% and 1-month mortality was 6.8%. This is comparable to that of surgery at the same centre, which was 14.6 and 7.3%, respectively, in a study by Kau and Kwek. 16 Moulton et al. agrees that while 30-day mortality in the nonsurgical group is higher, patients who survived beyond 30 days had prevalence of mortality similar to those who underwent surgery. 17 We attribute the relatively low mortality rates to a low inpatient complication rates (especially nosocomial infections) due to a shorter length of stay despite many of these patients not achieving ambulation at any stage in their follow-up.
It is also been shown that longer length of stay contributes to more inpatient complications by Hauck and Zhao. 18 By comparing with historical reports of length of stay for patients on traction, 15,19 the length of stay with our method has been reduced from up to 6 weeks to 17 days. This will mainly result in fewer decubitus complications than traditional traction. However, in our study, the complication rates were comparable between the patients achieving wheelchair mobilization and the remaining patients. As our numbers were too small, we were unable to perform a subgroup analysis by specific complications.
We acknowledge the limitations of our study as those inherent in a retrospective design. We also recognize that our results are subject to institution-specific biases and may not be applicable in centers that do not share similar characteristics. We suggest future research to address the optimal regimen for nonsurgical treatment, balancing good outcomes with the morbidities and mortalities involved.
Conclusion
Surgical therapy remains the preferred choice of management for patients with hip fractures. However, early wheelchair mobilization for nonsurgically treated elderly hip fractures leads to a shorter length of stay compared to traditional traction methods and comparable 1-year mortality rates with operative management. Despite this, complication rates remain high and only 48% of patients were able to achieve ambulation by 1 year, with healing in only 24% of fractures. These results will allow us to appropriately counsel and advise patients more effectively.
Footnotes
Acknowledgment
The authors would like to thank Ms Sun Bing, Clinical Research and Innovation Office, Tan Tock Seng Hospital, for providing statistical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.