
Abstract
Elderly patients with hip fracture constitute Single Largest Group of Emergency Orthopaedics Admissions. In 2050, 6.26 million hip fractures worldwide, approximately 50%, will occur in Asia. Only small number of reports on incidence of hip fractures in the Asian population exist. India lacks data registry for fragility hip fractures, therefore, the magnitude and standard of patient care are not known. A prospective multicenter study was conducted from January 2012 to April 2014 to describe population-based longitudinal trends, namely, age-specific incidence, fracture type, timing of presentation, kilometers traveled, timing of surgery, hospital stay, man hours lost, pressure ulcers, weight bearing, 30-day return, 3-month mortality, and so on, of fragility hip fractures. A total of 1031 patients were included with 59.7% females and 40.3% of male patients, with a female–male ratio of 1.5:1. Commonest mode: Falls 45%. 56.4% IT fractures. 66.2%patients operated, Operative/Conservative Ratio of 2.8:1. Patients travel a mean distance of 86.4 kilometers for quality treatment. Of the patients, 85.9 % presented late due to ignorance and misguiding quack practice. Incidence of delayed surgery was 69.3%. Persistent electrolytes imbalance and hyperglycemia normalized in 81.2% by second or third postoperative day. The man hours lost was 157.85 hours/person. Medical complications was more (90%) in patients who had delays in surgeries and presentation. Mortality rate was 6.2 %. Patients travel long for quality treatment, most of them are misguided, present late with significant complications and sufferings, and their pockets half drained depriving them off best treatment. Early presentation and operation have better prognosis and rehabilitation, facilitates early return to work, and independence. Increased pressure sores, infections, hospital stay, treatment cost, depression, and mortality are directly related to delays in surgeries and presentation. Estimated losses according to lost man hours may go up to 10 million dollars.
Introduction
Elderly patients with hip fracture constitute the single largest group of emergency orthopedic admissions. 1 Hip fractures are common and serious, causing short-term pain and disability and leading to longer term pain and even deformity. 2,3 More than 10% of survivors are unable to return to their previous residence. Elderly individuals have multiple medical and psychological problems, hence there is an emerging need to pay greater attention to aging-related issues and promote holistic policies and programs for dealing with the aging society. 4
By 2050, total of 323 million people in India is expected to be 60 years and older, a number greater than the total US population in 2012. 5 By 2030, 45% of the health burden in India are expected to be older adults. 6 By 2050, there will be 6.26 million hip fractures worldwide of which approximately 50% will occur in Asia, but only a small number of reports exist on the incidence of hip fractures in the Asian population. 7 In today’s world, care and security of elderly individuals is a major concern. All leading countries have an established fragility hip fracture database, whereas India lacks a data registry for fragility hip fractures. Hence, the magnitude and standard of patient care for these patients in our country are not known, therefore treatment is not standardized, and there is a lack of universal treatment protocol. It is very well observed that elderly patients with hip fractures do not receive prompt and standard treatment and are often neglected due to the lack of a universal treatment protocol.
We conducted a prospective multicenter study from 2012 to 2014 in city of Bhubaneswar, Odisha, India. The aims of this study were to describe the population-based longitudinal trends of fragility hip fractures, organize valuable data into the fragility hip fracture database, measure the standards of elderly patient care, identify the loopholes, and standardize the treatment received by these patients in Bhubaneswar, India.
Material and Methods
We conducted a multicenter prospective observational study on registered patients visiting outdoor/casualty from January 2012 to April 2014 to examine the epidemiological profile of fragility hip fractures in the elderly population in the city and the causes of delay in patient’s presentation and delayed surgeries and its effects on prognosis in patients with fragility hip fractures. To maintain a fragility hip fracture registry, the National Hip Fracture Database (United Kingdom) and “Boa/Bgs blue book” were taken as standards and modified for Indian setup. Inclusion criteria are male or female patients aged >55 years, visiting outdoor or casualty with a diagnosis of hip fractures—fractured neck, intertrochanteric, or subtrochanteric femur—and any etiology, irrespective of the treatment provided. The following variables were assessed: age, gender, marital status, fracture pattern, mode of injury, timing of hospital presentation, average kilometers traveled, ASA grade and type of anesthesia, timing of surgeries, treatment provided, mean hospital stay, man hours lost to work, incidence of pressure ulcer, 30-day return to home, timing of weight bearing, mortality rate at 3 months, and falls assessment. A Hip Data Registry was setup in the parent institution from where the study was managed. Data and variables from various centers were collected and entered in the registry by the authors after thorough clinical examination. Patients were observed during their stay in the hospital and further follow ups, patients who refused treatment were followed by visits to their residence and telephonic conversations. Follow-ups and fall assessment were performed by orthopaedicians (AP,NP,RP, SKD). We tabulated data, calculated ratios using standard MS Office Tools (Microsoft Office Professional Plus 2010- Ms Word, Ms Powerpoint, and Ms Excel), and compared them with the published data. Standard deviation (SD), mean, and range were calculated for continuous variables.
Results
A total of 1031 patients were included in this study of which 616 (59.7%) were female and 415 (40.3%) male, with a female–male ratio of 1.5:1 and a wide range of age distribution (see Figure 1) from 56 to 94 years, and with a mean of 71 years and SD of 10. Females were affected more in the age-group of 70 to 79 years and males in the age-group of 60 to 69 years. At the time of hospital admission, 710 (68.8%) patients were married and 321 (31.2%) patients were widowed.
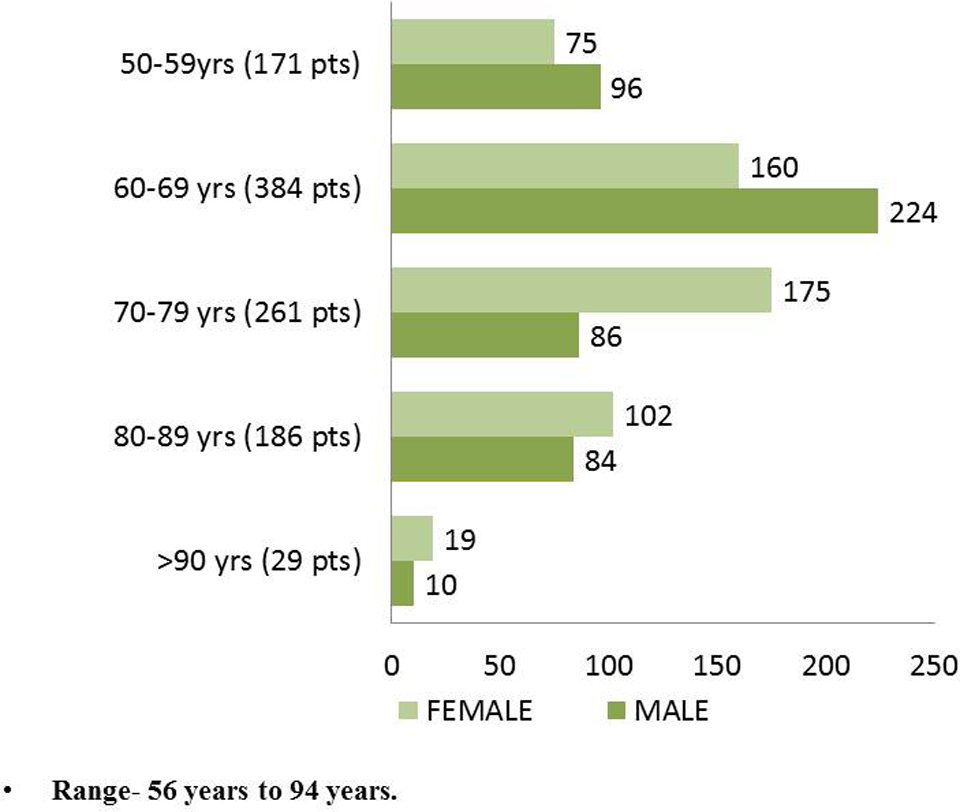
Age-specific incidence of hip fractures.
The commonest mode of injury was falls (45%; see Figure 2), followed by slipping while walking (36%) and others (19%) of which hit by a bull and falling in the drain constituted 5.3%. Fracture pattern was interesting with a maximum of 582 (56.4%) intertrochanteric fractures, 310 being right sided and 272 left sided, followed by 405 (39.2%) of femur neck fractures, 225 being left sided and 180 right sided. Of the 405 neck fractures, 195 fractures were subcapital, 112 were basocervical, and 98 were transcervical; 31 (3.0%) were subtrochanteric fractures, 20 being left sided and 11 being right sided. Of the 1031 patients, 712 (66.2%) patients were operated, 252 (25.9%) were managed conservatively with boot plaster and derotation bar, whereas 52 (5%) patients refused treatment with operative–conservative ratio of 2.8:1. A total of 767 (74.3%) patients were admitted for treatment, whereas 197 (19.1%) chose to be treated as an outpatient. More fractures (57.8%) were seen in summer months (Figures 3 and 4).

Mode of injury.

Type of fractures in 1031 patients.
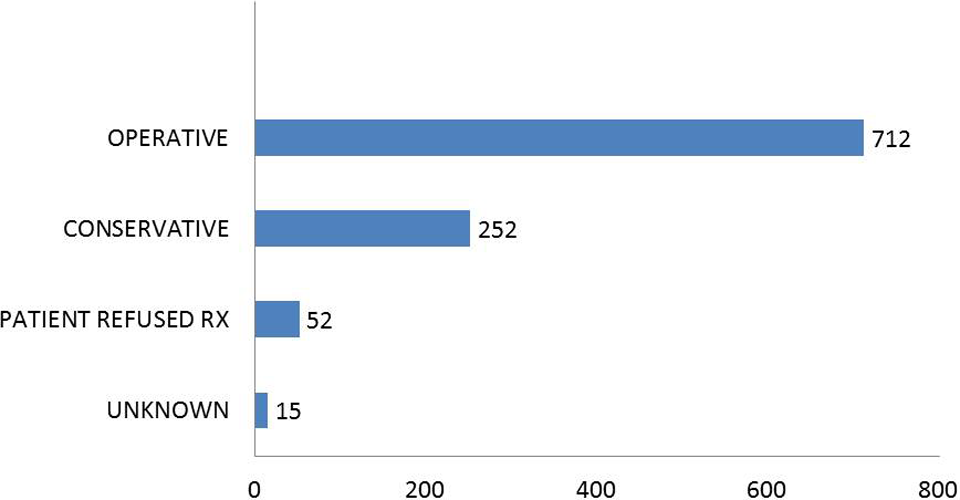
Type of treatment provided to the patients.
Patients had to travel huge kilometers to find quality service, a mean of 86.4 km with maximum being 321 km (P. Medinipur, West Bengal), as patients are often unsatisfied with the quality of care received at local areas or they are referred to higher centers; some of those who cannot afford the journey remain deprived of quality treatment. Majority (885 [85.9%]) of the patients present late to hospital (>1 day following fracture), with 50% presenting between 1 and 9 days (see Figure 5) with mean of 18 days and SD of 16.9 days, maximum being 20 years following the fracture. Causes for delay were mostly ignorance by the family members toward the elderly individuals and misguiding quack and nursing home practice at root level, delaying the patient’s presentation to higher centers for treatment. It was often seen that these patients would have spent huge amounts at those centers hence are unable to afford quality implants and treatment due to financial constraints. Commonest ASA grade was 3 (43%), and 92% of the surgeries were performed under spinal anesthesia.

Timing of patients’ presentation to the hospital (in days).
Despite patient’s presentation to the hospital, incidences of delayed surgeries excluding medically unfit (89 patients; see Figure 6; >2 days, including D0) were 69.3% (432 of 623 patients) with a mean of 3.7 days, SD of 2.9 days, and maximum delay of 12 days. Surgeries were often delayed due to delay in arrangement of funds for the operation, academic issues like public holidays, mechanical failure or strike, and fixed operative days of surgeon. Only 66 (9.26%) of 712 patients were operated within 24 hours of injury.

Timing of surgery (in days).
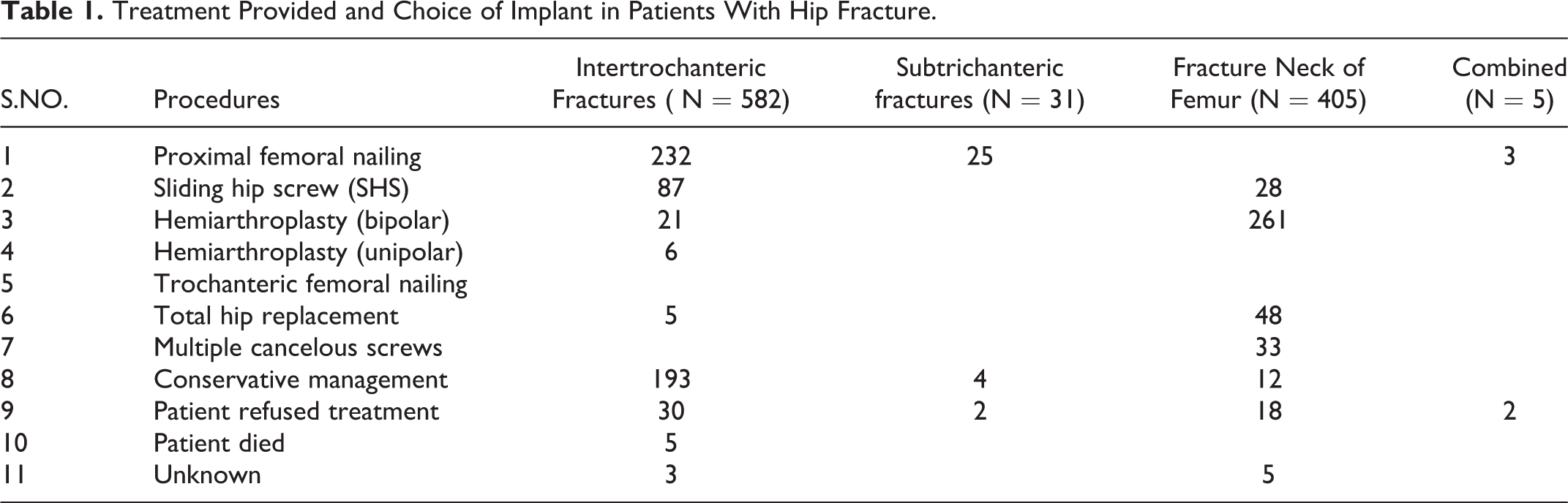
Persistent electrolyte (Na+/K+) imbalance and hyperglycemia in these patients generally returned to normal second or third postoperative day after fracture fixation as observed in 81.2% of operated patients. In patients with delayed presentation, delayed surgeries, or conservatively managed patients, these problems persist for long, superadded by depression, pressure sores, pneumonia, urinary tract infections, deep vein thrombosis, dehydration and disuse atrophy of muscles, and difficulty in operations due to contractures. Implants for fixation varied from dynamic hip screws, multiple cancellous screws, proximal femoral nailing, hemiarthroplasty, and total hip replacement (summarized in Table 1). Proximal femoral nailing was preferred for inter- and subtrochanteric fractures, whereas hemiarthroplasty (Bipolar prosthesis) was the choice of implant for femur neck fractures.
Treatment Provided and Choice of Implant in Patients With Hip Fracture.
In a country like India, patients are often accompanied by many attenders (average 3-4 per patient) who become part of the patient’s journey through treatment till discharge. In return, they also loose crucial man hours to work, that is, 157.85 h/19.7 d of work/person. Estimated losses according to lost man hours may go up to 10 million dollars.
Incidence of pressure ulcers was more with a relative risk of 2.4 in nonadmitted patients (66.6%, 132 of 197 patients) than in patients who were admitted and supervised (21.6%, 167 of 767). Medical complications like electrolyte imbalance, urinary tract infections, pneumonia, hyperglycemia, pressure sores, depression, and deep vein thrombosis were seen in 310 (40.4%) admitted patients and more in patients with delayed presentation to hospital and delayed surgeries (90%).
Rehabilitation started on the second postoperative day in a graded manner from passive to active exercises. In all, 709 (92.4%) admitted patients reached home by 30 days, with 365 (51.2%) admitted-operated patients bearing partial/full weight with an invalid walker at time of discharge. Mortality rate at 3 months was 6.2%. Fall assessment was performed by an orthopedician in 98% of the cases, and 100% of the cases received bone protection medications (with 20% receiving Zolendronic acid infusion). Mortality rate at 3 months was 6.2%. Of all the treated patients, 34% had government credits and facilities and the remaining 66% of the patients had to pay using personal funds. Majority of the patients from poor areas had to sell their lands to afford treatment. Also, majority of the savings were spent prior to arrival to the hospital.
Discussion
The phenomenon of population aging is becoming a major concern for the policy makers all over the world, for both developed and developing countries, during last 2 decades. 4 Hip fracture in elderly individuals is a burden for the society in terms of costs and for the single individual due to subsequent increased morbidity and mortality. 8 Old people have limited regenerative abilities and are more prone to disease, syndromes, and sickness when compared to other adults. Mortality associated with a hip fracture is about 5% to 10% after 1 month in patients who were neglected and patients who refused treatment, whereas in patients who were operated or managed conservatively under medical supervision, it was merely 3.2 %. The average age of patients with hip fracture is more than 80 years and nearly 80% are women. 1 In this study, fragility fractures were common in females (59.7%; female–male ratio, 1.5:1) with target age-group (60-80years). Most hip fractures result from a fall or stumble; only about 5% of cases have no history of injury. The incidence of hip fracture differs between and within continents, between rural and urban areas, between races within 1 country, between regions within countries and within a single city. The highest rates in the world were found in studies from Oslo, Norway. 9
India, now home to 1.2 billion people, is projected to overtake China in about a decade to become the world’s most populous country. The share of India’s population aged 50 and older will reach 34% by 2050. 10 In India, 65% of the aged individuals depend on others for day-to-day maintenance, and the situation is worse for elderly females (70%). 4 Combined, more than 0.75 billion people aged 60 and older will live in China and India in 2050, constituting 38.5% of the world’s 60-plus population. In India, by 2050, the proportion of people aged 60 and older will exceed that of people aged 0 to 14 years. According to population census (2001) in Odisha, 8.3% (3039-1536 female and 1503 male) of population aged 60 and older with a decadal growth rate of 25.2%. 4 In 2020, the projected annual cost of hip fractures in the United States is estimated to be US$16 billion and worldwide US $131 billion annually. 2
Many studies have found it detrimental to delay surgery. 11,12 Robbins and Donaldson 13 found that patients waited an average of 2.3 days in hospital until theater time became available. After fracture fixation, we observed correction of intractable hyperglycemia and electrolyte imbalance by second or third postoperative day. It has been suggested that trochanteric fractures are more closely related to osteoporosis and advancing age. The proportion of trochanteric fractures has been seen to be rising confirmed by our study. 14,15,16 Patients with hip fracture are at high risk of pressure ulcers 17 and can have significant negative effects in terms of pain, quality of life, length of hospital stay, cost of care, medical complications, and mortality. 18 The optimal treatment for these injuries is surgery, since nonoperative treatment was associated with longer hospitalization, more malunions, pressure ulcers, and less likely to return to an independent level of functioning. 19 Current guidelines suggest that Surgery for hip fracture should be performed within 24 hours of injury. 20 The incidence of hip fracture differs between and within continents, rural and urban areas, between races within one country, between regions within countries, and within a single city. 9,21 -24
Conclusion
Fragility hip fractures are common, incapitating but preventable injury of elderly individuals which make them dependent on family even for basic needs. Patients had to travel long distances for quality treatment, and many of them are misguided owing to ignorance and flourishing quack therapy in local areas and present late (85.9%) with significant complications and sufferings, with their pockets almost half drained depriving them of best treatment. Patients who present early and are operated early have better prognosis and rehabilitation and facilitates early return to work and independence. Increased pressure sores, infections, electrolytes imbalance, hyperglycemia, hospital stay, treatment cost, depression, and mortality are directly related to delays in surgeries and presentations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.