
Abstract
Many studies have shown that surgical management still leads to the best outcomes in elderly patients with hip fractures, with some studies showing non-inferiority of nonsurgical management as compared to surgery in fragility fractures. Evidence-based guidelines on whether to operate on these patients are lacking. A systematic literature search was conducted regarding outcomes of nonoperatively treated hip fractures in elderly patients with various comorbidities. A structured literature review of multiple databases (PubMed, Web of Science, EMBASE, and Cochrane library) referenced articles from 2000 to 2020. A total of 596 patients from 11 published studies were identified. Mean age was 83.3 years. Overall 328 (69.7%) complications occurred in 470 patients with nonsurgical treatment. Pneumonia and urinary tract infections were the most common complications which occurred in 53 (16.1%) and 46 (14.0%) patients, respectively. Hip fracture patients who were treated nonoperatively had a higher in-hospital (17.1% vs. 4.4%; p < 0.001), 30-day (31.4% vs. 10.2%; p < 0.001), and 1-year (48.5% vs. 19.9%; p < 0.001) mortality compared to a matched group of operatively treated patients (n = 1464). Of the 110 patients whose reported cause of death was nonoperative care, 44 (40%) was due to pneumonia. Patients with nonoperative treatment following hip fracture were associated with substantially higher complication and mortality compared with patients who were treated operatively. Our study will help health-care providers and caregivers to enable more informed decision-making for families and patients confronted with a hip fracture.
Introduction
The incidence of elderly hip fracture has been rising globally every year due to increase in the average life span with recent developments in medical technology. 1 It has been estimated that by 2050 half of hip fractures will occur in Asia and the total number of hip fractures in the Asian countries will increase from 1.12 million in 2018 to 2.56 million in 2050. 2,3 Even though operative management is the current standard of care for geriatric hip fracture patients, patients with poor general conditions are sometimes treated nonoperatively to avoid worsening of their status due to stress of surgery and anesthesia. Hip fractures in elderly patients deserve special attention because of their comorbidities.
Previously, it has been reported in a Cochrane Systematic Review that overall there was insufficient evidence to determine whether surgery is better than bed rest and traction for hip fractures tested in randomized trials. 4 Several studies also demonstrated that nonoperative management of hip fractures can produce acceptable results because a considerable number of patients were free of pain and could mobilize. 5,6 Kawaji et al. 6 suggested that nonoperative treatment should be considered for patients with poor ability for activities of daily living. However, the question whether nonsurgical treatment is appropriate for most fragile, elderly patients, with regard to quality of life, poses an ethical dilemma which should be addressed in an individualized manner. 7 Therefore, when discussing nonoperative hip fracture management with patients and their family, actually helpful and detailed information should be offered by providing updated mortality data. Nevertheless, our current knowledge about the mortality data of nonoperatively treated geriatric hip fracture patients is confined to a few reviews from single institutions or from multicenter national registries in one country, 8 even though the mortality rates may differ between patients of different ethnic backgrounds and nationalities. Few studies have presented the outcomes of nonsurgical treatment for fragility hip fracture patients, and groups were too small. 9 –11
The present study was designed to evaluate the outcome, complication, and mortality rate of geriatric hip fracture patients who underwent nonoperative management and to determine whether there was an associated reduced mortality with operative treatment with a review of the literature and pooled analysis. We therefore asked: (1) What are the outcomes and common complications of hip fracture treated nonoperatively in elderly patients? (2) What is the overall mortality rate after nonoperative management?
Methods
This review was conducted in accordance with the 2009 Preferred Reporting Items for Systematic Review and Meta-Analysis statement 12 to increase comprehensiveness and transparency of reporting.
Search strategy
A systematic literature search based on case–control study was conducted for hip fractures and treatment using multiple separate search strategies. Four computer databases (PubMed/MEDLINE, Web of Science, Embase, and Cochrane Library) were searched with the search words “hip fracture,” “femur neck fracture,” “intertrochanteric fracture,” “elderly,” “nonoperative,” and “mortality” in different combinations. With the assistance of a biomedical librarian, an initial search was conducted by the first author in January 2020, with an updated search conducted by the second author in March 2020 to ensure accuracy. No additional study was identified by repeating the search. A literature search from 2000 up to March 2020 was conducted (time restriction to the last 20 years) because mortality rates and surgical indications have changed recently due to advancements in medical technology.
Selection criteria
The inclusion criteria for the studies were (1) English-written articles in human species; (2) randomized controlled trials, non-randomized or quasi-randomized controlled trials, prospective cohort trials, or retrospective comparative studies; (3) femoral neck or intertrochanteric fracture (OTA/AO 31A and 31B 13 ); (4) articles reporting cases with elderly patients; (5) both retrospective and prospective series; and (6) only those articles that evaluated the final outcomes including mortality.
The exclusion criteria were (1) animal, biomechanical study; (2) conference presentations; (3) abstracts only; (4) greater trochanteric fractures, isolated lesser trochanteric fractures; (5) pathological fracture; (6) periprosthetic fracture; (7) acetabular and pelvic fractures 14 ; and (8) articles without the separate mortality rates for both groups (surgical and nonsurgical). 15 Limits for the number of patients in each study or the minimum duration of follow-up were not used. Only published clinical studies were included. Due to the limited evidence available on the topic, case series were included in our study.
To obtain more detailed clinical information including mortality and morbidity, we also intended to compare the clinical group of patients treated nonoperatively to a matched group of operatively treated patients by age, gender, hip fracture type, and American Society of Anesthesiologists (ASA) grade. 16 Surgical management consisted of cannulated screws, hemiarthroplasty, total hip arthroplasty, sliding hip screw construct, or cephalomedullary nail.
Study selection
Searching the aforementioned databases yielded a total of 1098 articles. The flow diagram of the study is shown in Figure 1. A first search of the PubMed database yielded 303 articles and a second search of the Web of Science database with use of the same search strategy yielded 276 articles. After removal of duplicate articles (n = 404), 694 unique titles and abstracts were screened for eligibility. Abstracts and full texts of the retrieved articles were read by two authors independently, and all relevant articles were read in full. Additionally, the reference lists of included studies were screened to minimize the risk of missing relevant articles. Discrepancies in selection between the two reviewers were resolved by consensus. In case of persistent disagreement, a third reviewer was consulted. Stringent exclusion criteria were applied, leaving 11 articles appropriate finally. As we could not identify any randomized or nonrandomized controlled trial, most of the larger cohorts giving an answer or at least an insight to clinical problems were selected for this review.

The flowchart of literature screening.
Data extraction
Two authors independently extracted data from all eligible studies. The extracted information included study characteristics and main outcome results. The primary outcome was mortality, either within hospital or during the first postoperative year. Secondary outcomes were average length of stay (LOS) and in-hospital complications. The corresponding authors of the included studies were contacted by e-mail if any required information was unavailable. The following data were also extracted: year of publication, country, level of evidence of included studies, demographics (age, gender), underlying disease, type of fractures, follow-up period, intervention, outcomes following treatment including complications, ambulatory status on admission and discharge, mortality after nonoperative treatment and surgery, and cause of death. As the measurements of patient characteristics and outcomes including mortality were consistent among the trials, we pooled these to derive mean values. The pooling of the functional assessment data sets was not attempted because of the significant variability in the criteria. Due to the qualitative, summative nature of this review and significant variations in study design, participants, treatments, and complications, a meta-analysis could not be conducted and effect sizes could not be calculated.
Statistical analysis
All data were recorded into an Excel spreadsheet (Microsoft Corp, Redmond, Washington, USA) and subsequently copied to a statistical analysis software SPSS version 18.0 (SPSS Inc., Chicago, Illinois, USA). Categorical data such as gender difference and in-hospital complications are given as n (%). The 30-day and 1-year mortality rates with odds ratio (OR) were extracted from the studies and included in the analysis. Mann–Whitney test was used to analyze nonparametric continuous data (overall ASA score). The χ 2 tests were used to determine any significant differences in categorical variables including mortality. Statistical analysis was performed by an independent statistician blinded to group allocations. All reported p values are two sided, and the values of p < 0.05 were considered significant.
Results
Search results and studies included
As presented in Figure 1, our systematic literature review of PubMed, Web of Science, Embase, and Cochrane literature searches revealed a total of 596 patients from 11 selected articles relevant to our research topic that met our criteria. The included observational studies were published between 2003 and 2019. Although complete data were not available, data such as age, gender, underlying medical/surgical conditions, and occurrence of serious complications were collected.
Demography
The patients who were treated nonoperatively for hip fractures between 1992 and 2016 were included in the present study. Sample sizes of each study ranged from n = 21 (Kawaji et al. 6 ) to n = 114 (Tay 17 ). The mean age of the overall patients was 83.3 years, and the mean age in each study ranged from 77.3 years (Jain et al. 18 ) to 86.7 years (Chlebeck et al. 19 ). The proportion of females ranged from 38% to 80.9%, with an overall mean of 67.3%. One paper 9 did not indicate the gender distributions of nonoperatively managed patients separately. Two studies 5,20 published only about displaced femoral neck fractures. Demographic information is detailed in Table 1. These patients were compared to a matched group of operatively treated patients (n = 1464). The matching was already performed in each study. 7,10,18,19,21 The mean age was similar for both the operative (82.6 years) and nonoperative groups (83.3 years). There was no significant difference in gender and presence of dementia (Table 2). Preinjury living location (home or institution) was reported in three studies. 7,10,19 Multiple comorbidities (acute or chronic) were identified in patients with nonoperative treatment. 5,7,18 However, it was unable to compare the number of underlying diseases between the two groups because the underlying diseases of surgical group were documented only in one article. 18 The overall ASA grade was higher for the nonsurgical treatment group (p = 0.001). There was a higher proportion of patients who were ASA grade 4 in the nonoperative group (26.8%) than the operative group (15.2%).
Demographic information of included studies.

NA: not available.
Patient characteristics for the comparative cohorts.

ASA: American Society of Anesthesiologists.
Treatment outcomes and complications
Due to reporting inconsistencies, analysis for persistent pain, functional outcome, or quality of life after treatment could not be performed. At the final follow-up, 164 patients (52%) treated nonoperatively were mobile with a wheelchair or better (three studies were not included 7,17,19 ). The mean LOS was informed in 9 studies (except 2 studies 20,21 ) and ranged from 5.3 days to 52.5 days. Duration of hospitalization was similar for patients who underwent surgery and those who were treated nonoperatively (15.8 days vs. 17.1 days, respectively). Operative treatment was associated with a reduced mean LOS. Rehabilitation protocol was not uniform among the authors or even in same series, and none of the studies analyzed outcomes upon rehabilitation methods.
The types of complications encountered in nonoperatively treated patients were reported by 8 studies (470 patients). Overall, 328 (69.7%) complications occurred in 470 patients with nonsurgical treatment. The most common complications were pneumonia and urinary tract infections which occurred in 53 (16.1%) and 46 (14.0%) patients, respectively. Common complications suffered by patients who managed nonoperatively are presented in Table 3. Other complications encountered were pulmonary embolism, sepsis, gastrointestinal bleeding, deep vein thrombosis, and pulmonary congestion.
Complications of patients treated nonoperatively.

Mortality
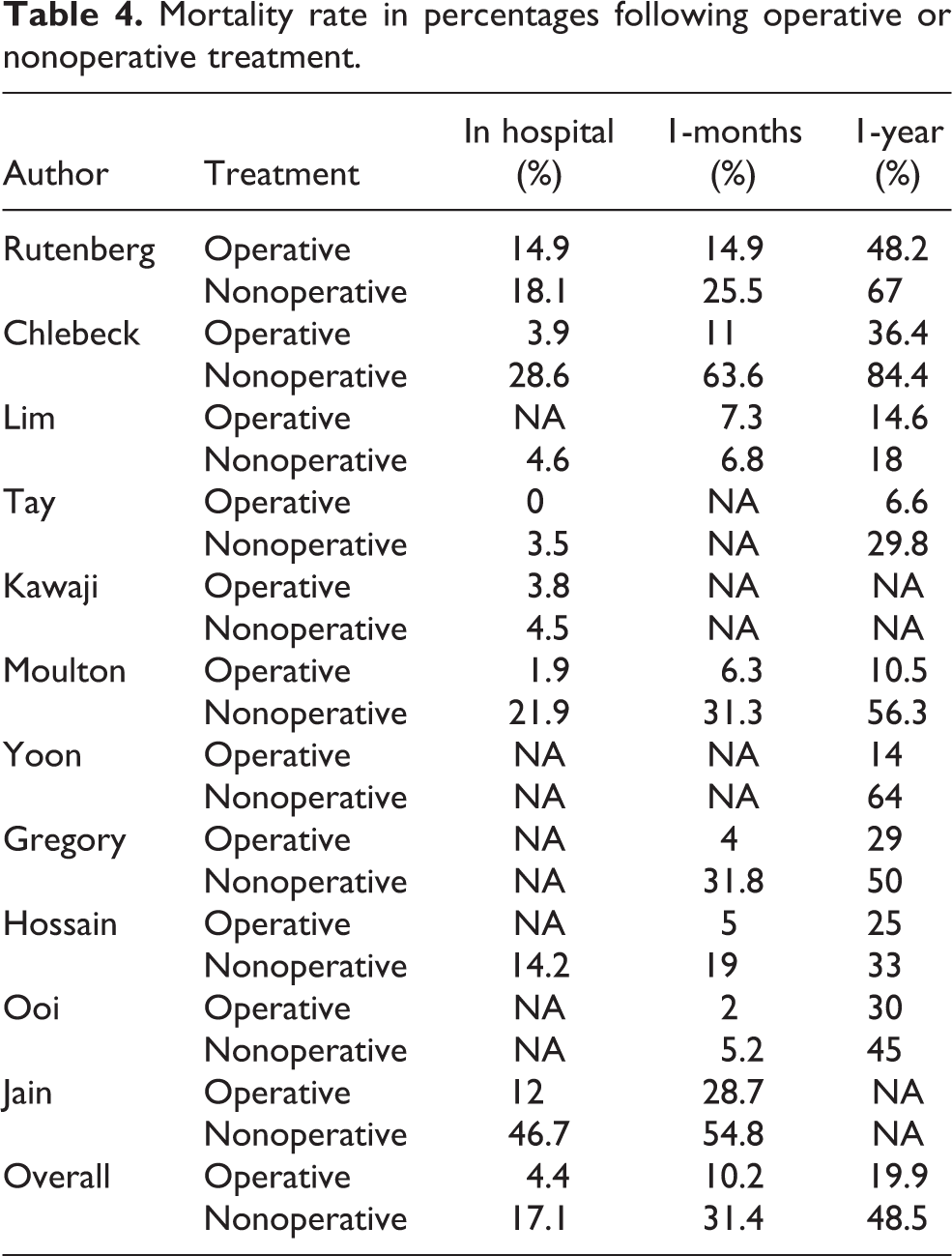
Causes for mortality were inconsistently reported, making interpretation of these data challenging. In the 110 patient pool with reported cause of death, 44 (40%) was due to pneumonia according to 5 studies. 5 –7,9,21 Hip fracture patients who were treated nonoperatively had a higher in-hospital (17.1% vs. 4.4%; p < 0.001), 30-day (31.4% vs. 10.2%; p < 0.001), and 1-year (48.5% vs. 19.9%; p < 0.001) mortality (Table 4). Nonoperative treatment was 4 times more likely to be associated with 1-month mortality compared to operative treatment (OR 4.0, 95% confidence interval (CI) 2.9–5.3; p < 0.001). At 1 year after fracture, the mortality risk of patients who were managed nonoperatively 3.7 times higher than that of those who underwent operative treatment (OR 3.7, 95% CI 3.0–4.7; p < 0.001).
Mortality rate in percentages following operative or nonoperative treatment.
Discussion
In this systematic review, we asked whether prognosis in patients who had been treated nonoperatively due to poor general health would be worse than that in patients who had undergone surgery. Our study found that geriatric hip fractures managed nonoperatively had significantly higher in-hospital, 30-day, and 1-year mortality compared with an operative cohort. While the majority of hip fractures in elderly patients are managed surgically with superior outcomes, 7 over the last 2 decades, few authors have tried to determine the outcomes of patients who were treated nonsurgically. 20,22 The outcomes of hip fracture managed nonoperatively are useful for the physician’s decision-making process.
Recently, one study showed that in patients with hip fractures, severe comorbidities, and poor general conditions, early prognosis after nonoperative treatment aiming for early transfer to wheelchair is no worse than that following surgical treatment. 6 Hossain et al. 10 reported that nonoperative management after hip fracture is suitable for medically unfit patients and does not result in statistically significant difference in functional outcome. However, in elderly patients with multiple comorbidities and hip fracture, the potential benefit of surgery should be considered together with the patients’ goals of care, and there is an opportunity to improve quality of care. In our pooled analysis, only 52% of patients treated nonoperatively were mobile with a wheelchair or better at the final follow-up. The others were shut-in patients and showed serious functional loss. Duration of hospitalization was similar for patients who underwent surgery and those who were treated nonoperatively (15.8 days vs. 17.1 days, respectively), even though operative treatment was associated with a slightly reduced mean LOS. The little difference of the LOS is probably due to the fact that the nonoperative cohort typically had discharge planning start immediately after making their nonoperative treatment decision. We believe, in routine cases, surgical intervention has better functional outcomes 23 than nonoperative treatment in terms of duration of stay in hospital, mobilization, and return to independent living. It also results in decreased hospitalization costs 24 and improved quality of life. 25 The Cochrane Review recommended that patients who are sufficiently fit should undergo surgical management for functional recovery. 4
Common complications of nonoperative management of hip fractures include the development of decubitus ulcers, pneumonias, thromboembolic disease, and urinary tract infections in addition to nonunions and malunions. 26 Traditionally, surgery was proposed to offset these complications. In the present study, the overall rate of complications of nonsurgical treatment groups was higher-than-expected (69%). Among them, pneumonia and urinary tract infections were the most common complications (16.1% and 14.0%, respectively). In addition, it is not surprising that the nonsurgical group will have more decubitus ulcers, because patients from the nonsurgical treatment group are less mobile to begin with. 27 Frenkel et al. 7 reported that the presence of decubitus ulcers was over 5 times higher for the nonsurgical group than the surgical group. Persistent pain was also more commonly reported among patients managed without surgery. 28 In the present study, even though causes of death were inconsistently reported and difficult to analyze, our data confirmed that pneumonia are reportedly the most likely causes for mortality among patients with proximal femoral fracture 6 with a pooled percentage of 40%.
It has been demonstrated that the overall inpatient mortality rates of hip fractures following surgical treatment approach 4% to 12%, 29 –31 while1-year mortality is between 12% and 37%. 32 Although many studies have assessed mortality and morbidity of surgically treated hip fractures in elderly patients, the mortality of nonoperative treatment is unclear and results differed between authors. Some found mortality to be higher in the nonsurgical treatment group, 19,21 while others did not reach the same result. 10,15 According to our systematic review, we have confirmed that hip fracture patients who were treated nonoperatively had a higher percent in-hospital (p < 0.001), 30-day (p < 0.001), and 1-year (p < 0.001) mortality. In addition, at 1 year after fracture, the mortality risk of patients who were managed nonoperatively was at least three to four times higher than that of those who underwent operative treatment. Our findings are consistent with studies of hip fracture in elderly patients that describe a survival benefit in persons undergoing surgical repair. 17 Because nonoperative management of hip fracture is associated with a high risk of displacement of the fracture, increased pain, loss of mobility, and increased mortality, 4,33 we believe it should be indicated only for patients who present late with a fracture that has begun to heal, are moribund, lack prospects for any functional recovery, or refuse surgery. 34
Limitations of this systematic review
There are several limitations to this study, which may have resulted in potential bias that should be addressed in further studies. First, most included studies were retrospective in nature, rendering reporting bias unavoidable. Due to the retrospective nature of data collection, some data were not available for analysis. In addition, a few patients with short-term follow-up were included in the present study which may have produced imprecise results. Longer time frame outcomes such as 2-year mortality were not able to be analyzed due to a paucity of data. Second, even though matched pairing was performed in several studies between the operative and nonoperative cohorts using age, sex, preinjury living location (home or institution), and presence of dementia, the groups were still different in terms of comorbidity due to deliberate selection bias. So, the comparison between two groups may not be valid. In other words, only medically stable patients underwent operation and nonoperative treatment was applied to the patients who were unwell. High mortality rates were probably due to the preexisting underlying diseases that made patients unfit for operation rather than the nonoperative treatment itself. Increased ASA grade in nonoperative cohorts must be associated with increased mortality following hip fracture. 35 In addition, some patients initially assigned to operative treatment might be changed to nonoperative treatment due to a major complication preoperatively. However, in the present study, we established strict selection and exclusion criteria to reduce selection bias as much as possible. In addition, there may not be significant bias in our series as our outcome measures are mostly hard and would not have been unduly influenced by observer bias. A future strictly designed and adequately powered trial is essential. 36 We believe that in the event that such a study is conducted, then, our study is one of the largest analyses in the literature comparing contemporary methods of operative and nonoperative treatment and can be used as the basis for power calculations.
Conclusion
In this systematic review, we found a significant difference of in-hospital, 30-day, and 1-year mortality between nonoperatively and operatively managed patients. Management decisions for elderly patients with multiple comorbidities should be guided by the goal of care as articulated by their health-care proxy. However, we believe that patients and their family should be counseled regarding the complications and increased risk of mortality if treated nonoperatively. Future research could help clinicians to determine specifically which category of patients could be treated nonoperatively by developing risk profiles.
Footnotes
Author contributions
SJK contributed to the study design and acquisition, analysis, and interpretation of the data. HSP and DWL conceived the study design and revised the data and manuscript. All authors had read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.