
Abstract
Background
To evaluate the clinical efficacy of PFNA in treating intertrochanteric fractures in super-elderly patients.
Methods
This study included patients aged over 90 years admitted to the orthopedic department of our hospital with intertrochanteric fractures between January 2021 and December 2023. The patients were categorized into two groups: the surgical group, which received treatment with PFNA, and the conservative group, which underwent tibial tubercle skeletal traction. PSM was additionally applied to control for confounding biases. Comparisons were conducted between the two groups concerning VAS scores at 1 week and 3 months post-admission, fracture healing time, complication rates, HHS, and SF-36 at the final follow-up, as well as 1-year survival rates.
Results
A total of 112 patients were enrolled, including 36 in the surgical group and 76 in the conservative group. After performing 1:1 PSM on baseline characteristics such as gender, age, BMI, bone density, Evans-Jensen classification, ASA grade, and CCI, 32 pairs of data were obtained, with 32 patients in the surgical group and 32 in the conservative group. Follow-up results indicated that the surgical group experienced faster pain relief, shorter fracture healing times, and lower incidence rates of most complications. Additionally, the HHS and SF-36 scores at the final follow-up were higher in the surgical group, and the one-year survival rate was also greater than that of the conservative group (P < 0.05).
Conclusion
For super-elderly patients with relatively good physical conditions who suffer from intertrochanteric fractures, the use of PFNA fixation, compared to conservative treatment, can achieve better limb function, a lower incidence of complications, and a higher survival rate.
Keywords
Introduction
According to the age stratification standards set by the World Health Organization (WHO), individuals aged 60-74 are classified as Young-Old Adults, those aged 75-89 as Old-Old Adults, and those aged 90 and above are defined as super-elderly. 1 This demographic is generally characterized by physiological frailty and multimorbidity, with a high prevalence of systemic diseases such as diabetes, hypertension, chronic heart failure, chronic obstructive pulmonary disease, post-stroke sequelae, chronic anemia, and malnutrition.2,3 This population often presents with severe osteoporosis, significantly increasing the risk of fractures following low-energy falls, with intertrochanteric fractures accounting for 63.7%, making them the leading cause of disability from elderly trauma. 4
Currently, there is no unified treatment standard established for super-elderly patients with intertrochanteric fractures. Conservative treatment, which requires prolonged bed rest, can lead to complications such as pressure sores, pneumonia, deep vein thrombosis (DVT), and urinary tract infections, significantly increasing mortality rates. 5 Even if fracture healing is achieved, it often results in complications such as hip internal rotation and limb shortening deformities, leading to loss of walking function and a dramatic decline in quality of life. 6 Although surgical treatment can restore biomechanical stability of the hip, 7 the perioperative stress response can trigger multiple organ dysfunction, accelerating patient mortality. 8
To explore the optimized treatment pathways for super-elderly patients with intertrochanteric fractures, this study conducted a retrospective cohort analysis of patients admitted to our hospital from 2021 to 2023 with intertrochanteric fractures. The clinical efficacy differences between surgical treatment and conservative treatment were compared, and the findings are reported as follows.
Material and Methods
Study Subjects and Design
This study conducted a retrospective cohort analysis, including 112 patients with intertrochanteric fractures admitted to our hospital’s orthopedic department from January 2021 to December 2023. Based on intervention strategies, the patients were divided into a surgical group of 36 cases, who underwent Proximal Femoral Nail Antirotation (PFNA) internal fixation, and a conservative group of 76 cases, who received tibial tubercle skeletal traction. After discharge, all cases followed a standardized follow-up protocol: regular monthly visits for fracture healing assessment until radiological confirmation of bony union, with final follow-up conducted at 12 months. Data collection encompassed baseline variables: gender, age, body mass index (BMI), bone density, Evans-Jensen classification, American Society of Anesthesiologists Classification (ASA) grade, Charlson Comorbidity Index (CCI) and efficacy endpoints: visual analog scale (VAS) scores on the 7th day and 3 months of admission, time to fracture healing, cumulative complication rates, Harris hip scores(HHS) at final follow-up, and scores for the physical component summary (PCS) and mental component summary (MCS) of the Medical Outcomes Study Short-Form 36 (SF-36), along with 1-year postoperative survival rates. To control for confounding biases, a 1:1 propensity score matching (PSM) approach was employed to adjust for the aforementioned variables, including age, ASA, and CCI. This research methodology adheres to the STROBE guidelines. All patients provided informed consent, all procdures in this study adhered to the ethical principles of clinical research outlined in the Declaration of Helsinki and the study was approved by the Medical Ethics Committee of our Hospital.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Age ≥ 90 years; (2) Three-dimensional CT shows intertrochanteric fracture; (3) Admitted for PFNA surgical treatment or conservative treatment with tibial tuberosity traction. Exclusion criteria: (1) Patients with multiple injuries; (2) Pathological fractures; (3) Open fractures; (4) Patients with significant vascular or nerve injuries; (5) Patients with pre-existing functional impairment of the affected lower limb prior to injury; (6) Patients who did not follow up as required; (7) Patients with mental disorders who are unable to cooperate with physical examination and follow-up.
Sample Size Calculation
The sample size was determined a priori based on the HHS. According to Guo et al, 9 conservative treatment yields a mean HHS of 60 ± 15 in super-elderly intertrochanteric patients. We hypothesized that surgical intervention would elevate the HHS to 80 ± 10. With α = 0.05 (two-sided), β = 0.20 (power = 80%), and effect size d = 1.33 (Cohen’s d), the required sample size was calculated to be 28 per group. To account for a 20% attrition rate and potential covariate imbalance, the target enrollment was set at 35 participants per group. After performing 1:1 PSM, 32 matched pairs were analyzed, achieving a power of 99.8% to detect the observed difference in HHS. Recruitment was constrained by the annual incidence of super-elderly intertrochanteric fractures. Although the target of 35 participants per group was not reached, the actual effect size exceeded the projections, indicating that the post-PSM sample was sufficient for detecting the primary outcome.
Intervention Measures
Treatment Method
Surgical Group
After admission, patients underwent systematic laboratory evaluations to specifically correct anemia (target hemoglobin > 90 g/L), hypoalbuminemia (target albumin > 30 g/L), and electrolyte imbalances (with a focus on potassium, sodium, and calcium ion balance). For patients with underlying diseases, optimization of organ function was conducted through a multidisciplinary team (MDT) consultation involving cardiology, respiratory, and endocrinology specialists. Low molecular weight heparin anticoagulation was initiated 24 h prior to surgery. The surgery was performed under general anesthesia with the patient positioned supine on an orthopedic traction table. After satisfactory reduction of the fracture was confirmed using a C-arm fluoroscope, routine disinfection and draping were conducted. A longitudinal incision, approximately 3-5 cm in length, was made at the proximal end of the greater trochanter. The skin, subcutaneous tissue, and fascia lata were incised layer by layer, and the gluteus medius muscle was bluntly separated to expose the apex of the greater trochanter. A guide pin was inserted at the apex of the greater trochanter, and its position within the femoral medullary cavity was confirmed using the C-arm in the anteroposterior view. An opening was created along the guide pin using a retractor, and a PFNA main nail of appropriate length and diameter was slowly inserted into the medullary cavity along the guide pin, with fluoroscopic confirmation of the nail depth. An aiming device was installed, and a hole was drilled through the lateral cortex, positioning the guide pin at the lower third of the femoral neck. The length of the guide pin was measured, and after drilling, a spiral blade was inserted. A distal locking screw was placed through the aiming device, with the C-arm confirming the length and position of the screw. The incision was irrigated with saline, hemostasis was achieved thoroughly, and the fascia, subcutaneous tissue, and skin were sutured layer by layer, followed by coverage with a sterile dressing. Anticoagulation therapy was restarted 24 h post-surgery, and wound dressing was changed while reviewing various indicators, with blood transfusion administered as necessary. Patients were instructed to perform ankle pump exercises. On the seventh postoperative day, a re-evaluation of various indicators was conducted, along with an X-ray examination of the affected hip joint. A rehabilitation therapist conducted both active and passive flexion-extension exercises for the lower limbs, as well as turning exercises. Stitches were removed on the fourteenth postoperative day, and Once clinical parameters normalized, the patient was discharged. After discharge, patients were advised to continue rehabilitation exercises to strengthen muscle power and improve range of motion. Regular follow-ups were scheduled as per medical advice, with re-evaluation through X-rays. Once the fracture has healed, gradual weight-bearing walking with the aid of a walker can be initiated (Figure 1A, C and D). Treatment of Intertrochanteric Fractures With PFNA (A); Tibial Tuberosity Traction Treatment (B); A 95-Year-Old Patient With an Intertrochanteric Fracture Was Sitting on the Bed Drinking Water (C) and Washing Hands (D) Two Weeks After PFNA Fixation
Conservative Group
Immediately after admission, patients underwent bone traction on the affected side’s tibial tuberosity (with traction weight set at 10%-15% of body weight) to achieve preliminary stabilization of the fracture. Simultaneously, a systemic internal environment regulation plan was initiated: targeted correction of anemia (target hemoglobin > 90 g/L), hypoalbuminemia (target serum albumin > 30 g/L), and electrolyte imbalances based on laboratory test results. If necessary, concentrated red blood cells or human albumin were administered intravenously. All cases routinely received low molecular weight heparin prophylaxis. Patients with underlying diseases underwent multidisciplinary consultations (led by cardiology, respiratory medicine, and endocrinology) to develop comorbidity management strategies aimed at optimizing organ functional reserve. Throughout the treatment, a standardized ankle pump training program was executed under the supervision of a physical therapist. After a 14-day hospitalization period with dynamic monitoring, bone traction was removed, and patients transitioned to home rehabilitation. Post-discharge, patients continued bed rest and followed regular follow-up appointments as per medical advice, including reexamination of X-rays. Once the fracture healed, rehabilitation exercises for the affected lower limb could be intensified, and gradual attempts to walk could be made (Figure 1B).
Outcome Measures
Outcome indicators include VAS scores on the 7th day and 3 months of admission for two groups, fracture healing time, incidence of complications, HHS and quality of life measured by the SF-36 at the last follow-up, as well as one-year survival rates.
The criteria for assessing fracture healing adhere to a multimodal comprehensive evaluation principle: (1) Radiological healing: Continuous anteroposterior X-rays show complete disappearance of the fracture line, with continuous connectivity of the trabecular bone; (2) Clinical functional assessment: Negative axial percussion pain in the affected limb, and no significant pain during active/passive range of motion testing. All physical examinations are conducted by senior orthopedic attending physicians. Radiological interpretation follows a double-blind protocol—two senior radiologists independently evaluated the images. In the event of discrepancies, a consensus meeting is held to integrate clinical and imaging data to form a final diagnosis.
This study records all complications occurring in patients during hospitalization and follow-up. The main complications include malunion, failure of internal fixation (surgical group), surgical site infection (surgical group), delirium, DVT, pressure ulcers, pneumonia, and urinary tract infections. The criteria for malunion are defined as follows: on a standard X-ray, if the neck-shaft angle is less than 120° or greater than 135°, or if there is a shortening of more than 2 cm on the affected side. Failure of internal fixation includes imaging-confirmed screw loosening, plate fracture, or femoral head cut-out; surgical site infection is classified into superficial infection (redness/tenderness at the incision with purulent discharge) or deep infection (involving the fascial layer with positive bacterial cultures). Delirium is diagnosed using the Confusion Assessment Method (CAM), which requires the presence of an acute change in consciousness, attention deficits, and cognitive disturbances, while excluding dementia, intoxication, metabolic disorders, and neurological diseases. DVT is confirmed based on compressive ultrasound showing venous incompressibility and absence of blood flow signals. Pressure ulcers follow the staging criteria set by the National Pressure Injury Advisory Panel (NPIAP), recording lesions of Stage I (non-blanchable erythema) and above. Pneumonia requires chest CT to show new infiltrates consistent with clinical signs of infection (fever, purulent sputum, or elevated white blood cell count). The diagnosis of urinary tract infection is based on quantitative urine culture (≥105 CFU/mL) and pyuria (urine sediment WBC ≥10/HPF). All diagnoses of complications are based on predefined objective criteria to minimize judgment bias.
This study utilizes the SF-36 to assess the quality of life of patients. The survey comprises eight standardized dimensions: Physical Functioning (PF), Role-Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role-Emotional (RE), and Mental Health (MH). According to the internationally accepted scoring rules, the aforementioned dimensions can be aggregated into two summary component scales: PCS, which comprehensively assesses the PF, RP, BP, and GH dimensions, reflecting physical functional status, pain interference, and health perception; and MCS, which integrates the VT, SF, RE, and MH dimensions, measuring vitality levels, social adaptation, and emotional regulation capabilities. This study compares the differences in PCS and MCS scores between the two groups at their final follow-up.
Statistical Analysis
Statistical analysis was conducted using SPSS 24.0. Data are presented as means ± standard deviations. For quantitative data, either analysis of variance or the Wilcoxon test was employed, depending on the data distribution. The Cochran-Mantel-Haenszel (CMH) chi-square test was utilized for ordered categorical data, while the Pearson chi-square test or Fisher’s exact test was used for binary or unordered categorical data. A P-value of less than 0.05 was deemed statistically significant. To address imbalanced baseline characteristics, PSM was additionally applied. Covariate balance after PSM was assessed using both hypothesis testing (P < 0.05) and standardized mean differences (SMD). For binary variables, report the absolute percentage difference (APD); For ordinal categorical variables, calculate the maximum cumulative distribution difference (MCD).
Results
Baseline Patient Profiles
Comparison of Baseline Data Between the Two Groups
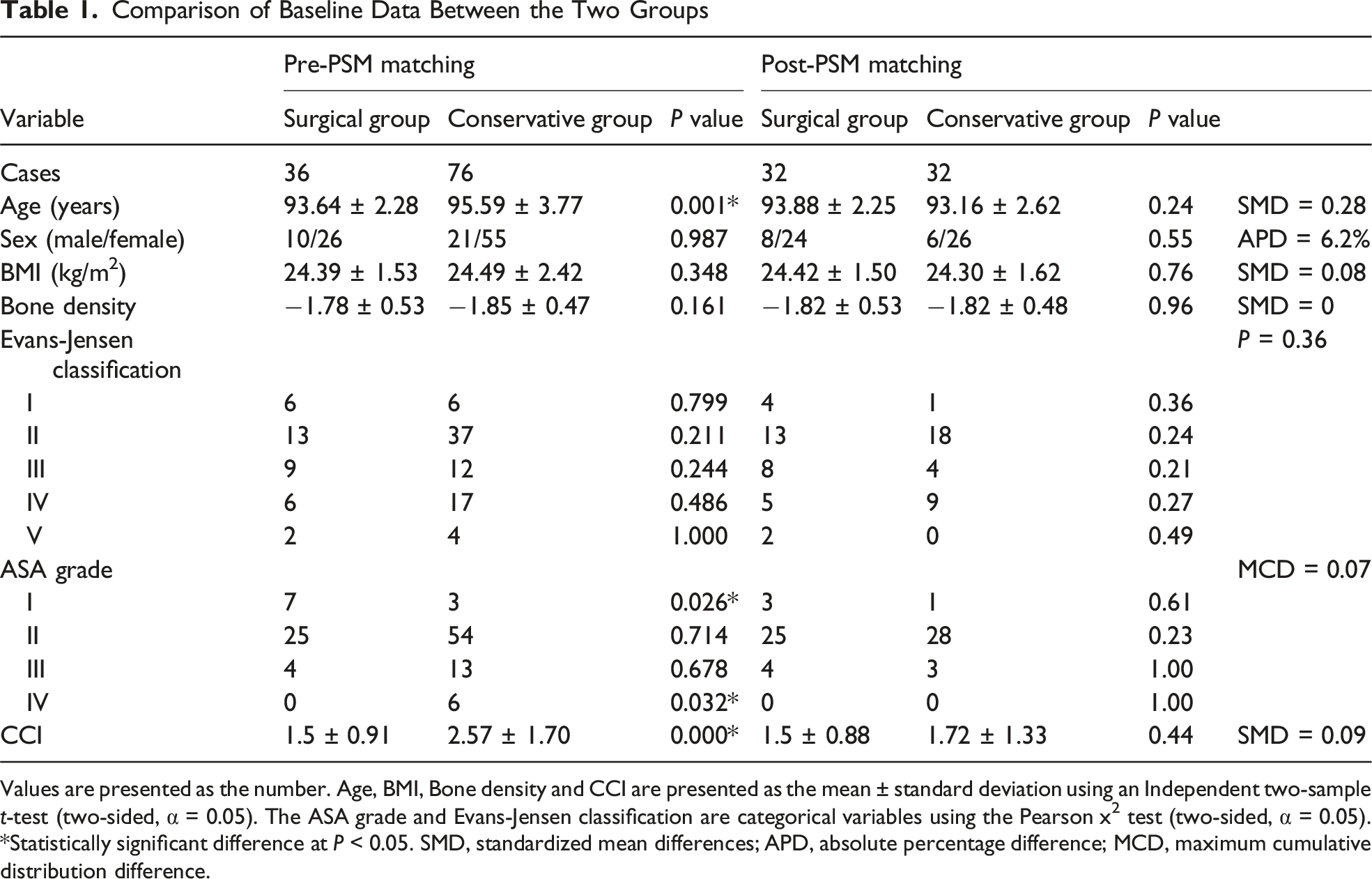
Values are presented as the number. Age, BMI, Bone density and CCI are presented as the mean ± standard deviation using an Independent two-sample t-test (two-sided, α = 0.05). The ASA grade and Evans-Jensen classification are categorical variables using the Pearson x2 test (two-sided, α = 0.05). *Statistically significant difference at P < 0.05. SMD, standardized mean differences; APD, absolute percentage difference; MCD, maximum cumulative distribution difference.

Participant Screening and Cohort Allocation
Clinical Efficacy
Comparison of Outcome Measures Between the Two Groups

VAS score, Fracture healing time, Harris score and SF-36 are presented as the mean ± standard deviation using an Independent two-sample t-test (two-sided, α = 0.05). The Complications and 1-year survival rate are categorical variables using the Pearson x2 test (two-sided, α = 0.05). MD, Mean Difference; OR, Odds Ratio; CI, Confidence Interval, *Statistically significant difference at P < 0.05.
Discussion
According to the 2017 report on the World Population Prospects published by the United Nations Department of Economic and Social Affairs, the population of individuals aged 90 and above in China has surpassed 2 million, accounting for over 15% of the global population in this age group. It is projected that this figure will exceed 3 million by 2030. 10 This significant trend of population aging is accompanied by a sharp increase in the number of elderly patients with hip fractures. 11 In the treatment of intertrochanteric fractures in such patients, the decision-making between surgical and conservative treatment has always been one of the challenges in clinical practice, and there is currently no unified standard for treatment options. 12
Bolton et al conducted a retrospective cohort study analyzing the prognosis of 60 patients over the age of 100 with hip fractures based on data from the National Hip Fracture Database (NHFD). The study found that even for extremely elderly patients, surgical treatment can significantly improve their quality of life. 13 The results emphasize that optimizing treatment strategies, including early surgical intervention and a multidisciplinary collaboration model during the perioperative period, is a key factor in improving prognosis. 14 The conclusion of the study suggested that clinical decision-making for super-elderly hip fracture patients should be based on a comprehensive assessment of the patient’s functional status (such as daily activity ability and cognitive level), 15 and individualized treatment goals should be established rather than relying solely on age as a decisive indicator of prognosis.9,16
In the treatment of patients with super-elderly intertrochanteric fractures, our study emphasizes the need for flexible decision-making based on the specific circumstances of each patient. Although the ASA grade and the CCI provide important quantitative references for surgical risk—data indicates that patients with ASA ≥ IV have a 2.3-fold increase in postoperative complication risk, and those with a CCI ≥ 4 have a one-year survival rate of less than 45% 17 —clinical practice has not established strict numerical thresholds as absolute contraindications for surgery. The surgeon must integrate multiple factors, including the patient’s physiological reserve, cognitive function, and social support, to conduct a comprehensive assessment through MDT model, 18 In this context, anesthesiology focuses on evaluating cardiopulmonary compensation capacity, critical care medicine predicts perioperative organ support needs, and rehabilitation develops early functional reconstruction plans. The principles of Enhanced Recovery After Surgery (ERAS) are consistently emphasized throughout, 19 highlighting the importance of precise interventions such as optimizing cardiopulmonary function, correcting nutritional status, and preventing thrombosis within 48 hours. It is noteworthy that the treatment willingness of patients’ families and the quality of communication with the medical team constitute key variables: when family members exhibit deep anxiety regarding surgical risks, even if the patient’s physiological indicators remain within the surgical range, the final decision may still lean towards conservative treatment. This decision-making model reveals that the treatment of super-elderly patients is not merely a selection of physiological indicators, but rather a dynamic balance between quality of life and treatment risks in the context of shared decision-making between doctors and patients. Adequate informed consent and a trusting relationship are the cornerstones for achieving optimal treatment outcomes.
The incidence of complications after intertrochanteric fractures in super-elderly patients is relatively high, 20 A multicenter study conducted in the UK included 24 523 patients from 77 hospitals, revealing that the main complications in elderly patients following hip fractures include malunion, delirium, DVT, pressure ulcers, pneumonia, and urinary tract infections. Furthermore, if surgical treatment is employed, patients also face risks such as implant failure and surgical site infections. 21 The results of our study indicate that, compared to the conservative group, patients in the surgical group experienced a significantly lower incidence of complications such as DVT, pressure ulcers, and pneumonia. The reason for this is that patients in the surgical group were able to begin non-weight-bearing functional training for the lower limbs within 48 h postoperatively, effectively reducing the risk of DVT. 22 Additionally, surgical treatment facilitates the implementation of standardized positional management. According to the literature, axial turning can reduce the incidence of pressure ulcers by 58%, while postoperative back patting to facilitate sputum drainage can decrease the risk of pneumonia by 42%.23,24 Surgical treatment allows for more precise fracture reduction, which is beneficial for restoring the normal neck-shaft angle of the hip joint and reducing the risk of malunion. Stable internal fixation can alleviate early pain in patients and promote fracture healing. 25 In contrast, patients undergoing conservative treatment often struggle to tolerate prolonged traction therapy, which can lead to loss of reduction and various forms of malunion. However, the incidence of delirium in the surgical group was slightly higher, but there was no statistically significant difference. This may be attributed to perioperative stress, the complexity of pain management, and the lack of preoperative cognitive assessments for the patients. Future research should prospectively collect baseline cognitive data and integrate delirium prevention into the ERAS protocol. Critically, there was a significant difference in hip joint function between the two groups at the final follow-up, with the surgical group achieving a HHS of 84.38 ± 9.75, indicating a good level, while the conservative group only scored 61.56 ± 24.05. Poor recovery of hip joint function directly leads to a decline in the quality of life for patients and affects their physical and mental health, 26 as evidenced by the significantly lower PCS and MCS scores in the conservative group on the SF-36 scale compared to the surgical group.
This study focuses on the surgical and conservative treatment options for super-elderly patients with intertrochanteric fractures. It is important to note that the inclusion criteria for the conservative treatment group tend to favor patients with extremely high surgical risks or severe comorbidities, resulting in a significantly poorer baseline health status, which may lead to selection bias. Baseline data show that the age, ASA grade, and CCI of the conservative group are significantly higher than those of the surgical group (P < 0.05). To control for confounding factors, we employed PSM to adjust for baseline variables, ultimately obtaining 32 pairs of baseline-balanced matched cases. It is noteworthy that the health status of patients in the successfully matched conservative treatment group was better than that of the overall group. Therefore, the conclusion of this study may be more applicable to a subgroup with a lighter burden of comorbidities and should not be directly extrapolated to all super-elderly populations,particularly those excluded by PSM. Specifically, post-PSM exclusion of 44 higher-risk patients may underestimate conservative treatment mortality. In real-world conservative treatment cohorts, patients are often more frail, which may result in a lower one-year survival rate. Therefore, the surgical benefits we report may be conservative— the actual advantages could be greater compared to patients receiving non-selective conservative treatment. This is one of the limitations of the current study. Future research needs to include a broader patient population in a prospective design to validate the absolute survival benefits of PFNA in the overall super-elderly population.
Secondly, another limitation of this study pertains to the analysis of complications. Although the statistical power was sufficient for the primary outcome (HHS) after PSM, the individual complications (eg, DVT, pneumonia, pressure ulcers) are inherently low-incidence clinical events. The post-matching sample size (n = 64), while adequate for detecting differences in functional scores, provides a limited number of events for the analysis of these relatively rare outcomes. Consequently, some odds ratios (ORs) are based on few event counts, resulting in wide confidence intervals and underpowered statistical tests. Therefore, the comparative findings regarding complication rates should be interpreted as preliminary and indicative, requiring validation by future studies with larger sample sizes to provide more precise and reliable estimates of the effect sizes.
Thirdly, although we employed PSM to minimize selection bias, there remains a slight age imbalance between the surgical group and the conservative group after matching (SMD = 0.28). While the absolute difference of 0.72 years (93.88 vs 93.16) has very low clinical relevance in populations over 90 years old, and all other important prognostic variables have achieved excellent balance, we acknowledge that this is still a limitation from a purely methodological perspective. However, considering the substantial differences observed between the two groups in terms of primary functional outcomes (HHS difference > 22) and survival rates (difference > 21%), such a degree of age imbalance is highly unlikely to be the primary driver of these results. Nevertheless, future studies with larger sample sizes are expected to achieve perfect balance across all covariates, including age.
Existing evidence primarily focuses on the comparison between surgical and conservative treatments for elderly patients under 80 years of age, while direct comparative studies targeting the super-elderly population (≥90 years) are severely lacking. This study addresses the baseline heterogeneity issue in this population through PSM, rigorously adjusting for core covariates such as age, ASA classification, and the CCI, thereby isolating confounding factors in the super-elderly group. It provides a decision-making basis for treatment strategies for fractures in the super-elderly. However, this study has certain limitations. It is a retrospective analysis that introduces selection biases, as all patients were sourced from a single center and the sample size is relatively small. Future research should validate the universality of treatment strategies in a broad super-elderly population through prospective, multi-center collaborative studies with larger sample sizes and clarify the optimal selection criteria for indications.
Conclusion
The results of our study indicate that for super-elderly patients with intertrochanteric fractures who meet the surgical tolerance criteria, undergoing PFNA surgery significantly improves postoperative hip joint functional, effectively reduces the incidence of complications, and enhances patient survival rates compared to conservative treatment options. Therefore, under the strict adherence to indications, age ≥90 should not be a contraindication for surgery when physical status allows. PFNA surgery can be considered a preferred treatment strategy for this specific patient population, and the MDT model holds an irreplaceable core value for them.
Footnotes
Ethical Considerations
All procedures in this study adhered to the ethical principles of clinical research outlined in the Declaration of Helsinki and the study was approved by the Medical Ethics Committee of Shanghai Seventh People’s Hospital (SSJW-2020105). This is a retrospective study and clinical trial number: not applicable.
Consent to Participate
All patients provided informed consent.
Consent for Publication
All authors were involved in revising it critically for important intellectual content, and all authors approved the final version to be published.
Author Contributions
L BL and Y X contributed to the research design and implementation, and made in-depth discussions on research hotspots and technical difficulties. A RG and L BL collaborated on developing the patients’ treatment plans, while L DM, L XK and L HJ were in charge of collecting the patient’s information and images. Yu X and LDM handled the writing of the article and statistical analysis. Additionally, all authors actively participated in the patient’s surgery and follow-up. All authors were involved in revising it critically for important intellectual content, and all authors approved the final version to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by New Quality Clinical Specialty Program of High-end Medical Disciplinary Construction in Shanghai Pudong New Area (2024-PWXZ-21); Talents Training Program of Seventh People’s Hospital of Shanghai University of Traditional Chinese Medicine (Grant No. LJ2024-01).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to ethical restrictions and participant confidentiality agreements, the raw data are not publicly available. De-identified data may be requested from the corresponding author with approval from the institutional ethics committee.