
Abstract
Purpose:
To evaluate and compare the accuracy of the placement of thoracic pedicle screws between concave and convex side curve using freehand technique and triggered electromyogram (EMG).
Methods:
Three-hundred sixty eight thoracic pedicle screws were included for the evaluation of accuracy from postoperative computed tomography (CT) scans in 24 patients with adolescent idiopathic scoliosis with a mean follow-up of 27 months (range 24–58 months). All screws had stimulation thresholds greater than 6 mA. We divided the screws into two groups: (1) group A: concave side curve—254 screws (2) group B: convex side curve—114 screws.
Results:
The mean age at surgery was 12.8 years (range 11–17 years). The preoperative Cobb angle was 57.5° (range 50–75°). There were 41 total breaches (medial = 21, lateral = 20, p = 0.66) with an overall incidence of 11.1%. The overall breach rate did not attain statistically significant difference (group A = 11.8%, group B = 9.6%, p = 0.59). The rate of medial breaches was also similar for both concave and convex side (group A = 6.1%, group B = 5.9%, p > 0.05). No postoperative neurological or vascular complications were noted in both groups.
Conclusion:
Thoracic pedicle screw placement using both freehand technique and triggered EMG for adolescent idiopathic scoliosis surgery is safe and reliable. The overall accuracy rate is 88.9% with similar breaches on the concave and convex side on postoperative CT scans.
Keywords
Introduction
Correcting deformity using thoracic pedicle screw instrumentation in patients with adolescent idiopathic scoliosis (AIS) has been widely accepted with superior results. Although the use of thoracic pedicle screws may result in better deformity correction and fixation, the safe and accurate placement of these screws is still considered technically challenging, especially on concave side because of the small size or the absence of thoracic pedicle, the potential risk to the great vessels, and spinal cord displacement to the concave side. 1 –6 The rates of penetrating the pedicle cortex, depending on the employed techniques, have ranged from 15.9% to 54.7% in laboratory studies with cadavers. 7,8 Clinically, bony landmarks and intraoperative C-arm X-rays are commonly used to determine the correct placement, yet these methods are frequently inaccurate with large dose X-ray exposure and longer operation time. 1,7,9,10
Among several techniques for pedicle screw insertion, freehand technique with triggered electromyogram (EMG) is one of the common methods in terms of accuracy, operation time, radiation exposure to the patients and spine surgeons. 11 Although no absolute threshold or range of threshold values was correlated with medially breached screws, a previous study of seven cases showed that pedicle screws that had stimulation threshold greater than 6 mA in AIS patients were safe, with the overall reliability of 90.3%, as was firmly assessed on the postoperative computed tomography (CT) scans. 12
There is still controversy about the different accuracy of pedicle screw placement in the concave and convex side. 4 –6,13
The purpose of this study was to evaluate the difference in accuracy of thoracic pedicle screw placement between concave and convex side using both freehand technique and triggered EMG.
Materials and methods
After approval from the institutional review board, 24 AIS patients who have postoperative CT scans with all pedicle screw construct were included. Patient consent for the use of medical information was provided at the time of surgery. The mean body mass index of the patients was 21.2 kg/m2 (range: 14.6–27.4 kg/m2). All patients were treated by a single surgeon at a single institution. The mean age at the time of operation was 12.8 years (range 11–17 years). The average preoperative Cobb angle was 57.5° (range 50–78°). All pedicle screws were inserted using freehand technique: A probe was advanced into the vertebral body through the pedicles, using the so-called gearshift technique, turning the probe 180° medially after initial advancement at the entry point. A sounding device was then used to palpate five bony borders (the floor and the proximal, distal, medial, and lateral borders). Using a tapper, the pedicle hole was tapped and the tapped pedicle hole was palpated again. A proper sized pedicle screw was placed into the hole. The triggered EMG activities from stimulation of the screws were recorded from the abdominal muscles. The intraoperative EMG monitoring system we used was a commercially available neural integrity monitoring spine system (NIM-Spine system, Medtronic Sofamor Danek, Memphis, Tennessee, USA) (Figure 1). After finishing the insertion of all pedicle screws, intraoperative fluoroscopic images were obtained for final confirmation. General anesthesia was done by a special spine anesthesiologist who followed the recommended anesthesia protocol for motor evoked potential (MEP) monitoring. The diameter of all screws was 5.5 mm, and the length of the pedicle screw was from 35 mm to 40 mm. In total, 368 thoracic pedicle screws were divided into two groups: (1) group A: concave side curve—254 screws and (2) group B: convex side curve—114 screws. The postoperative CT scans were read by two surgeons (spine surgeon and spine fellow). The thoracic vertebral levels that were instrumented included T1 (10 screws), T2 (9 screws), T3 (8 screws), T4 (40 screws), T5 (42 screws), T6 (38 screws), T7 (36 screws), T8 (31 screws), T9 (39 screws), T10 (37 screws), T11 (38 screws), T12 (40 screws) (Figures 2 and 3). Two spine surgeons reviewed the postoperative CT scans of all patients through the picture archiving and communication system system with the help of software at a magnification of 300%. Criteria for breach of the pedicle screw are as follows: in—intraosseous or <2 mm breach, out—>2 mm breach through medial or lateral pedicle wall (Figure 4). All screws were assessed for intrapedicular placement and length twice, and their average values were used for final decision (r = 0.92, Pearson’s correlation coefficient). Paired t-test was used for statistical analysis for comparison of the breach rate of concave and convex side.

Intraoperatively triggered EMG monitoring: placement of the electrodes used to record the triggered EMG through the stimulation of the pedicle screws. EMG: electromyogram.

Female, age 15 years, and had double thoracic curve. Cobb’s angle was 50° and 67° and corrected to 24° and 26° postoperatively. All pedicle screws were inserted properly at all levels.
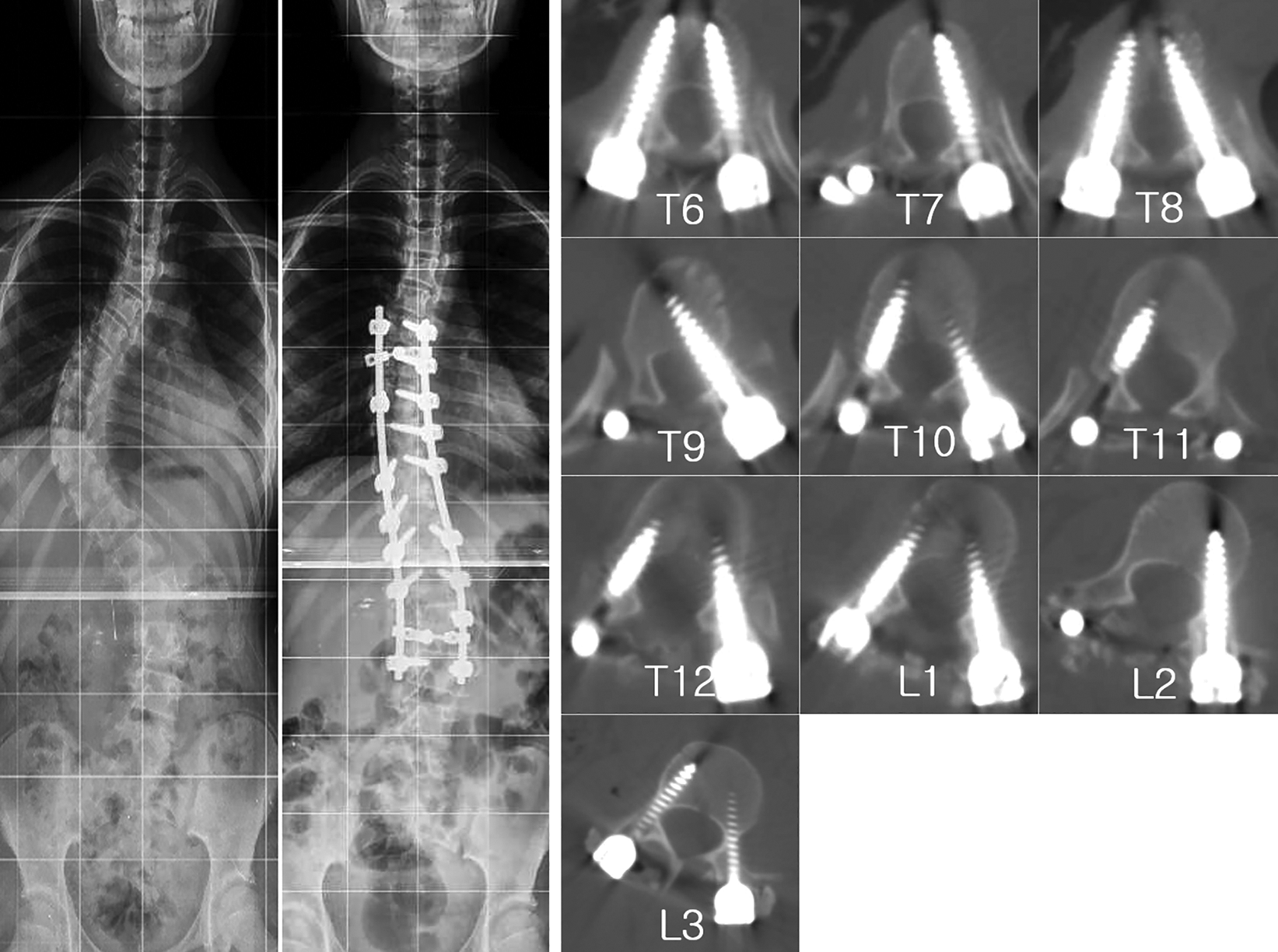
Female, age 16 years, and had double major curve. Cobb’s angle was 72° and 58° and corrected to 24° and 25° postoperatively. One pedicle screw at the T9 level has penetrated medially at the concave side.

Definition of pedicle penetration: (a) medial penetration: penetrated medially over 2 mm; (b) screws were inserted into pedicle properly; and (c) lateral penetration: penetrated laterally over 2 mm.
Results
The EMG thresholds with thoracolumbar pedicle screw stimulation ranged from 6 mA to 14 mA. Intraoperative EMG thresholds of ≤6 mA were shown by 11 screws, which were initially inserted by freehand technique only and reinserted after the confirmation of low-triggered EMG (<5 mA, for all 11 screws), with the resultant final threshold over 6 mA. We used these final resultant thresholds for evaluating the results.
There were 41 total breaches with an overall incidence of 11.1% (41 of 368), which shows that screws penetrated through either medial or lateral wall comprising 5.7% (21 of 368) and 5.4% (20 of 368), respectively (Table 1). The overall breach rate did not attain statistically significant difference (p = 0.59). Nine screws (2.4%) penetrated the anterior wall by an average 2.9 mm (range 0.5–8.1 mm). Breach rate of the concave side was similar to the convex side (group A = 11.0% (28 of 254), group B = 11.4% (13 of 114), p > 0.05). The rate of medial breaches was also similar for both concave and convex side (group A = 5.9%, group B = 6.1%, p > 0.05). No change was identified in the concurrently monitored upper and lower extremity MEP immediately after the deformity correction procedure (rod derotation or cantilever) in any of these patients. No postoperative neurological or vascular complications were noted in any of the patients of both groups. No early or late complications attributable to the thoracic pedicle screw insertion were noted.
Comparison of overall breach rate.

a p > 0.05.
Discussion
Spinal deformity correction using pedicle screw instrumentation, known as the most effective and powerful technique, is becoming the standard treatment option nowadays. Because of the young age and smaller size (sometimes absent) of thoracic vertebral pedicles, the risk for cortical breach is probably greater than that for the lumbar vertebrae. Serious complications by screw malplacement can occur because of the proximity of the neurovascular structures, especially the spinal cord. For these reasons, a reliable method of assessing the position of screws is critically important when applying thoracic pedicle screws in AIS. Among several techniques for pedicle screw insertion, freehand technique is one of the effective methods in terms of reduction of radiation exposure and operative time, for some of the experienced spine surgeons. 11,14
Thoracic pedicle screw placement of concave side of AIS is known to be more difficult than that of convex side screw placement. Smorgick et al. 15 reported a higher breach rate for concave thoracic pedicle screws when compared with the convexity. We believe that it takes a lot of time to learn to place thoracic pedicle screw on the concave side safely through the deformed pedicle, even for an experienced spine surgeon. During the surgery, there are several methods to confirm the accuracy of screw position, such as pedicle wall palpation with a probe, making harmonious arc of the screws, using intraoperative simple radiography, C-arm fluoroscopy, O-arm scan, and triggered EMG. Among those, we rely on freehand technique (anatomical landmark and tactile palpation of pedicle wall) and intraoperatively triggered EMG with final confirmation radiography. For successful insertion of the pedicle screw using freehand technique, exact entry point and palpation of pedicle is the most important part. 16,17
Lehman et al. 17 demonstrated the improved ability to palpate pedicle screw breaches with the probe by the most experienced surgeons. This may in part explain the trend toward a decreased overall breach rate, particularly the medial breaches, seen in the most experienced surgeon group. From our experience, to start gearshift technique of pedicle probing, finding the soft spot of pedicle is very important. Interestingly, this study shows that the overall breach rate did not attain statistically significant difference between group A and B (group A = 11.8%, group B = 10.5%, p = 0.59). The rate of medial breaches was also similar for both concave and convex side (group A = 6.1%, group B = 5.9%, p > 0.05).
The triggered EMG from screw stimulation provides information regarding the physiological effects of screw placement. It estimates the integrity of the vertebral cortex by measuring the intensity of the electrical energy needed to activate the adjacent nerve roots. The stimulus intensity required to activate the nerve root is directly related to the electrical impedance to the passage of current from the screw to the nerve root, which is provided by the intervening structures and most prominently by an intact medial bony cortex of the pedicle. 18 Pedicle screw stimulation has been used for evaluating lumbosacral screws with satisfactory results. 19 In our previous study, we found that the mean range of threshold of the triggered EMG was from 7 mA to 10 mA, which was assessed via the postoperative CT scan. After that, we thought the usual threshold of EMG for AIS patients (over 6 mA) would be safe for assessing pedicle screw fixation. This study also showed that with the combination of freehand technique and triggered EMG which had stimulation threshold greater than 6 mA in AIS patients, thoracic pedicle screws were safe, with the overall reliability of 88.9%. Of course, there are some different reports about triggered EMGs. de Blas et al. 20 reported that the concave and convex sides showed a different EMG threshold range for uncertain screw location. They stated that the threshold values less than 8 mA and 11 mA each in the concave and convex sides, respectively, should be unacceptable. We believe that the difference in threshold values comes from different mean ages of patients at the surgery of each studies (12.8 years in our study and 16.2 years in de Blas et al. 20 ). Furthermore, another study suggested that the triggered EMG threshold for T2–T6 might be different that of lower segments. However, there study was about axillary chest wall electrodes, which were not used in our study. 21
The placement of the convex screws has been known as technically easier than that of the concave side because of anatomical easiness to find the entry point of pedicle and less variation of pedicle morphology. But, in some ways, insertion of the convex screw may be more dangerous than insertion of the concave one, if the surgeon uses routine medial angulation, the screw will be directed into the canal. Preoperative CT scan also can give us information of the trajectory of the pedicle screw.
The percentage of the breached thoracic pedicle screws using the freehand technique and triggered EMG is 11.1% (41 of 368). This percentage comparable to Kim et al. 16 and Lehman et al. 17 is significantly lower than that of the previously reported series of most series. 17,22 –26 Lehman et al 17 found decreased the incidence of fully contained screws between T1 and T8 as compared to T9–T12. However, we did not find any difference in breach rate between the thoracic vertebral levels. Freehand techniques in thoracic pedicle screwing may be familiar to some experienced surgeons. Although there are some superior results of accuracy rate with the navigation or three-dimensional fluoroscopic images, 27,28 radiation hazard and delayed operation time should be concerned.
We would like to suggest that a triggered EMG threshold of >6 mA represented safe screw placement in 88.9% of the screws in AIS patients. The final decision in terms of screw safety should be based on a combination of results of the triggered EMG threshold, the intraoperative radiography, and palpation of the pedicle as well as the operator’s surgical experience.
Conclusion
Freehand technique with triggered EMG which had stimulation threshold of ≥6 mA can safely place thoracic pedicle screw with 88.9% reliability. No statistically significant difference was reported between the concave and the convex sides. According to our present study, information obtained using triggered EMG from pedicle screw stimulation is rapid and useful intraoperatively, and this may help the surgeon determine whether a screw needs to be reevaluated or repositioned to avoid possible postoperative complications to an extent, regardless of the sides of pedicle.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.