
Abstract
Purpose
Surgical site infection (SSI) caused by Propionibacterium acnes is an infrequent but devastating complication after spinal fusion. The purpose of this study was to identify risk factors for SSI with Propionibacterium acnes after spinal fusion for juvenile and adolescent idiopathic scoliosis (JIS and AIS).
Methods
A case-control study was performed. Each case was matched 2:1 for age, gender and diagnosis. Retrospective chart review was performed to obtain relevant demographic, surgical and clinical data for all cases and controls. Statistical analysis included paired t-test and McNemar test, as well as exact logistic regression and robust regression models.
Results
This study included ten infection cases (eight AIS, two JIS) and 20 controls (16 AIS, four JIS). In total, six infected cases presented within two weeks of the index procedure (acute infection) and four infected cases presented more than one year from the index procedure (delayed infection). The most common presentation for acute infections was wound drainage, while back pain was more common in delayed infections. All infections were successfully treated with surgical irrigation and debridement and postoperative antibiotics. Hardware was removed for patients with delayed infections. The strongest risk factor for infection was increased requirement for blood transfusion, but it did not reach statistical significance.
Conclusion
SSI with Propionibacterium acnes is an important complication after spinal fusion for idiopathic scoliosis. These infections can be successfully treated, but larger studies are needed to further identify risk factors and establish standardized guidelines for the treatment and prevention of this complication.
Level of Evidence Level III
Introduction
Spinal fusion is a common treatment for correcting and preventing the progression of spinal deformity for juvenile idiopathic scoliosis (JIS) and adolescent idiopathic scoliosis (AIS). However, this procedure is associated with various postoperative complications, and adverse events following surgery may occur in 3% to 23% of cases.1–6 Surgical site infection (SSI) is an infrequent but devastating complication, and it is the most common reason for readmission following spinal fusion surgery for idiopathic scoliosis.1,7
Several studies have reported the incidence of SSI following surgery for idiopathic scoliosis. Incidence has been reported to range from 0.2% to 9%, but can vary based on patient population, study parameters and definition for SSI (deep versus superficial, acute versus delayed).3,4,6,8,9 A recent study using a large, national, multi-centre database reported a 1.6% incidence of infection (0.6% deep, 1.0% superficial) within 30 days of surgery. 1 While the incidence of acute infection is low, delayed infection is an important but under-recognized complication in the AIS population. Two studies reported a 4.7% to 6.7% incidence of late infection (more than six months after index procedure),8,9 and interestingly, low virulence skin-flora such as Propionibacterium acnes and Staphylococcus epidermidis were cultured in many of these cases. Other investigations reported similar findings.10–13 In a recent study from our institution, we reported a deep infection rate of 1% for AIS patients over a 12 year period. 14 Furthermore, the most common pathogen implicated in infections in patients with idiopathic scoliosis was Propionibacterium acnes. 14 Even though Propionibacterium acnes is traditionally associated with delayed infections, it is now recognized as an important cause for acute infections as well. 14
Many studies have focused on risk factors and prevention of SSI following surgery for idiopathic scoliosis. More specifically, factors such as American Society of Anesthesiologist (ASA) grade, 15 obesity,1,15 use of allograft, 16 length of surgery, 1 number of levels fused, 1 blood transfusion, 11 surgeon factors, 16 prior medical history 16 and use of postoperative drain 16 have been associated with SSIs. However, there is a paucity of literature focusing on risk factors and best practice guidelines for preventing infections with low virulent organisms, particularly Propionibacterium acnes. The purpose of this study is to assess for independent risk factors for the development of SSI with Propionibacterium acnes and to describe the current literature and treatment recommendations for the prevention of these infections.
Patients and methods
We performed a case-control study to identify risk factors associated with the development of Propionibacterium acnes infections in patients with idiopathic scoliosis. First, we identified all patients that underwent spinal fusion for idiopathic scoliosis at our institution between 2000 and 2012 and subsequently developed a SSI. We previously published the details of this cohort, including the overall incidence of SSIs and proportion of SSIs with Propionibacterium acnes in idiopathic scoliosis. 14 We queried our paediatric medicine division and paediatric spine surgeons, and identified additional patients with idiopathic scoliosis that presented with a SSI between 2012 and 2015. Inclusion criteria included age < 21 years at time of index procedure, spinal fusion for JIS or AIS at our institution and treatment for a postoperative SSI at our institution. To ensure a minimum follow-up period of at least one year, patients presenting with a SSI through 2015 were included. All patients underwent posterior spinal fusion, and implant density was determined by patient factors, spinal deformity and surgeon preference. Patients presenting from an outside facility following index procedure for management of postoperative infection were excluded. This study was approved by our institutional review board.
Chart review
We reviewed the charts of all patients that developed a postoperative SSI with Propionibacterium acnes to collect demographic, surgical, infection and microbiology data. A 2:1 control cohort matched by age, gender and diagnosis was also obtained from the initial group of patients described above. These control patients did not develop a SSI after surgery, and chart review was performed to collect demographic and surgical data for these patients as well. We compared the following variables between the cases and controls: body mass index (BMI), surgeon, number of levels fused, ASA grade, length of surgery, use of perioperative antibiotics, surgical site preparation, estimated blood loss, transfusion requirement, use of vancomycin powder, type of lavage (with or without antibiotics), implant material, use of cross-links, use of postoperative drain, length of drain use and length of stay. All of these variables were determined after a literature review of risk factors for SSI after spinal fusion.1,11,15–18 We further reviewed the literature to identify and summarize studies focusing on the diagnosis, prevention and management of Propionibacterium acnes infections in orthopaedic surgery.
Statistical analysis
Descriptive statistics were summarized using means and sds for continuous variables, and frequencies and percentages for categorical variables. The cases and controls were matched for age, gender and diagnosis. Paired t-test and McNemar test were performed to compared continuous and categorical variables between both groups, respectively. Exact logistic regression and robust regression models were used to examine if there are associations between variables and risk of infection. Statistical significance was set to 0.05, and all analyses were performed using Stata 14.0 (StataCorp, College Station, Texas).
Results
Our study included ten patients with SSI after spinal fusion surgery (Table 1). More specifically, six cases of infection were identified from the previous study, 14 and between 2012 and 2015, four additional cases of infection with Propionibacterium acnes were managed at our institution. There were no other cases of infection after spinal deformity surgery in patients with JIS or AIS between 2012 and 2015. In our cohort, nine patients had culture-positive infections with Propionibacterium acnes and one patient had a culture-negative infection that was treated as a presumed Propionibacterium acnes infection. In addition, eight patients had a diagnosis of AIS and two patients had a diagnosis of JIS. The mean age at time of surgery was 15 years (range 13 to 18 years) and there were an equal number of male and female patients. Our control group was comprised of 20 patients (16 AIS, four JIS) matched for age, gender and diagnosis.
Cases of surgical site infection after spinal fusion surgery
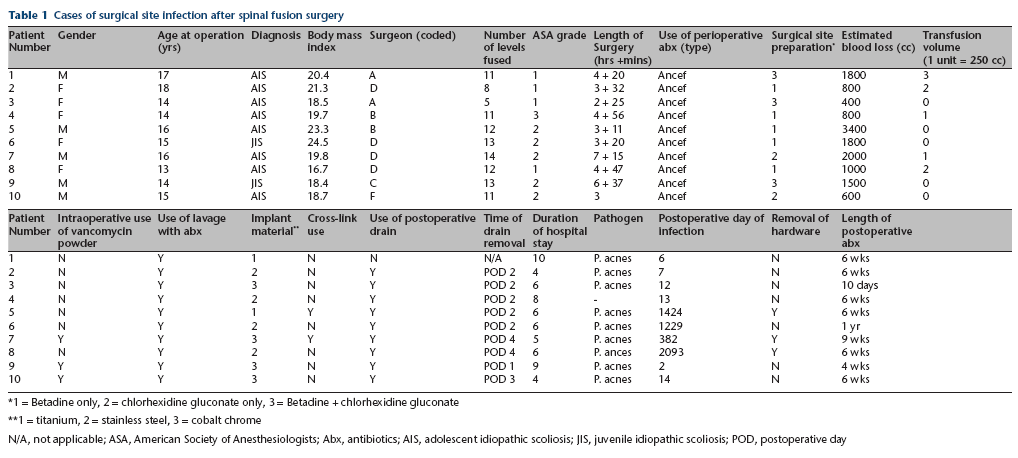
1 = Betadine only, 2 = chlorhexidine gluconate only, 3 = Betadine + chlorhexidine gluconate
1 = titanium, 2 = stainless steel, 3 = cobalt chrome
N/A, not applicable; ASA, American Society of Anesthesiologists; Abx, antibiotics; AIS, adolescent idiopathic scoliosis; JIS, juvenile idiopathic scoliosis; POD, postoperative day
Infection data
Patients with SSI had surgery between 2006 and 2015. Infections were noted in six patients within two weeks of the index procedure (acute infection), and four patients developed infections over one year from the index procedure (delayed infection). No patients had notable back acne or dermatological complaints at the time of their surgical consultation or preoperative visit. The presenting complaint was wound drainage for all acute infections. On the other hand, delayed infections typically presented with complaints of back pain. The most common laboratory abnormalities included leukocytosis in two out of four patients (12 700 and 14 810 white blood cells per mcL) and elevated inflammatory markers in two out of four patients (c-reactive protein (CRP)) 3.6 mg/dl and 6.7 mg/dl, normal < 1 mg/dl). The work-up for delayed infections was comprised of laboratory tests, advanced imaging, and in one case, bone culture and aspiration.
Regardless of acute or delayed presentation, all patients were treated with operative management and postoperative antibiotics. Acute infections were treated with irrigation and debridement, and two patients with acute infections had this procedure during their index admission. Delayed infections were treated with irrigation and debridement as well as removal of hardware in three out of four cases. A robust fusion mass was confirmed on CT scans and intraoperatively in all patients that underwent hardware removal. Intraoperative findings were significant for a hypertrophic soft-tissue reaction around the implant in one patient with a delayed infection; a deep sinus tract with frank purulence in another patient with delayed infection; superficial purulence in one patient with an acute infection; and seroma formation in two other patients with acute infections.
Postoperative antibiotic treatment for acute infections included cephalexin, ampicillin-sulbactam or ciprofloxacin and clindamycin, and duration of treatment was most commonly six weeks, but ranged from ten days to six weeks. Antibiotic treatment for delayed infections was a short course of intravenous antibiotics followed by oral antibiotics (cephalexin or amoxicillin), and the duration of treatment ranged from six weeks to one year. Treatment was successful in all patients in this study.
Variables
Univariate logistic regression analysis was performed to determine any significant risk factors for infection (Table 2). There were no significant differences in BMI, surgeon and number of levels fused between cases and controls (p > 0.05). Similarly, the length of surgery, surgical site preparation and estimated blood loss did not significantly differ between groups (p > 0.05). However, 3/10 infection cases and 1/20 controls required two or more units of blood in the perioperative period (p = 0.15).
Risk factors for surgical site infection after spinal fusion surgery
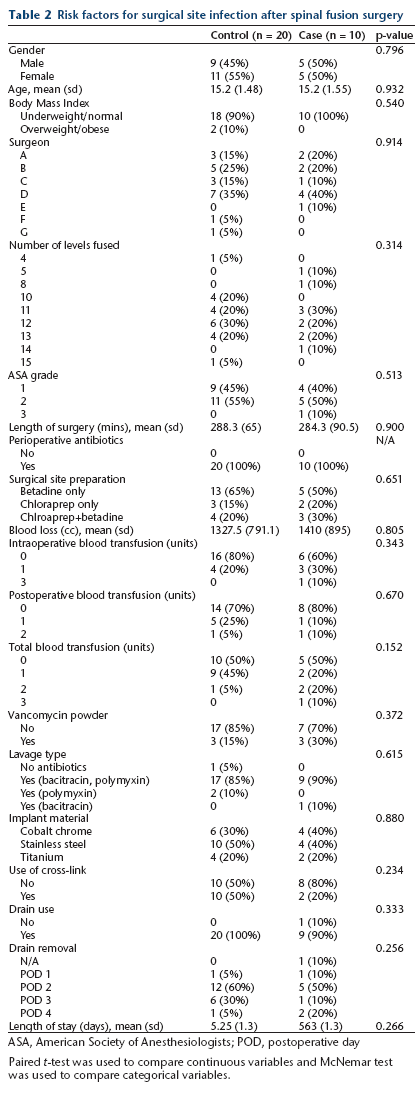
ASA, American Society of Anesthesiologists; POD, postoperative day
Paired t-test was used to compare continuous variables and McNemar test was used to compare categorical variables.
Furthermore, all patients received cefazolin for perioperative antibiotic prophylaxis, and there were no significant differences in vancomycin powder use and antibiotic lavage between groups (p > 0.05). There was also no significant difference in implant material and the use of cross-links between groups (p > 0.05). Drains were placed in almost all cases, and these drains were typically removed on postoperative day (POD) 2 for cases and controls (p > 0.05). After excluding infection cases that underwent irrigation and debridement during the index admission, the mean length of stay did not differ between groups (p > 0.05).
All variables were dichotomized based on their distribution, and odds ratios (OR) were calculated (Fig. 1). ASA grade (Grades 2 and 3) (OR 1.22, 95% confidence interval (CI) 0.21 to 7.85), surgical site preparation (both betadine and chlorhexidine gluconate) (OR 1.68, 95% CI 0.19 to 13.2), use of vancomycin powder (OR 2.35, 95% CI 0.25 to 22.31), intraoperative blood transfusion (OR 2.57, 95% CI 0.36 to 19.25) and length of stay (greater than five days) (OR 2.66, 95% CI 0.36 to 23.88) had the largest ORs for infection. We re-analyzed the data after excluding the patient with a culture-negative infection and found no other significant associations.
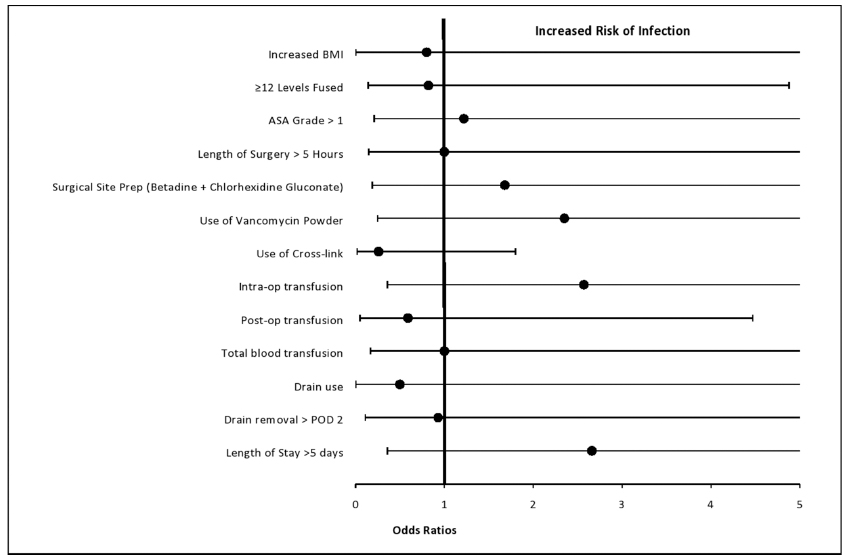
Odd ratios and associated 95% confidence interval for risk factors of infection with Propionibacterium acnes (BMI, body mass index; ASA, American Society of Anesthesiologists; POD, postoperative day).
Discussion
SSI is an infrequent but devastating complication of spinal fusion surgery for idiopathic scoliosis. Propionibacterium acnes is a well described cause of infection in these patients, however, there is limited data on its presentation, risk factors and management. In this study, the most common presentation for acute infections with Propionibacterium acnes was wound drainage, while back pain was more common in delayed infections. All infections were successfully treated with surgical irrigation and debridement followed by antibiotics. We did not find any significant risk factor for the development of infection with Propionibacterium acnes with our sample size. However, factors such as transfusion requirement, surgical site preparation, use of vancomycin powder and length of stay may be implicated, and require additional study.
Propionibacterium acnes is a gram-positive, facultative anaerobe with a slow growth rate and low virulence.19–21 It is part of the skin flora populating the oily pilosebaceous glands of the chest, back, manubrium and ear,22–24 and it is considered an important pathogen in infections following various orthopaedic procedures, particularly in spine and shoulder surgery.8,20,22,25 Due to its deep dermal location, Propionibacterium acnes is relatively sheltered from the standard perioperative antibiotic regimen 26 and surgical skin preparations. 27 Furthermore, it forms a polysaccharide matrix biofilm in the presence of implanted materials, making its eradication difficult without surgical intervention.28,29 Inoculation into the deep wound is believed to occur with skin incision,25,27,30,31 however, other routes such as hematogenous spread, introduction by prior procedure or surgical instrument and provider contamination have also been proposed. 25
Data regarding prevention strategies for Propionibacterium acnes is mostly anecdotal and observational. Strategies suggested in both the spine and shoulder arthroplasty literature include dermatology referral and treatment for skin acne until cleared prior to surgery; adequate skin preparation; tailored prophylactic antibiotics with effectiveness against Propionibacterium acnes; using a new knife for deep dissection; copious irrigation of the field with antibiotic containing saline; usage of titanium implants that may decrease biofilm formation; insertion of implants with new gloves; avoidance of implant contact with skin edge; and avoidance of cross-links that lead to bursa formation.8,25,27,32,33 Our general strategy includes preoperative dermatological referral in the setting of back acne; surgical site preparation with either betadine or chlorhexidine; perioperative antibiotic prophylaxis; meticulous hemostasis; copious irrigation with saline containing antibiotic; and routine use of postoperative drains.
In our study, blood transfusion during the perioperative period trended towards a significant relationship with SSI. Blood transfusion is a recognized risk factor for infection in orthopaedic and non-orthopaedic surgery. A greater number of patients with infections in our study required two or more units of blood in the perioperative period. Our findings are consistent with Ho et al, 11 who found that blood transfusion and increasing units of blood transfusion were associated with infections following posterior spinal fusion for AIS. The increased risk of infection may be due to transfusion-induced immunomodulation, which refers to the relative immunosuppressive effects of blood transfusion. 34 Furthermore, surgical site preparation, vancomycin powder use and length of stay had large ORs but their CIs crossed 1. While previous studies have implicated some of these factors,11,35 larger studies are needed to better understand the relationship between blood transfusion and SSI with Propionibacterium acnes, as well as better elucidate the role of surgical site preparation, vancomycin powder use and length of stay in the pathogenesis of SSIs with Propionibacterium acnes.
Diagnosis of acute infection in our cohort was relatively straightforward as all patients presented with active wound drainage within two weeks of surgery. Meanwhile, delayed infection can present a diagnostic challenge. Each of our patients with delayed infections presented with increasing back pain, necessitating further work-up including labs and advanced imaging to evaluate for collection and fusion mass. This presentation is consistent with the previously described ‘honeymoon period’ of expected prolonged recovery and function, followed by onset of stiffness, pain and spasms.10,25,28 Wound drainage and/or fever are rare presentations for delayed infections.10,36,37 Elevation of white blood cell count and inflammatory markers (erythrocyte sedimentation rate and CRP) were seen in 50% of our patients, but this was variable and has been reported in less than 50% of cases.10,38 Diagnostic imaging modalities, such as MRI and CT, can be invaluable in determining the presence of a collection and assessing bony fusion prior to operative intervention.37,39
Established literature on treatment for Propionibacterium acnes infection in idiopathic scoliosis is sparse. In a study on delayed postoperative infection, Richards et al 8 recommended irrigation and debridement, implant removal, primary wound closure and short-term postoperative parental antibiotic therapy (first generation cephalosporin) followed by oral antibiotics for one to two weeks. Eradication of the protective biofilm was of primary concern and the authors suggested removal of hardware for all delayed infections.8,40 As biofilm formation appears to occur slowly, removal of hardware may not be required in acute infection. 41 Meanwhile, treatment in the total shoulder arthroplasty literature typically consists of irrigation and debridement, intravenous or oral antibiotic treatment and suppression for four to six weeks and one- or two-stage revision. 42 Regional resistance to various antibiotics has been noted, leading investigators to use multidrug programmes often including penicillin or cephalosporin and rifampin. 43 Vancomycin and clindamycin demonstrate only ‘fair’ activity. 44
At our institution, routine perioperative antibiotics are given intravenously within one hour of skin incision, re-dosed after four hours for long cases, and continued for 24 hours after surgery. In the setting of SSI after spinal deformity surgery, our treatment algorithm consists of surgical irrigation and debridement for all acute infections, and removal of hardware for delayed infections. At least four cultures are taken at the time of surgery, and prolonged incubation is performed for all cultures. In the literature, final cultures reported at 72 hours have been found to miss the causative organism, especially for low virulent skin flora like Staphylococcus epidermidis and Propionibacterium acnes.8,9,12 Current recommendations advise culture incubation for at least ten days, 8 and at our institution, we commonly utilize liquid media (thioglycolate) and incubate cultures for 14 days. Postoperative antibiotic coverage and duration is determined in consultation with an infectious disease specialist and is based on culture data, sensitivities, regional microbiodata and relevant literature. In acute infections with Propionibacterium acnes, we typically treat with aminopenicillins or first generation cephalosporins for one to six weeks; and in delayed infections, we treat with intravenous cephalosporins followed by oral aminopenicillins or first generation cephalosporins for a minimum of six weeks. There is considerable variation in the duration of antimicrobial therapy, and additional study is needed to determine the optimal duration of treatment.
Limitations of this study include its retrospective nature and small sample size. However, we employed a case-control study design, which is the optimal design to study rare events, and our study identifies several risk factors to guide future study. Additionally, this study was completed at a single institution, which raises questions about the generalizability of our microbiodata on a regional and national level. Similarly, we did not control for other factors such as the number of levels fused. However, we did not find any significant difference in factors between groups. Furthermore, we compared our cases of Propionibacterium acnes infection with patients without infection, which counts as a drawback of this study. Additional studies comparing cases of infection with Propionibacterium acnes to infection with other pathogens may provide additional insight into risk factors and pathogenesis. Of note, we have had only one SSI in patients with idiopathic scoliosis that has been caused by a pathogen other than Propionibacterium acnes over the study period. This study derives its strengths from the case-control study design with 2:1 controls matched for age, gender and diagnosis, as well as its focus on several risk factors that have been previously hypothesized in the literature. Additionally, it is to our knowledge the first study to describe the diagnosis and treatment of a cohort of patients with idiopathic scoliosis and specifically Propionibacterium acnes infections.
Many advances have been made in the prevention of postoperative infection following surgery for idiopathic scoliosis. However, SSI with low-virulent organisms such as propionibacterium acnes continues to remain an important complication. In this study, we describe the presentation and treatment of a series of acute and delayed infections with propionibacterium acnes. We found no significant risk factors for SSI with propionibacterium acnes, likely due to our limited sample size. SSI with propionibacterium acnes can be successfully treated, however larger studies are needed to better describe risk factors for infection and establish standardized guidelines for the treatment and prevention of this complication.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.