
Abstract
Purpose:
To evaluate the influence of different arm postures from the physiological standing position using force plate analysis of the gravity line.
Methods:
Forty healthy volunteered university students were enrolled. Each subject assumed different standing positions including standing with arms resting on the side (control), with fist over the clavicle (clavicular position), with active shoulder flexion in 30°, 60° and 90° with elbows extended (active flexion A), with hand rest on a bar with a static support (passive flexion P), and with hand rest on a bar with a drip stand (passive flexion D). The offset of the gravity line from the heel was measured by force plate analysis. The offset of the gravity line in different arm positions was compared with the control using paired t-test.
Results:
The mean anterior offset of the gravity line in control position is 39.80% of the foot length. All testing positions showed anterior shift of the gravity line compared with the control position from 0.51% to 7.50%. There were statistically significant changes of the gravity line from the control position in all (p < 0.05), except in the clavicular position (p = 0.249).
Conclusion:
All testing positions cause anterior shifting of the center of gravity from the physiological standing position. Clavicular position is the best comparable posture to the physiological standing position in taking a lateral radiograph. We recommend using the clavicular position as the standard testing position in the assessment of the sagittal profile.
Introduction
Sagittal balance is an important clinical parameter in the management of a spinal problem and has been gaining awareness over the years. 1 –7 A lateral radiograph of the spine has been used in the evaluation of the sagittal profile. In a relaxed standing position, the arms on the sides obscured important anatomical landmarks and the arm is necessary to reposition when taking the lateral radiograph for the evaluation of the anatomical details of the spine. 8 Different arm positions had been suggested by different authors 8 –13 for this purpose. However, repositioning of the arm will change the sagittal alignment of the spine. In our locality, different positions have been used and there is no standard positioning in the evaluation of the sagittal profile. The aim of this study is to evaluate the influence of different arm postures from the physiological standing position using force plate analysis of the gravity line. The “best” arm position for taking the lateral radiograph will be suggested.
Methods and materials
Subject selection
Forty healthy volunteered university students (26 females and 14 males) were enrolled in this study. Inclusion criteria include (1) age between 18 and 30, (2) without previous history of back injury or back pain, and (3) BMI < 26. Consent form was signed before the test and the participants have the right to terminate the test at any point if they wish to do so.
The measurement
Basic anthropometric data including height, weight, and feet length were measured. Reflective markers of 9-mm diameter were attached to the subject using a double-side tape on heels and second metatarsal head of both feet (Figure 1). Data were captured by the Vicon motion monitoring system. Subjects were asked to stand still with feet apart and toes pointing forward.

Measurement of the anterior offset of CG referencing to foot length. CG: Center of gravity.
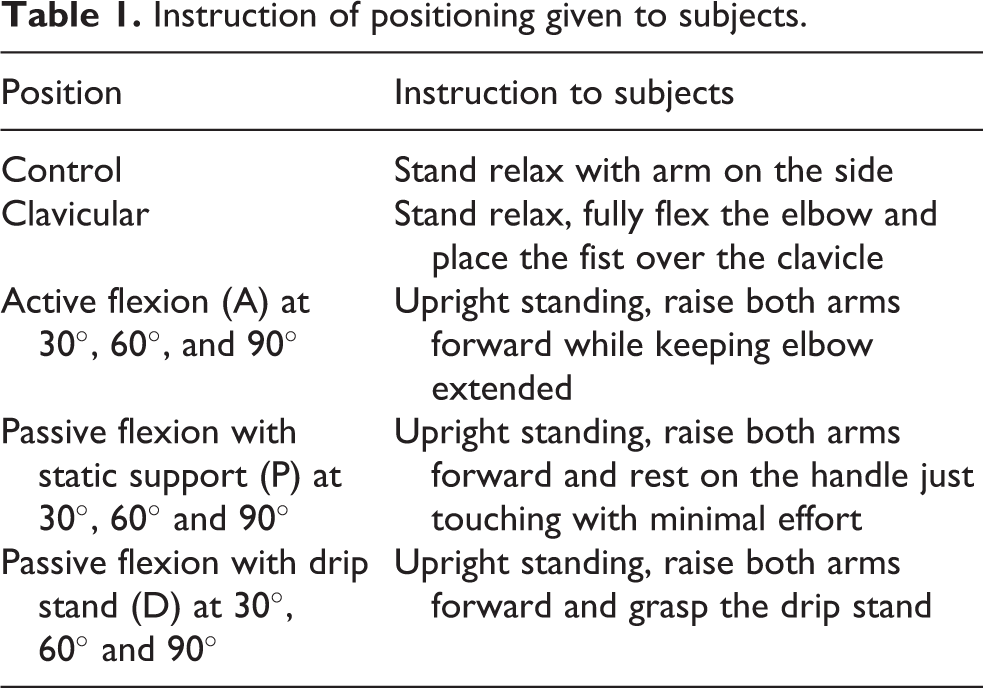
The investigator introduced the testing procedure to the subject with instructions (Table 1) and pictures of different positions (Figure 2) including those described in previous studies 8 –13 : standing with arms resting on either side (control position); standing with fist over the clavicle (clavicular position); standing with active shoulder flexion in 30°, 60°, and 90° with elbows extended (active flexion A); forward arm flexion in 30°, 60°, and 90° with hand rest on a bar with a static support (passive flexion P)—in this position, the patient is advised to rest their hand with minimal transfer of body weight and this is verified by measurement using additional force plate underneath the hand rest; finally, forward arm flexion in 30°, 60° and 90° with hand rest on a bar with a drip stand (passive flexion D). The subjects were instructed to look forward to the end of the laboratory (40 m) to ensure their forward gaze with neutral head position.
Instruction of positioning given to subjects.

Control and testing positions. (1) Control, (2) clavicular position, (3) 30A, (4) 60A, (5) 90A, (6) 30P, (7) 60P, (8) 90P, (9) 30D, (10) 60D, and (11) 90D.
The subject was instructed to perform four static standing trials for each of the above postures in a random sequence. Shoulder positions were verified using a goniometer and the subjects were completely repositioned between each trial. Rest will be given after every five trials. The offset of the gravity line from the heel position is evaluated by force plate analysis (Figure 3), which was measured as percentage as reference to the foot to minimize the effect of different individual’s foot length. The measurements were calculated by averaging the four static trials.

Force plate analysis.
Data processing and statistic
The offsets of the gravity line from the heel in different positions are compared with the control using paired t-test carried by SPSS version 16.0. The level of significance was set at 0.05.
Results
The average age of the subjects was 23.25 years (19–30 years, standard deviation (SD) 2.31 years). The average height and weight were 164 cm (149–182 cm, SD 8.5 cm) and 55.33 kg (41–82.3 kg, SD 10.26 kg), respectively. The average BMI was 20.25 (16.40–25.69, SD 2.34). The mean offset of the gravity line from the heel in the subjects in the relaxed standing control position (control) was 39.80% (SD 7.20) of foot length anterior to the heel (Table 2). All testing positions showed anterior shift of the gravity line (Figure 4) from 40.30% (SD 6.25) to 47.23% (SD 8.00) of the foot length. There were statistically significant differences of the offset of the gravity line from the control position in all arm positions (p < 0.05), except in the clavicular position (p = 0.249; Table 2). There is no statistically significant change of the position of the gravity line with the clavicular position.
Offset of gravity line from the heel (%).

SD: standard deviation.
a p > 0.05.
b p < 0.05.

Anterior offset of CG from heel in different standing positions. *Statistical significance (p < 0.05), #NS (p = 0.249). CG: Center of Gravity; NS: Not significant.
Discussion
The sagittal profile is the conclusion of spine, pelvis, and limb position when an individual stands. Dubousset described the cone of economy referring to the narrow range within which the body can remain balanced, unsupported with minimal effort. 14 This is in turn described as the “stable zone” through which the center of force or the gravity line passed. Despite the great variety of the normative values of the spinopelvic parameters, the gravity line is always positioned at a relatively fixed offset from the heel. 4,5,7,15,16 Lafage demonstrated a difference in the gravity line offset between patients and normal subjects, yet they were relatively constant within the same group. 5
With aging, there were changes in the spinal alignment with anterior shift of the gravity line. 1,4,15,16 This will lead to the recruitment of compensatory mechanisms to resume a more acceptable (economic) functional sagittal balance. 1,5,7,15 –19 These were achieved by retroversion of the pelvis and flexion of the hips and knees. However, further deviation of the gravity line beyond the compensatory limit of the individual will lead to decompensation and the appearance of symptoms eventually. 7,11,20 The ability to recognize the sagittal imbalance and the degree of compensatory mechanism is crucial in the management of a patient with spinal deformity. 5,6,15 –17,21 –23 Moreover, postoperative patients with poor sagittal balance were associated with poor clinical outcome. 6,9,20,24 –27
In taking the lateral radiograph of the spine, arms should be deviated from the resting position for the evaluation of anatomical details. However, different arm positions will cause a change in the sagittal profile from the physiological standing posture, which in turn leads to discrepancy from the true sagittal profile of the individual. 8 Standardizing patient position for the lateral radiograph is of critical importance in terms of the accuracy of measurement, for comparison and communication.
Previous studies 8 –13 have suggested different arm positions in taking the lateral radiograph, including the clavicular position and forward arm flexion of different degrees with or without support (Table 3). Faro studied 50 scoliosis patients with or without surgery, comparing the spinal vertebral axis (SVA) in the clavicular position and active arm abduction at 45°. 8 The SVA shifted posteriorly in both positions but the clavicular position is significantly less deviated. Holton 10 studied 22 scoliosis patients and recommended the fist on the clavicle position over the flexed arm at 60° and 90°. However, his study mainly evaluated the visualization of anatomical landmarks but not the influence on the sagittal profile. Marks compared the changes of the SVA in three arm positions from the functional position of 22 healthy adults using reflective markers to calculate the SVA. 8 There was posterior shift of the SVA in all positions. In passive arm flexion with hand support, there was significantly less posterior shift of the SVA compared with the other position.
Arm positions and recommendations from studies.

AIS: Adolescent idiopathic scoliosis; SVA: spinal vertebral axis.
Aota found less posterior shift of the SVA from the functional position in the clavicular position compared with active arm flexion. 11 He was not satisfied with all tested positions because all were showed to be significantly deviated from the functional position. In his later studies, he recommended the arm in front with the hand-clasped position because it was significantly less deviated compared with other positions. 13 However, like his previous study, all the tested positions showed significant posterior shift of the SVA. Moreover, the arm in front position may have a problem in the visualization of the anatomical details. The vertebral bodies at the thoracolumbar junction were not clearly seen from the X-ray in his published paper.
Some authors have commented that the active arm abduction and the use of drip stand for hand support caused excessive posterior shift of the SVA due to muscle contraction. 10 In this study, we have also tried to evaluate this issue using a static support (position 30P, 60P, and 90P. The testing subjects were instructed to put minimal weight onto the support, which could be detected by the force plate analysis. The 30-degree flexed position with the static support was found to be the most deviated position compared with the control. This can be explained by the complicated instruction to our subjects. This can be even more difficult for our elderly patients if we applied in clinical practice.
It is interesting to recognize the posterior shift of the SVA in most of the previous studies 8,11,13 and we have demonstrated anterior shift of the gravity line offset globally. The posterior shifting of the SVA demonstrated the changes in response to the moment of the weight of the arm. There were increased lordosis and decreased thoracic kyphosis, 11,13 leading to posterior shift of the SVA. The more the influence from the weight of the arm, the more the posterior shift of the SVA is expected. Among different positions in previous studies, the clavicular position is the least outlying position as essentially caused the least change in the SVA. 9,10,12 In our study, we measured the change of the sagittal profile by the gravity line offset through the force plate analysis. All positions showed anterior shift of the gravity line, which is responsive to the anterior placement of the arm that changed the weight distribution of the body. Similarly, the clavicular position as the least outlying position demonstrated the best approximation to the functional standing position (control) with no significant difference, while the rest of the positions were significantly deviated from the control.
For comparison the influence of different positions to sagittal profile, our method using gravity line from force plate analysis is a superior than lateral radiograph as in previous studies. Gravity line offset is the expression of the global sagittal profile in standing but the SAV only evaluates the spinopelvic parameter. Moreover, the force plate analysis of the gravity line is more accurate especially for small changes. The measurement of the SVA from X-ray relies on the projection of the anatomical landmark. This is subjected to the influence of resolution and anatomical variations, with a substantiate level of intra- and interobserver discrepancy. Finally, our subject did not expose to radiation, and we can compare as many postures as possible in the study without causing health hazard. In our study, we can repeat and average the measurement to improve accuracy, and we are able to show the clavicular position has no statistical difference from the functional position. In previous studies, the clavicular position was better but was still deviated significantly from the functional position.
Conclusion
All tested positions cause anterior shifting of the center of force when compared with the functional standing position. Through this explicit and extensive positional evaluation, we concluded that the clavicular position is the best comparable to the functional resting position in taking the lateral radiograph. We recommend using the clavicular position as the standard testing position in the assessment of the sagittal profile.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.