
Abstract
Background:
A previous study on 2-dimensional evaluation of the subtalar joint functioning in varus ankle osteoarthritis concluded that varus deformity was compensated for by the subtalar joint during early stages but not in the advanced stages. Although compensatory function is expected both along the axial and coronal planes, compensatory function in all 3 dimensions (3D) remains unevaluated. This study evaluated the 3D-compensatory function of a varus subtalar joint using Globally Optimal Iterative Closest Points (Go-ICP), a 3D-shape registration algorithm, after 3D-bone shape reconstruction using computed tomography.
Methods:
This study included 22 ankles: 4 stage 2 ankles, 5 stage 3a ankles, 6 stage 3b ankles, and 4 stage 4 ankles, categorized according to the Takakura-Tanaka classification. As the control group, 3 ankles without prior ankle injuries and disorders and 4 stage 2 ankles were included. One control ankle was used as a reference. Relative values compared with the reference ankle were evaluated in each group using Go-ICP. Each axis was set so that dorsiflexion, valgus, and abduction were positive on the X axis, Y axis, and Z axis, respectively.
Results:
Rotation angles of the talus (Rotation T) and calcaneus (Rotation C) on the Y axis in the control and stage 3b were −7.6, −28, −2.1, and −13 degrees, respectively, indicating significant differences. Value of Rotation T-Rotation C (Rotation T-C) represents compensatory function of the subtalar joint. In all ankles, there was a correlation between Rotation T and Rotation T-C on the Y axis and Z axis (P < .01, r = 0.84; P < .01, r = −0.84, respectively). There was a correlation between Rotation T values on the on Y and Z axes (P = .01, r = 0.53).
Conclusion:
In varus ankle osteoarthritis, the talus had varus deformity with adduction. Compensatory function in the coronal plane persisted, even in the advanced stages; however, it was not sufficiently maintained in stage 3b. Furthermore, compensatory function in the axial plane was relatively sustained.
Level of Evidence:
Level III, retrospective comparative study.
Introduction
Ankle osteoarthritis (OA) approximately affects 6% of the population. 6 Functional disability and diminished quality of life associated with end-stage ankle OA are reportedly comparable to those associated with end-stage hip or knee OA.1,12 The most common cause of ankle OA is intra-articular fracture.2,13 Varus ankle OA without prior trauma or general disorder is rare. Although the etiology is unclear, it may be associated with the Japanese lifestyle in which people sit cross-legged or with their legs tucked underneath their body. 14
Radiologic features of varus ankle OA include a characteristic varus deformity combined with anterior opening of the tibiotalar joint and often hypoplasia of the medial malleolus. To date, there have been few reports on the etiology and biomechanics of varus ankle OA. Furthermore, there have been a few reports 5 on the 2-dimensional compensatory function of the subtalar joint using plain radiographs. Varus deformity in the tibiotalar joint is compensated for in the early stages. 5
Although joint alignment has been evaluated using plain radiography and computed tomography (CT) in many studies, it is difficult to evaluate 3-dimensional (3D) relationships. Recently, the evaluation of 3D bone alignment based on principal components analysis (PCA) using image deformation has been reported.3,18 In the proposed method, PCA is used to create a 3D bone model based on bone thickness—which is estimated by Globally Optimal Iterative Closest Points (Go-ICP), a 3D registration algorithm—after 3D bone shape has been reconstructed using DICOM data from weightbearing simulated CT.3,18
We hypothesized that compensatory function would be evident in both the axial and coronal planes. Currently, there are no published reports evaluating 3D compensatory function. This study aimed to evaluate the 3D relationships between the tibia, talus, and calcaneus in patients with varus ankle OA using Go-ICP, a new technique in evaluating 3D bone alignment.
Material and Methods
This study included 19 ankles of 19 patients diagnosed with varus ankle OA who were treated either conservatively or surgically from 2015 to 2018 in our department. The average age was 63±10 (range, 44-73) years. Diagnosis was made using conventional weightbearing ankle radiography for all patients. Each case of OA was then graded using the Takakura-Tanaka classification by 2 orthopaedic physicians. 15 The control group included 3 ankles without prior ankle injuries or disorders. The uninjured and unaffected sides of the patients who were treated either conservatively or surgically for trauma or bone tumors were included as the control group. Patients with stage 2 ankle OA were also included in the control group. Therefore, 3 ankles on the contralateral side of the bone tumor or trauma side and 4 ankles in the stage 2 group were evaluated as the control group. Patients in stage 3a, 3b, and 4 and control groups included 5, 6, 4, and 7 ankles, respectively.
Weightbearing simulated CT with axial loading, using a DynaWell L-spine compression device (DynaWell Inc, Las Vegas, NV), was performed at our institution. The study participants were asked to lie down in a supine position, and pressure was applied from the plantar side using a dedicated plastic board with an adjustment mechanism. The amount of pressure was determined to be 300 N according to the instrument manual.7,8,10,11,16 Cross-sectional areas of the tibia, 50 mm from the tibial plafond, were adjusted in the axial plane on the CT to align all the scans (Figure 1). A perpendicular line was dropped from the central point of the axial tibial slice, 1 cm from the tibial plafond, and the point at which it met the ground was regarded as the origin. The line from this point in the direction of the second toe was defined as the Y axis, the axis perpendicular to this was defined as the X axis, and the proximal tibial shaft direction was defined as the Z axis (Figure 2). Each axis was set such that the direction of dorsiflexion was the positive direction of the X axis, the valgus direction was the positive direction of the Y axis, and the direction of abduction was the positive direction of the Z axis. Quantification using the volume registration method was performed using CT data. The reference ankle bone model in the control group was created by quantifying the difference in bone shape for each participant and using the average of the values. In this study, the volume registration method was used to quantify the difference in bone shape. 18 By overlapping the image of the affected tibiae on that of the tibia of the reference ankle bone model, it was possible to set the same coordinates for all tibiae (Figure 3A). The Go-ICP algorithm was used for the objective and highly accurate matching of each coordinate system.3,18 The difference in the postures of the talus and calcaneus with those of the reference bone was calculated using this algorithm (Figure 3B). Plantar and dorsal flexion, inversion and eversion, and adduction and abduction of the talus and calcaneus were evaluated in each group. In this study, relative values of all affected ankles (in comparison to the reference ankle) were evaluated, not the absolute values. The accuracy and reproducibility of this method has been previously reported in the foot and ankle. 3
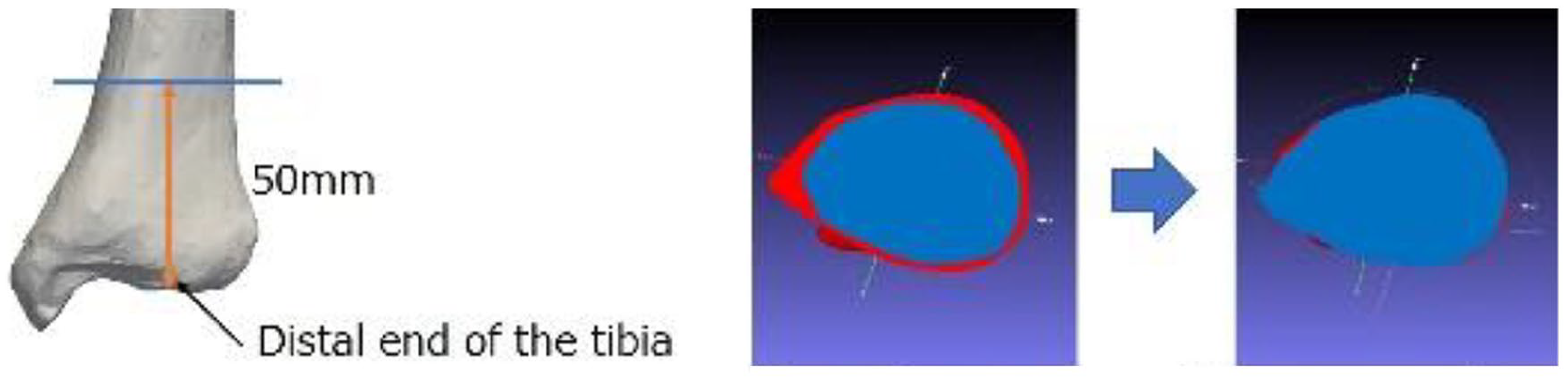
Cross-sectional areas of the tibia, 50 mm from the tibial plafond, were adjusted in the axial plane on the CT to align the scans (red: reference ankle, blue: target ankle)

Figures illustrate the origin (white arrow) and course of each axis: (A) X axis, (B) Y axis, and (C) Z axis.

(A) Overlapping the tibia of the 2 ankle joints with Go-ICP (orange dots: reference joint; black dots: target joint). (B) Amount of change was calculated by overlapping each talus and calcaneus.
Statistical Analysis
First, the normal distribution of data was evaluated using Bartlett test. After the data were confirmed to be normally distributed, a single-factor analysis of variance was used to compare each group. If the data were not normally distributed, the Steel-Dwass test was used. Pearson correlation was used for all ankles, regardless of the group. Statistical significance was set at P <.05. All statistical analyses were performed using Statcel 3 software (version 3; OMS, Tokyo, Japan).
Results
Rotation angles of the talus (Rotation T) in the control, stage 3a, stage 3b, and stage 4 groups were −6.2, −8.5, −5.9, and −4.9 degrees on the X axis; −7.6, −11, −28, and −15 degrees on the Y axis; and −6.8, −15, −18, and −8.6 degrees on the Z axis, respectively; whereas the rotation angles of the calcaneus (Rotation C) were −2.0, −1.5, −0.48, and −5.5 degrees on the X axis; −2.1, −6.7, −13, and −5.3 degrees on the Y axis; and −3.8, −5.6, −2.5, and −7.3 degrees on the Z axis, respectively. Rotation T and Rotation C on the Y axis in the stage 3b group were significantly lower than those in the control group (Tables 1 and 2, Figure 4).
Rotation Angle of the Talus.

Rotation Angle of the Calcaneus.


(A) Rotation angle of the talus on the Y axis in different stages. (B) Rotation angle of the calcaneus on the Y axis in different stages.
Rotation T-Rotation C (Rotation T-C) represents a compensatory function of the subtalar joint. In all ankles, there was a correlation between Rotation T and Rotation T-C on the Y axis (P < .01, r=0.84; Figure 5). On the Z axis, there was a correlation between Rotation T and Rotation T-C (P < .01, r= –0.84; Figure 6). There was a correlation between Rotation T on the Y axis and Rotation T on the Z axis (P = .01, r = 0.53; Figure 7).
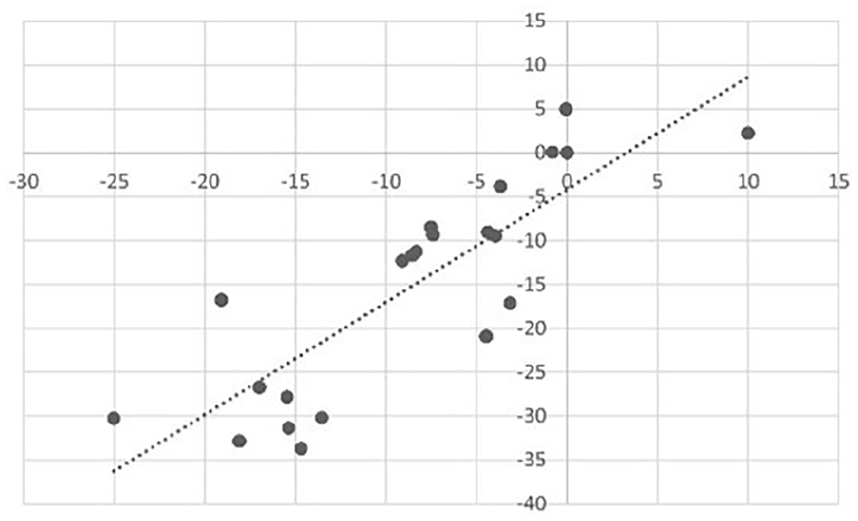
Correlation between the rotation angle of the talus (Rotation T) and Rotation T-C on the Y axis.
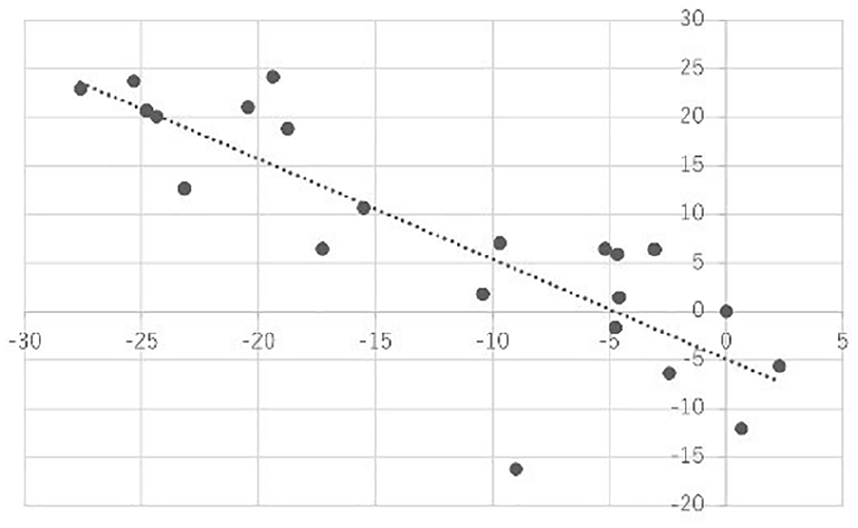
Correlation between Rotation T and Rotation T-C on the Z axis.

Correlation between Rotation T on the Y axis and Rotation T on the Z axis.
Discussion
Little is known about the etiology of varus ankle OA. Dysfunction of lateral ligaments, such as the anterior tibiofibular and calcaneofibular ligaments, impairs the sagittal, coronal, and transverse joint stability, resulting in a tendency for varus tilt and anterior translation of the talus in the tibiotalar joint.4,9
Regarding the compensatory function of the subtalar joint for varus deformities of the tibiotalar joint, Takakura 14 speculated that the subtalar joint may have some ability to compensate and this ability may prevent ankle OA progression. Based on their observations of a relatively small cohort with end-stage ankle OA, they postulated that ankle OA may progress after the subtalar compensatory function is lost. 14 Hayashi 5 documented the subtalar joint inclination at varus ankle OA using plain radiography. They concluded the following mechanism. As the varus deformity of the tibiotalar joint progresses, the simultaneous compensatory function (valgus inclination) of the subtalar joint does not concentrate the weightbearing stress on the medial side of the ankle. However, the breakdown of the compensatory function leads to the varus inclination of the subtalar joint. The medial stress concentration in the ankle increases, and the varus ankle OA progresses to the end stage. 5 However, Bibo reported that even in patients with end-stage ankle OA, those with mild or no degenerative changes of the subtalar joint may compensate for the ankle malalignment, resulting in a neutral hindfoot alignment. 17 The importance of assessing the subtalar joint was described.
These previous reports have only evaluated the compensatory function of varus and valgus using plain radiographs, and there are no reports on 3D evaluation, including adduction and abduction of the hindfoot. In this study, we evaluated the 3D alignment based on bone thickness using PCA. Ankle OA could be evaluated with high accuracy by creating a 3D bone model as a reference. In addition, using the Go-ICP algorithm, it is possible to assign the same coordinates for all bones to be analyzed, and data can be acquired with high objectivity. Although Go-ICP is a relatively new technique, its effectiveness in evaluating the ankle joint has been reported. 3
In this study, there were no significant differences in the talus or calcaneus between the groups in the X axis. Moreover, the alignment of the dorsal and plantar flexion was retained regardless of the stage.
As the talus and calcaneus were significantly angled inward in relation to the Y axis in the stage 3b group, varus deformity in the tibiotalar joint was not sufficiently compensated by the subtalar joint in the stage 3b group. However, a positive correlation between Rotation T-C and Rotation T on the Y axis was indicated, and the compensatory function of the subtalar joint was not lost, regardless of the stage or condition of the subtalar joint, which is different from previous reports. As the varus deformity of the tibiotalar joint progressed, the compensation function could not be maintained, resulting in the misalignment of the hindfoot due to the progressed varus deformity of the tibiotalar and subtalar joints.
In all cases, Rotation T on the Y and Z axes showed a positive correlation. The talus had varus deformity with adduction. There was no significant difference in the talus or calcaneus on the Z axis between the groups. As shown by the negative correlation between Rotation T and Rotation T-C on the Z axis, it was found that the adduction deformity was compensated.
This study had some limitations. First, the sample size was small, which compelled us to include stage 2 ankles with near normal bone alignment in the control group. Second, although weightbearing cone beam CT is now available, we used weightbearing simulated CT with axial loading, using a DynaWell L-spine compression device. In terms of radiation dose and economics, this method may not be preferred. When total ankle arthroplasty or arthrodesis is performed for ankle OA, the condition of the adjacent joints, such as the subtalar joint, plays a significant role in the clinical outcome. Similarly, the compensatory function of the subtalar joint is important when conservative treatment with a lateral wedge insole is indicated. The results of this study are expected to be useful in clinical practice.
In conclusion, the 3D compensatory function of the subtalar joint using Go-ICP in patients with varus-type ankle OA was evaluated. The talus had varus deformity with adduction. The compensatory function in the coronal plane was sustained, even in the advanced stages; however, it could not be sufficiently maintained in stage 3b. Furthermore, compensatory function was relatively sustained in the axial plane.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114221103584 – Supplemental material for Evaluation of Subtalar Joint’s Compensatory Function in Varus Ankle Osteoarthritis Using Globally Optimal Iterative Closest Points (Go-ICP)
Supplemental material, sj-pdf-1-fao-10.1177_24730114221103584 for Evaluation of Subtalar Joint’s Compensatory Function in Varus Ankle Osteoarthritis Using Globally Optimal Iterative Closest Points (Go-ICP) by Hiroaki Kurokawa, Shinichi Kosugi, Takuya Fujinuma, Yuya Oishi, Takuma Miyamoto, Akira Taniguchi, Hiroshi Takemura and Yasuhito Tanaka in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Nara Medical University (IRB No. 848). An opt-out statement regarding the application of medical data was published on our institute’s website and the participants were given the option to opt out. This study was conducted in accordance with the principles of the World Medical Association Declaration of Helsinki.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.