
Abstract
Purpose:
The aim of this study was to assess the diagnostic accuracy of swab polymerase chain reaction (PCR) compared with tissue culture as the current gold standard.
Methods:
Forty-one consecutive patients were prospectively enrolled undergoing revision arthroplasty due to septic and aseptic reasons. Infection classification was done according to the criteria of the Musculoskeletal Infection Society. Intraoperatively, tissue samples of the periprosthetic membrane were collected for culture analysis, and swabs were taken from the accessible implant surface to perform 16S ribosomal RNA PCR. The diagnostic performance of swab PCR and tissue cultures was determined.
Results:
Of the 41 patients, 53.7% (n = 22) had a periprosthetic joint infection (PJI) and 46.3% (n = 19) an aseptic loosening. Swab PCR showed a higher sensitivity than tissue cultures (86.4% vs. 68.2%), while the specificity was equal (89.5%). The area under the curve was 0.79 for tissue cultures and 0.88 for swab PCR.
Conclusions:
In this first investigation of swab PCR for diagnosing PJI, this procedure revealed a higher sensitivity for diagnosing PJI compared with tissue cultures. Because swab PCR is easily implementable and does not require special equipment, it can potentially improve the diagnosis of PJI.
Keywords
Introduction
Periprosthetic joint infection (PJI) is a serious problem in orthopaedic surgery that accounts for high patient morbidity and considerable healthcare costs. 1 The incidence is approximately 1% after primary arthroplasty. 2 Differentiation between chronic PJI and aseptic prosthesis loosening can be challenging because typical clinical signs of infection may be absent and laboratory presentation can sometimes be similar in both entities. Because there is no diagnostic test with absolute accuracy, typical case definitions for PJI comprises a set of parameters including clinical, laboratory, microbiological, histopathological and synovial fluid findings. 3,4 The identification of a causative pathogen is of particular importance in order to initiate a targeted antibiotic therapy in addition to the surgical treatment. In this context, molecular methods, such as polymerase chain reaction (PCR), have come into the focus of intensive research because they may identify small amounts of bacterial DNA and, thus, are supposed to have a higher sensitivity. 5 However, PCR has not been implemented into clinical practice yet. This is, at least in part, due to uncertainties regarding the choice of the PCR-based method (specific, broad range, multiplex, etc.) and the type of sampling (synovial fluid, tissue, sonication fluid, etc.). Although swabs are known to have inferior diagnostic accuracy in culture methods, 6 they have not been evaluated as specimens for PCR to detect PJI. The purpose of this study was to assess the diagnostic accuracy of swab PCR in the diagnosis of PJI and to compare it with tissue cultures as the current gold standard. We hypothesized that swabs of the implant surface will yield sufficient amount of bacteria for PCR to have a good diagnostic accuracy for detecting PJI.
Materials and methods
Approval for this study was obtained from our Institution’s Ethics Committee (#5544). Patients gave their informed consent prior to the experiments.
Study design
We prospectively enrolled consecutive patients who underwent revision arthroplasty from January 2013 to December 2015 in our institution. Indications for revision surgery were septic and aseptic. Medical history including demographic data, comorbidities and clinical presentation was recorded. Prior to surgery, synovial fluid was aspirated for the evaluation of white blood cell (WBC) count and percentage of polymorphonuclear cells(%PMN). Blood specimens were taken to assess serum C-reactive protein (CRP) and peripheral blood leucocytes. Intraoperatively, tissue samples of the periprosthetic membrane were collected for culture analysis. Prior to prosthesis removal, swabs from the accessible implant surface were taken using sterilized foam pellets (ORBIS Dental, Münster, Germany). Only patients with a complete set of data were included in this study.
Periprosthetic joint infection
PJI was assumed according to a modified consensus classification of the Musculoskeletal Infection Society (MSIS) when one of the following parameters was fulfilled
3,4,7,8
: sinus tract or open wound in communication with the prosthesis; at least two tissue cultures tested positive for the presence of the same pathogen and the presence of the following four criteria: elevated CRP (>10 mg L−1), elevated WBC (>1700 µL−1 in knees and >3000 µL−1 in hips), elevated %PMN (> 64% in knees; >80% in hips) and intraoperative purulence.
16S rRNA PCR
For extraction of bacterial DNA, swabs were incubated for 30 min at 37°C in a lysis buffer containing 20 mg mL−1 lysozyme in 2 mM ethylenediaminetetraacetic acid, 20 mM Tris hydrogen chloride and 1.2% Triton X-100 at pH 8. Following proteinase K digestion, the suspension was homogenized (Omni Inc, Kennesaw Georgia, USA) using a Precellys 24 bead mill and 0.5-mm glass beads (6500 r min−1, 3 × 20 s and 15-s interval).
Fragments of bacterial genome with a length of about 500 bp were amplified by PCR using the universal primers 27f (5′-AGAGTTTGATCMTGGCTCAG-3′) and 5′-phosphorylated 521revP (5′-ACCGCGGCTGCTGGCAC-3′), targeting the hypervariable regions V1 and V3 within the 16S ribosomal RNA (rRNA) gene. The PCR mix contained 50 ng of template DNA, 200 nM of each primer, PCR buffer, 1.5 U HotStarTaq polymerase and 200 mM of each deoxynucleotide triphosphate in a total volume of 50 µL. Thirty amplification cycles were performed, including denaturation at 94°C for 1 min, annealing at 52°C for 40 s and elongation at 72°C for 1 min. The PCR products were purified using the QIAquick PCR Purification Kit according to the manufacturer’s description (Qiagen, Hilden, Germany). Subsequently, electrophoresis was conducted on agarose gel (1.2%) with genomic double-stranded DNA of each specimen.
Following sequencing of the amplicons, the results were checked using the BioEdit software package v7.0.9 (Ibis Biosciences, Carlsbad, CA, USA). A comparison was made to the database from the National Center for Biotechnology Information (NCBI), and the best matches were identified using both the Basic Local Alignment Search Tool (BLAST) and the SEQMATCH Tool from the Ribosome Database Project.
Statistics
Continuous variables (age, peripheral blood leucocytes, CRP, WBC and %PMN) were checked for normal distribution using the Shapiro–Wilk test and presented as mean ± standard deviation. In all cases, a normal distribution was proved, and an independent samples t-test was used to compare the above-mentioned data for infected and non-infected arthroplasties. Categorical variables were reported as percentages and compared with the Fisher’s exact test. For swab PCR and tissue cultures, the sensitivity, specificity, positive predictive value, negative predictive value, accuracy and area under the receiver operating characteristic curve (AUC) were calculated.
A p-value of <0.05 was considered to be statistically significant. The SPSS program (SPSS 22.0, SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
Results
A total of 41 patients were included in this study; of these, 53.7% (n = 22) accounted for infected patients, while the remaining 46.3% (n = 19) did not fulfil the criteria of the MSIS. We did not find any significant difference between these groups for age, gender, comorbidities and distribution of total hip and total knee arthroplasties. Nine patients had sinus tracts in communication with the prosthesis, while 14 patients had at least two tissue cultures tested positive for the presence of the same pathogen. Purulence in the affected joint was evident in 11 patients. CRP and %PMN were significantly higher for the infected group. The preoperative baseline characteristics of the patients and perioperative data are presented in Table 1.
Characteristics of the analysed subjects.

CRP: C-reactive protein; WBC: white blood cells; %PMN: percentage polymorphonuclear cells; PCR: polymerase chain reaction.
Test characteristics are summarized in Table 2. Swab PCR showed a higher sensitivity than tissue cultures (86.4 vs. 68.2%), while the specificity was the same (89.5%). Accordingly, the AUC was higher for the swab PCR (Figure 1). The gram-positive and gram-negative microorganisms isolated by swab PCR and tissue cultures are presented in Table 3.
Diagnostic performance of tissue culture and swab PCR.
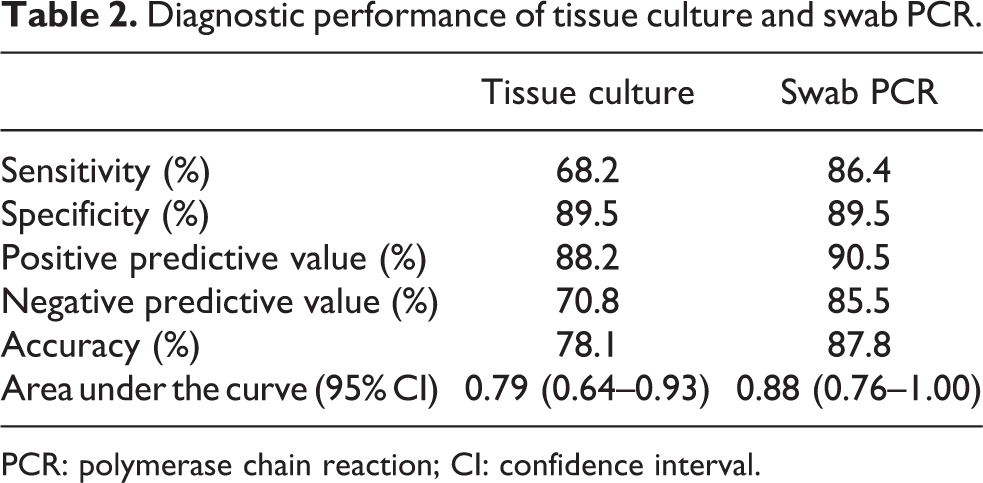
PCR: polymerase chain reaction; CI: confidence interval.

ROC curves of the specificity and sensitivity of tissue cultures and swab PCR for diagnosing PJI. ROC: receiver operating characteristic; PCR: polymerase chain reaction; PJI: periprosthetic joint infection.
Organisms isolated in the 22 infected arthroplasties.
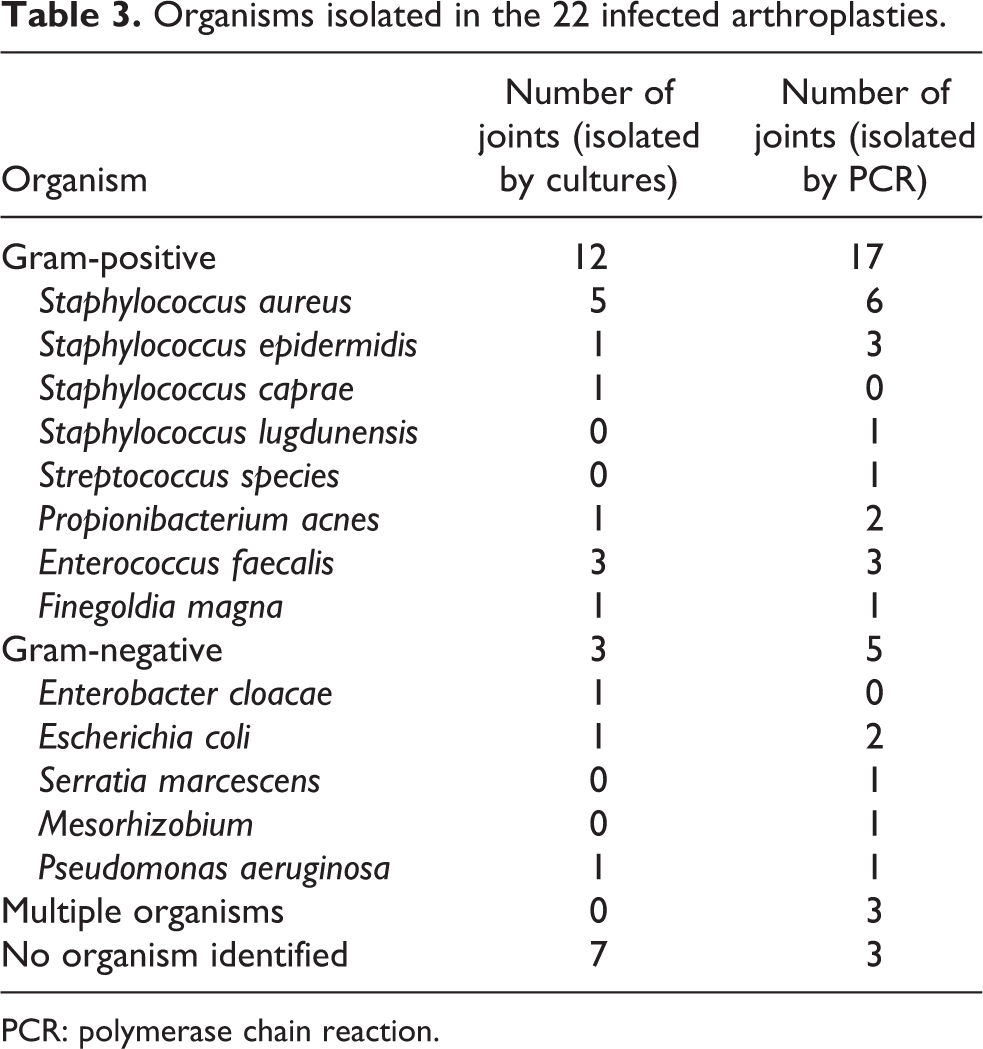
PCR: polymerase chain reaction.
Discussion
The main finding of this study was that swab PCR revealed a higher sensitivity for diagnosing PJI compared with tissue cultures. Especially patients undergoing revision surgery with implant retention may benefit from this diagnostic procedure, because this method is not tissue consumptive and does not require implant removal.
While acute PJI is normally easy to detect due to distinct clinical presentation caused by high virulent pathogens, the diagnosis of chronic PJI can be challenging. The explanation may be twofold. First, bacteria are predominately attached to the implant surface and surrounded by a biofilm, thus making dislodgement for diagnostic purposes very difficult. Second, bacteria that are responsible for chronic PJI are typically low virulent and low replicative. These pathogen-related characteristics complicate detection by culture-based methods, which require a critical bacterial load for induction of growth. 9 Growing evidence has shown that PCR-based methods have a higher sensitivity than culture because they are theoretically capable of detecting a single bacterial DNA molecule. This was previously shown for different specimens including sonication fluid 10 –12 and tissue. 13 –17 However, PCR is considered to be prone to false-positive results through detection of contaminating bacteria or primer cross-reactivity. 18
The results of diagnostic tests for PJI generally depend on the sampling procedure. 18 For culture methods, it is assumed that swabs have an inferior diagnostic accuracy than tissue. Aggarwal et al. reported, in a prospective study with 117 cases, a sensitivity of 63% versus 53% and a specificity of 98% versus 98% for tissue versus swab cultures, respectively. 6 These findings were also supported by Font-Vizcarra et al. who in their retrospective study of 150 cases found a superior sensitivity of tissue (69%) to swab cultures (61%). 19 In contrast, they determined a decreased specificity of tissue (81%) compared with swab cultures (99%). Compared with the studies of Aggarwal et al. and Font-Vizcarra et al., 6,19 tissue cultures performed similarly in the current study (sensitivity 68% and specificity 90%), while swab PCR (sensitivity 86% and specificity 90%) yielded superior results to swab cultures. It is conceivable that the improved results of swab PCR are due to a lower detection limit of PCR-based methods. As discussed earlier, a major problem is to dislodge the bacteria from their biofilm on the implant surface. Unlike with cultures, swabbing seems to yield a sufficient amount of bacteria for PCR-based methods.
The shortcoming of insufficient bacterial yield for diagnosing chronic PJI is one of the driving forces of research in the field of sampling. Sonication fluid is considered as a promising specimen, either for culture or for PCR; however, it has not been implemented routinely into clinical practice yet. 20 Studies that evaluated sonication fluid PCR for diagnosing PJI found sensitivities ranging from 70% to 96% and specificities ranging from 97% to 100%. 10 –12 This is comparable to the results of the current study for swab PCR (sensitivity 86% and specificity 90%). In contrast to swabs, producing sonication fluid requires considerable personnel and technical efforts and has an increased risk of contamination during processing. 11,21 Moreover, for sonication, it is obligate to remove the prosthesis that is not always possible or intended. 22,23
Tissue samples, currently considered as the specimen of choice for pathogen detection, yielded variable results when investigated using PCR-based methods. Studies revealed a wide range of sensitivities from 16% to 90% and specificities from 45% to 97% for diagnosing PJI. 13 –17,24 The results are at least in part explained by the different applied PCR methods but also ascribable to the low concentration and unequal distribution of bacteria in the surrounding tissue. 9,18 As bacteria are predominantly located on the implant surface in multiple aggregates, specimen collection from the implant surface using swabs seems to be reasonable but requires standardized protocols. In the current study, the accessible implant surface was completely swabbed prior to prosthesis removal. Although this procedure may relevantly be biased by the surgeon, this first investigation of swab PCR in diagnosing PJI revealed promising results, making further elucidation desirable.
There are several limitations to this study. First, the sample size was relatively low implying that the results should be regarded as preliminary. Second, the study population was inhomogeneous and comprised of hip and knee prostheses, which have different diagnostic thresholds in terms of synovial fluid analysis. Moreover, questions remain unanswered regarding the optimum swab material, the number of specimen and the region of specimen obtainment.
This study has also important strengths, including completeness of the data and detailed clinical information. To the best of our knowledge, this is the first study analysing swab PCR as a diagnostic tool to detect PJI.
Conclusion
In this first investigation of swab PCR for diagnosing PJI, this procedure revealed a higher sensitivity for diagnosing PJI compared with tissue cultures. Swab PCR is easily implementable and does not require special equipment. Moreover, it can be performed in revision arthroplasty with implant retention as well as with implant removal. Due to the limited sample size of the current analysis, further studies are warranted to elucidate the value of swab PCR in the diagnosis of PJI.
Footnotes
Acknowledgement
The authors thank Rainer Schreeb for his excellent technical help.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants of Hoschulinterne Leistungsförderung of Hannover Medical School, Traumastiftung and Axis-Forschungsstiftung.