
Abstract
Background/purpose:
Total hip arthroplasty is a safe, cost-effective surgical intervention which restores mobility and alleviates pain from most kinds of hip arthritis. The proposed biomechanical study evaluates the effect of the stem size on the mechanical environment of the hip and its association with aseptic loosening.
Methods:
Medium left, fourth-generation, composite femoral models were used, and different prosthesis dimensions were examined. Fourteen strain gages were placed at specific positions on the femur. Load cycles were programmed to simulate single-leg stance of gait of a normal-weight subject.
Results:
Microstrains in the anterior and posterior region of the femur shaft were found to decrease with increasing the stem length, while no specific tendency was observed in the regions of the great and lesser trochanteric as well as in the medial and lateral femur.
Conclusion:
This study indicates that shorter implants are subjected to higher strains distally to the pertrochanteric area.
Introduction
Total hip arthroplasty (THA) is a safe and cost-effective surgical intervention which restores mobility and alleviates pain from most kinds of hip arthritis improving the quality of a patient’s life. Several research groups have investigated the implant status after a THA and the risk of failure due to aseptic loosening. Various parameters have been examined such as different implant designs, 1,2 loading conditions, 3 –6 and patient characteristics. 7 The stem length could be a potential factor associated with loosening and has been addressed by several clinical, animal, and experimental studies with controversial results. 8 –13
Specifically, the use of short femoral stems has several advantages such as that they are less invasive due to less loss of femoral osseous tissue, patient experience less pain, and there is less stress shielding on proximal femurs. 8 However, it has been found that shorter stems lead to higher cement strains that may increase the risk for aseptic loosening, and patients with stable implants have larger stem sizes and lower bone to stem ratios that those with loose implants. 9,10
Despite the fact that several studies have addressed the impact of femoral stem length on aseptic loosening, no safe conclusion can be drawn. On the other hand, there is an absence of biomechanical studies addressing the association of the stem length with strain distribution in the published literature. Moving forward beyond the state of the art in this research field, in the present biomechanical study, we aimed to evaluate the developed microstrains at different receiving positions of composite femoral bones by changing the length of a specific stem design.
Materials and methods
Model geometry
In this study, we used custom-made, commercially available, medium left, fourth-generation, composite femoral models for biomechanical testing (Sawbones, Pacific Research Laboratories, Vashon Island, Washington, USA) which are shown in Figures 1 and 2. More specifically, the cortical bone consists of short fiber-filled epoxy (density: 1640 kg/m3, compressive strength: 157 MPa, modulus of elasticity: 16.7 GPa) and the cancellous bone of rigid polyurethane foam (density: 270 kg/m3, compressive strength: 6 MPa, modulus of elasticity: 155 MPa).
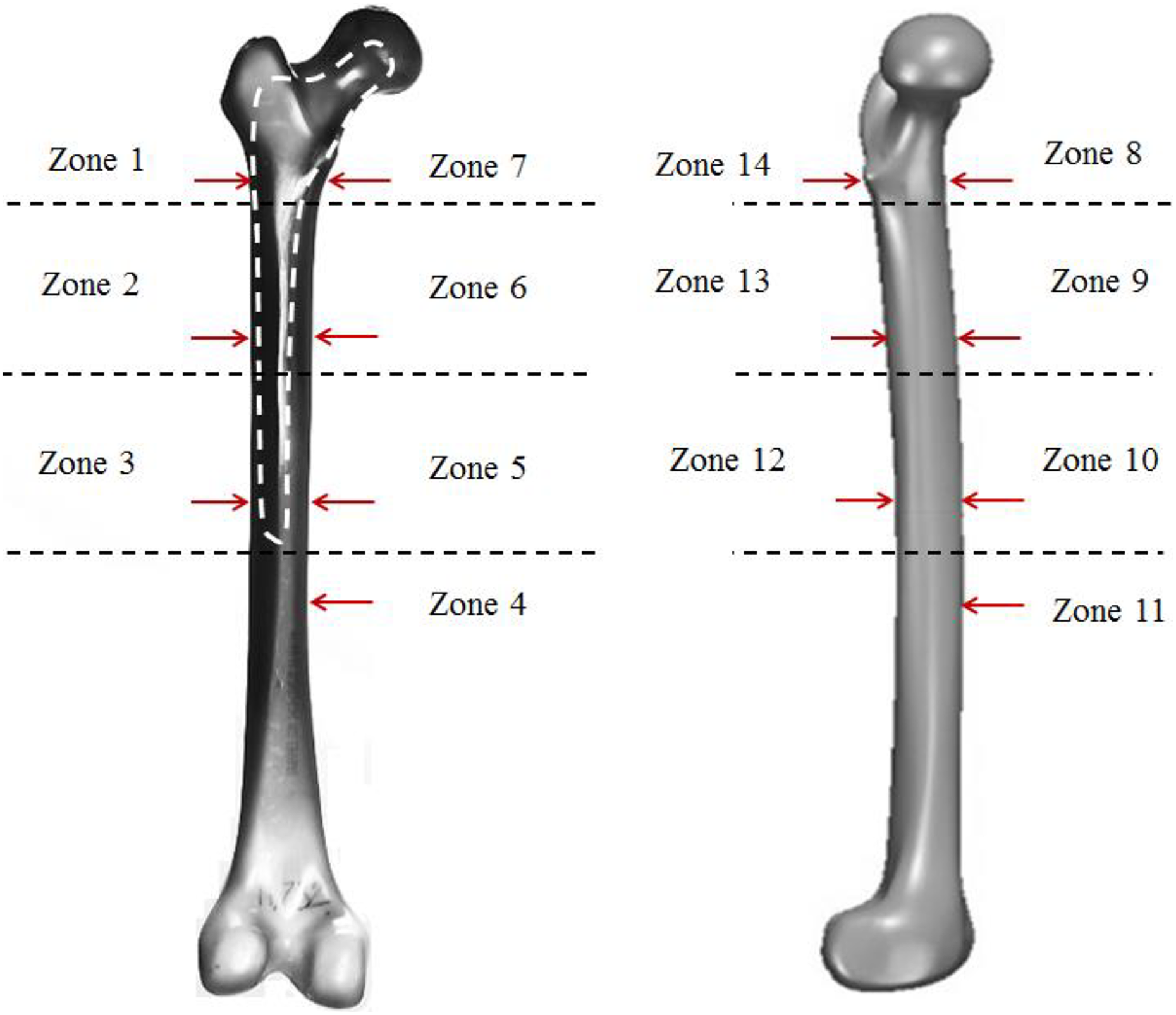
Schematic overview of the medium left, fourth-generation, composite femoral models, and definition of stem surface zones corresponding to radiographic Gruen zones. The red arrows illustrate the position of the 14 strain gages.

Experimental setup.
A CLS spotorno Stem (CLS® Spotorno® Hip Stem, Zimmer (http://www.zimmer.co.uk/)) was used. The tapered shape of this stem (a) enables excellent primary stability; (b) ensures that the stability is maintained, thanks to the self-stabilizing properties of the implant; and (c) favors a largely proximal transfer of load. The initial length of the prosthesis was 13.75 cm, which was then cut to perform experiments for the stem lengths 12 and 11 cm. The stem consisted of Ti-6Al-7Nb (Protasul-100), which is a titanium alloy featuring high strength, low weight ratio, and good corrosion resistance (modulus of elasticity: 110 GPa, Poisson’s ratio: 0.37).
More specifically, the bones were osteotomized and specifically machined for use by an orthopedic surgeon according to the procedure recommended by the manufacturer. The biomechanical femur was secured with a clamp (DREMEL #220076 D-VISE) in the vertical position to prepare the canal for the implantation. A standard neck osteotomy was performed with a reciprocating saw. Subsequently, the rasping technique as provided by the manufacturer was used to prepare the femoral canal for the stem implantation. In all composite bones, a size 8 of the CLS Spotorno Stem was used.
Boundary conditions
In Figure 2, the experimental setup is presented based on the study of Politis et al. 2 A custom-made fixture designed to reproduce loading conditions during the single-leg stance phase of walking was attached to the load cell of a computer-controlled hydraulic testing machine (MTS 858 Mini Bionix, MTS Systems Corporation, Eden Prairie, Minnesota, USA) according to McLeish and Charnley. 14 The femur was tilted into 12° of valgus and was positioned neutral on the sagittal plane. Hip abductors were simulated by a small chain attached to a custom-made base that was fixed to the lateral aspect of the greater trochanter. The abductor force simulation applied the load at an angle of abduction 15° to the sagittal plane. 14,15 The distal end of the femur was embedded in a steel pot with an appropriate polymer (polyester). A modified universal ball joint was mounted between the distal construct and the base of the machine.
Load cycles were programmed to simulate single-leg stance of a normal-weight subject. Applying a vertical force five-sixths of the body weight, with the weight of the lower extremity subtracted, would yield a physiological resultant hip joint force in the hip simulator. 16 An axial load of 600 N was applied to simulate the single-leg stance of a subject weighing 73 kg. A three-step testing sequence was used as follows: (1) ramp-up to −300 N (rate 100 N/s), (2) sinusoidal axial loading between −100 N and −600 N applied at a frequency of 1 Hz for 200 cycles, and (3) ramp-down to −50 N (rate 500 N/s). The material testing system operated under force control. Load cell limit was set at −750 N.
Strain gages
To measure the microstrains on the femur during single-leg stance of gait, 14 uniaxial 120-Ω strain gages (KYOWA, KFC-5-C1-11L300, Kyowa Electronic Instrument, Tokyo, Japan) were positioned on critical stress points of the femur. As illustrated in Figure 1, the concept of Gruen femoral zones was used for the evaluation of radiographs for signs of loosening. 17,18 The strain gages were placed on predefined positions in each one of the seven Gruen zones (Figure 1).
The leads of the gages were connected to a Wheatstone bridge configuration (KYOWA SS-24R Switching and Balancing Box, Kyowa Electronic Instrument). The gage outputs were transferred to a signal amplifier module and consequently to a data acquisition system (MTS TestStar II®, MTS Systems Corporation). Finally, during gait simulation, a computer connected to the acquisition system recorded all the microstrain measured data on 5-ms intervals. Prior to testing, the abductor chain was pre-tensioned until the level arm was balanced at the horizontal plane in the beginning of every load cycle. Strain values were recorded for 1000 time instants. Each experiment was repeated three times for each specimen to obtain the average values for all measurements and calculate the standard errors for the examined zones of interest. The maximum value of the sinusoidal strain over time was computed for each receiving position.
Statistical analysis
A statistical analysis was conducted, and the results are presented as the median of the maximum microstrain values derived from three measurements ± standard error. One-way analysis of variance (ANOVA) was used to evaluate changes in the stem length which lead to statistically significant results. The statistical findings were considered significant for p values <0.05.
Results
For zones 4, 9, 10, 12, and 13, the microstrain values were found to decrease with increasing the stem length (Figure 3). For all the other examined zones, the decrease in the stem length led to random alterations of the microstrain values and will not be further analyzed.
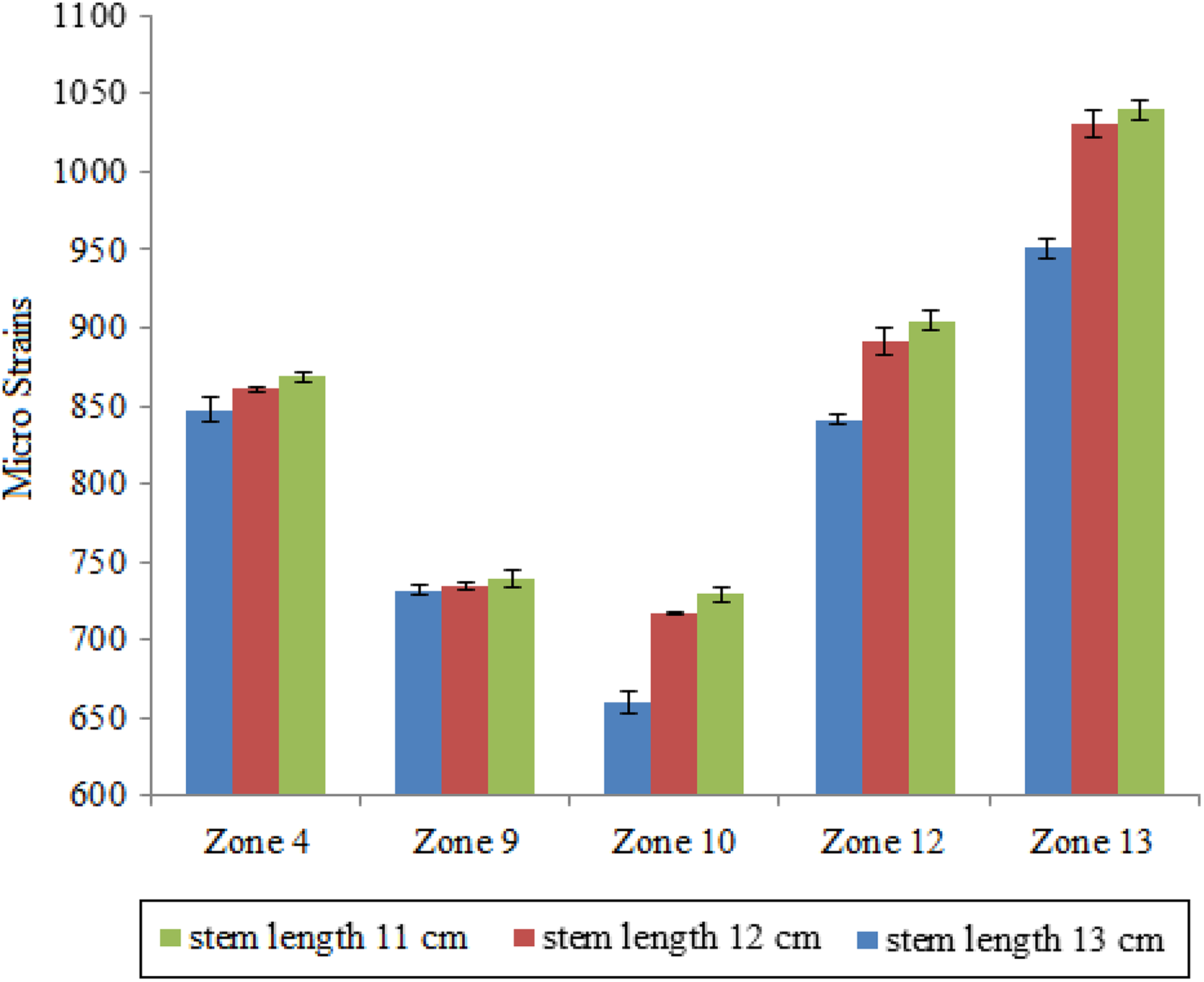
Microstrain values derived from the zones which revealed a specific microstrain pattern related to alterations in the stem length.
More specifically, for zone 4, the measured microstrains were 0.0848 for a stem length of 13.75 cm, 0.086 for 12 cm, and 0.0869 for 11 cm. For zone 9, the measured values were 0.0731 for 13.75 cm, 0.0734 for 12 cm, and 0.0739 for 11 cm. Higher differences were observed among the examined cases in zone 10 with microstrain values of 0.0656 for 13.75 cm, 0.072 for 12 cm, and 0.0729 for 11 cm. A same tendency was derived in zone 12, and the measured microstrains were 0.084 for 13.75 cm, 0.089 for 12 cm, and 0.090 for 11 cm. Finally, in zone 13, the measured values increased with decreasing the stem length from 0.095 for 13.75 cm to 0.103 for 12 cm and 0.104 for 11 cm.
In addition, it can be observed that the most significant differences among the examined stem lengths were derived for the zones 10, 12, and 13. More specifically, if we consider the stem length 13.75 cm as the reference case, the relative percentage difference (RPD) can be calculated as an indicator reflecting the absolute difference among various stem lengths in pairs. Concerning zone 10, the RPD was found 10.6% for the pair stem length 11–13.75 cm and 9.09% for the pair stem length 12–13.75 cm. For zone 12, the RPD was 7.14% for the pair stem length 11–13.75 cm and 5.95% for the pair stem length 12–13.75 cm. For zone 13, the RPD was found to be 9.47% for the pair stem length 11–13.75 cm and 8.42% for the pair stem length 12–13.75 cm. Lower RPDs were observed for zones 4 and 9. For zone 4, the RPD was found to be 2.35% for the pair stem length 11–13.75 cm and 8.60% for the pair stem length 12–13.75 cm. Finally, for zone 9, the RPD value was 1.37% for both the examined stem pairs.
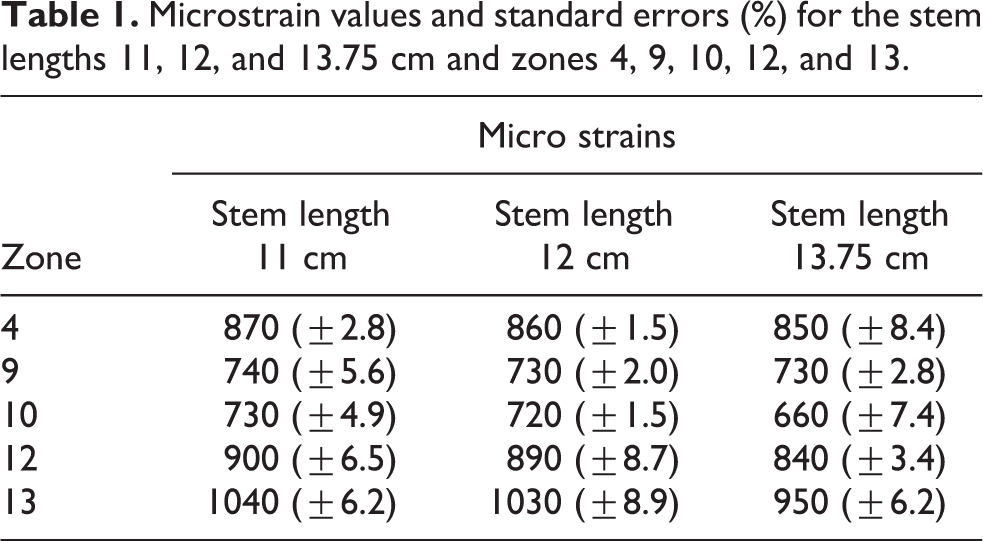
A statistical analysis was also performed based on the three repetitive measurements for each examined case, and the standard error bars are illustrated in Figure 3. One-way ANOVA was used to evaluate which stem lengths and zones lead to statistically significant differences. It was found that the p values for all the examined cases were lower than 0.05, approximating zero values, showing that the results are statistically significant, and there is association among the examined groups. Table 1 summarizes the microstrain values with the corresponding standard errors.
Microstrain values and standard errors (%) for the stem lengths 11, 12, and 13.75 cm and zones 4, 9, 10, 12, and 13.
Discussion
This work presented a biomechanical analysis aiming to investigate the role of the prosthesis length on the mechanical environment of the hip joint after a THA. From a clinical point of view, the main objective is to provide new knowledge on the impact of the stem length on aseptic loosening. The experiments were performed using custom-made, commercially available, medium left, fourth-generation, medium composite femoral models, and the single-leg stance of gait of a subject weighing 70 kg was considered as the loading condition. The experimental setup was based on the study of Politis et al. 2 Strain gages were used to measure the microstrains at 14 different receiving positions of the femur, and each measurement was conducted three times for the stem lengths 13.75, 12, and 11 cm.
It was found that in zones 4, 9, 10, 12, and 13 a decrease in the stem length leads to the increase of the microstrain values. Measurements from the great and lesser trochanter, as well as from the medial and lateral positions led to a random variation of the microstrain values and have not been further analyzed in the present work as no information can be derived for the evaluation of the stem length impact on the mechanical environment of the hip.
A statistical analysis was conducted and the calculated values of the standard errors indicate the accuracy of the three successive measurements which were performed for each zone and stem length. Also, the calculated p values indicate that the findings are statistically significant. Finally, when we considered the stem length of 13.75 cm as the reference case, higher RPDs were detected in zone 10 among the examined stem lengths in a pairwise comparison.
According to the literature, although a change in the stress pattern at the femur is expected after a THA, it is not known how the alteration of the stem length influences bone loading and which measurement positions could (a) reflect a risk for stress shielding and (b) early detect the factors that lead to revision THA including aseptic loosening. Stress shielding occurs when there is a mismatch in the elastic modulus of two materials perfectly bonded to each other, such as the prosthesis stem and the bone. 19 Aseptic loosening can be the result of inadequate initial fixation, mechanical loss of fixation over time, or biologic loss of fixation caused by particle-induced osteolysis around the implant. 20 Also, it should be emphasized that the stem size affects the survival rate of the implant. The clinical study of Retpen and Jensen 11 showed that the survival rate of a cemented revision femoral stem was improved if the stem extended beyond the zone of bone loss a distance equal to the diameter of the femoral shaft. This was validated experimentally by Panjabi et al. 12 However, Gramkow et al. 13 did not find a better survival rate for the stems which were longer than 210 mm compared to those that were shorter than 210 mm.
The results of this study are in agreement with the study of Dassler et al. 9 which evaluated the effect of femoral stem length on cements strains in a canine total hip replacement model. This study reported that although a shorter implant stem has a potential to improve implant fit, it led to significantly higher cement strains that may increase the risk for aseptic loosening. In addition, Bergin et al. 10 examined whether the diaphysis-to-stem ratio may predict loosening, and whether resection percentage correlates with failure, to establish the overall failure and aseptic loosening rates in a tumor population. Radiographs were used and the stem size, bone diaphyseal width, and resection percentage of the femur were determined. It was found that patients with stable implants had larger stem sizes and lower bone to stem ratios than those with loose implants. The results of the present study are in contrary to the study of Abdullah et al. 19 who examined the impact of stem length using the finite element method. The examined stem lengths were 13, 10, and 8.5 cm, and the stress variation was examined in intact and THA femur for normal walking activity. It was found that short prosthesis stem minimized the risk of stress shielding and bone thickening implying that the short prosthesis stem will increase the primary stability of the surgery. This can be explained by the fact that a shorter implant length limits the contact area of the prosthesis and bone with a material mismatch reducing the risk of stress shielding. Therefore, although according to Kim and Yoo, 8 the use of shorter implants has several advantages as they are less invasive due to less loss of osseous tissue, patients experience less pain, and there is less stress shielding, there are potential disadvantages such as malalignment, inadvertent subsidence, and potential proximal femoral fracture. 21 In addition, Shin et al. 21 showed that specific femoral short stems resulted in a higher incidence of malalignment and subsidence and a lower incidence of thigh pain and proximal bone resorption compared with conventional-length femoral stems.
However, no specific microstrain evolution pattern was detected in the great and lesser trochanter for different stem lengths. This could be attributed to the fact that the alterations of the stem length mainly influence the mechanical environment of the femoral shaft rather than the great trochanter which is more prone to structural changes of the prosthesis neck. According to Politis et al., 2 the use of long necks resulted in higher stress at the shaft of the femur, whereas the use of short necks led to higher stresses at the trans-trochanteric area. The increase of micro strains in Gruen zones distally to the pertrochanteric area could increase the risk of distal periprosthetic fracture, while it is unknown whether it could possibly influence the longevity of the prosthesis.
While the proposed study has presented useful information and new knowledge about the impact of the stem length on the mechanical environment of the hip after a THA, it has some limitations which have to be pointed out. First of all, only three different stem lengths were examined. Also, the effect of different loading conditions in combination with different stem lengths was not addressed. Furthermore, this study has the advantage of measuring the strain in ideal conditions, changing only the stem length every time. Nevertheless, this is often not the case in the clinical setting as the choice of the femoral stem geometry is made regarding the preoperative planning, the restoration of the leg length, joint stability, and the quality of the bone. 2 Finally, another constraint is that X-ray images were not considered for the evaluation of the implant position and strain evolution for different stem lengths, which could reveal supplementary information. However, the methodology presented in this work has been standardized in our previous study, 2 in which X-ray images were considered.
In conclusion, this is the first biomechanical study which investigates the microstrains at different receiving positions of composite femoral bones by changing the endoprosthesis length. Our future study will combine experimental and numerical means to further investigate which is the optimal stem length related to aseptic loosening and which is the role of the different loading conditions for normal and overweight subjects.
Conclusion
This work presented a biomechanical study aiming to investigate the effect of the implant stem length on aseptic loosening. The microstrains were measured at predefined receiving positions of the femur keeping constant the loading conditions and all the other material and structural properties of the femoral model and stem, except for the stem length. It was shown that the measured microstrain values in Gruen zones distally to the pertrochanteric area increase with decreasing the stem length which may increase the risk of distal periprosthetic fracture and influence the longevity of the prosthesis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.