
Abstract
Background
Perioperative antibiotics is a well established measure to prevent periprosthetic joint infection (PJI). However, the usual practice of prescription vary from surgeon to surgeon. This study aims to investigate and compare the usual practice and variability of prescribing antibiotic prophylaxis among different joint replacement surgeons in Hong Kong.
Methods
An online questionnaire was prepared and sent to members of the Adult Joint Reconstruction (AJR) Chapter of the Hong Kong Orthopaedic Association (HKOA). The questionnaire consists of a total of 15 questions in 3 categories: choice of antibiotics, dose of antibiotics and duration of antibiotics prescribed by the surgeon.
Results
A total of 25 responses were received and data collected. Participants were from a diverse background from different hospitals with variable years of experience. Results showed a general consensus on the choice of antibiotics, but also a wide variability on the actual prescription, particularly about the weight-adjusted dose and total duration of antibiotics given.
Conclusion
There is a wide variability among surgeons regarding the actual prescription of antibiotic prophylaxis. Correlation between rate of PJI and specific aspects of antibiotic prescription is needed to give recommendations to surgeons regarding perioperative antibiotic usage in total joint arthroplasties.
Introduction
In the current aging population, the incidence of osteoarthritis and total joint arthroplasties is increasing each year. One rare but devastating complication after arthroplasty is periprosthetic joint infection (PJI), which may expose the patient to repeated operations subsequently and impose a high financial cost to the healthcare system. Joint replacement surgeons have been undertaking various measures to prevent PJI.
One of the most well established measures is to prescribe peri-operative intravenous antibiotic as a prophylaxis to PJI. This has led to the creation of numeral guidelines published by different institutions around the world. However, many of these guidelines did not include specifics of the prescription, such as the choice of antibiotics, how the surgeon should proceed when patient has documented allergy, whether the dose given should be weight-adjusted, whether a combination of antibiotics is beneficial, and whether giving additional doses after the operation can reduce the risk of PJI. Without specific recommendations from guidelines, the usual practice might vary widely from surgeon to surgeon. The purpose of this study is to investigate and compare the usual practice and variability of prescribing antibiotic prophylaxis among different joint replacement surgeons in Hong Kong.
Materials and methods
Following institutional review board approval, we conducted an online questionnaire for practising orthopaedic surgeons in Hong Kong regarding their usual practice of prescribing antibiotic prophylaxis for total joint arthroplasties. The questionnaire was sent to members of the Adult Joint Reconstruction (AJR) Chapter of the Hong Kong Orthopaedic Association (HKOA). All members had full autonomy to choose whether to participate in the study or not, and they were given 3 months of time to reply before data collection was concluded. Demographic information of the surgeons, including gender, age, location of practice, and years of experience, were collected anonymously, with surgeon’s name list as an optional field.
The HKOA is a prominent body that comprises of orthopaedic surgeons in Hong Kong. Although the opinion of AJR Chapter members may not be generalized to every single joint replacement surgeon in Hong Kong, this sample gives us an idea whether the practice of antibiotic use is unanimous or widely disputed. Researchers will be able to know if the surgeons are following international guidelines, practice from local institutions or derived from their own personal opinions. This will give us insight whether any difference in practice will affect patient’s outcome, and whether the practice should be unified.
The main questionnaire consists of 15 questions divided in 3 categories: choice of antibiotics, dose of antibiotics and duration of antibiotics prescribed by the surgeon. Questions comprise the usual choice of antibiotics, the usual dose of antibiotics, their approach when patients have documented antibiotic allergy, their dose adjustments for overweight patients, and regarding additional doses given after the operation.
Results
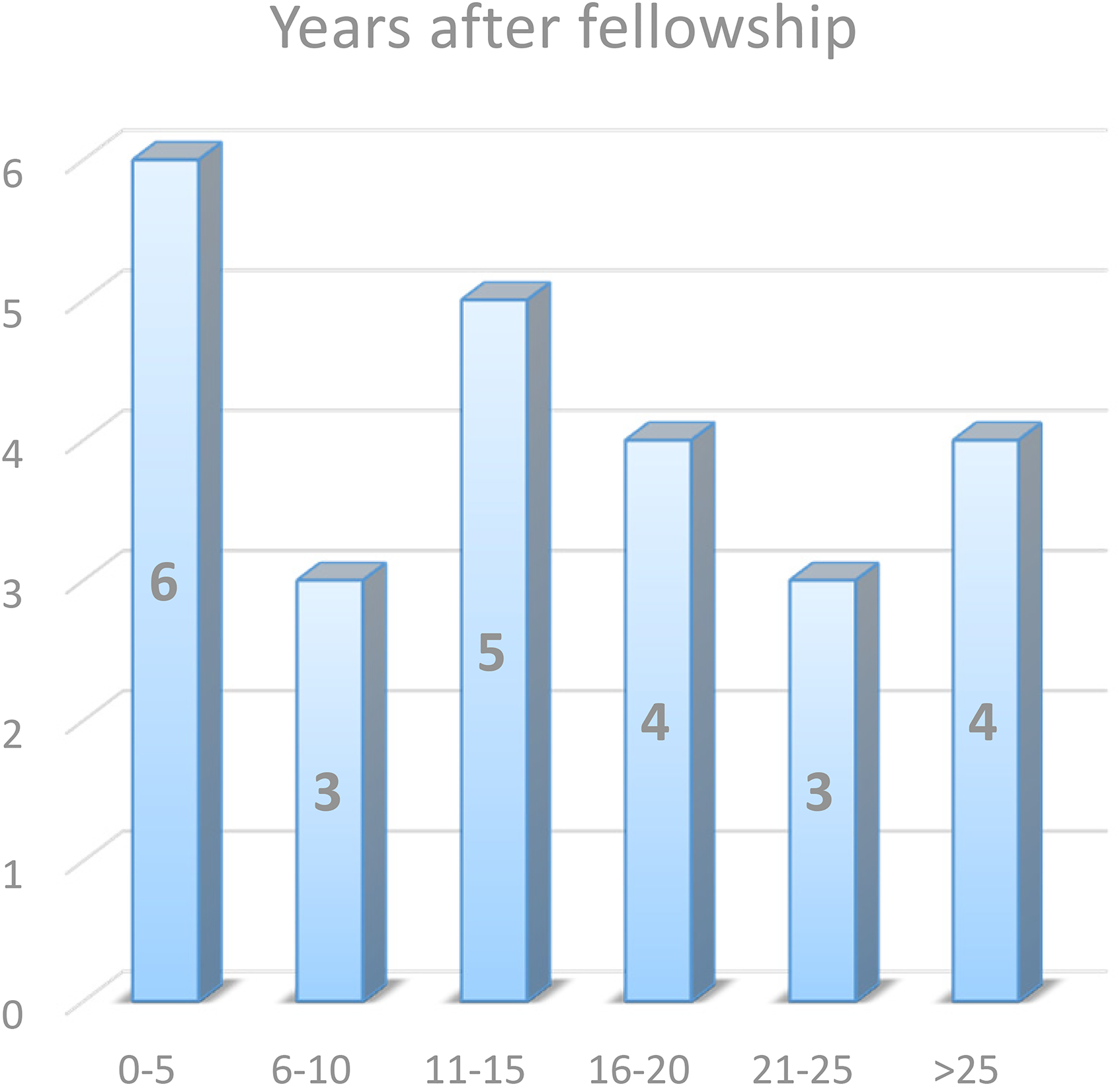
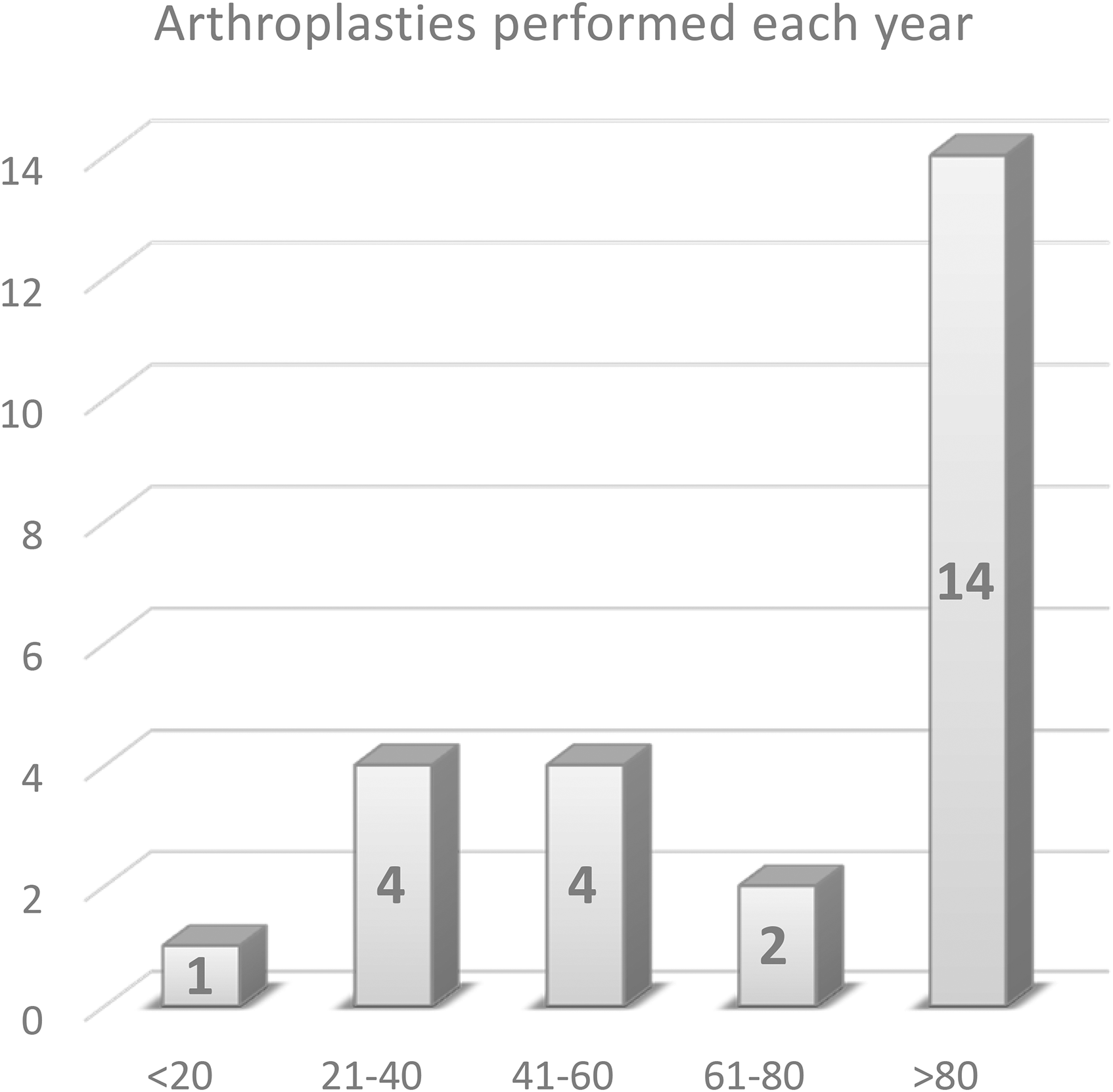
A total of 25 responses were received, amongst 79 members from the AJR Chapter. The overall response rate was 32%. The 25 participants have a diverse background from different hospitals in Hong Kong, with 15 (60%) in public practice, 8 (32%) in private practice, and 2 (8%) in both. They have variable years of experience in orthopaedic practice and joint replacement surgeries. Detailed statistics can be found in the figures below.
Section 1 – Antibiotic choice
This section covers the surgeon’s preferred choice of antibiotics, their approach when they face patients with beta-lactam allergy, and their opinion on prescribing a combination of antibiotics.
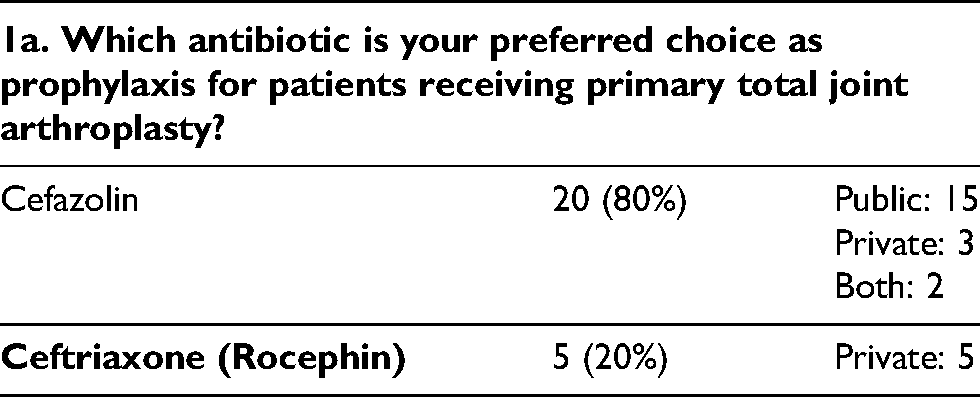
For primary total joint arthroplasty, 20 (80%) use intravenous Cefazolin while 5 (20%) use intravenous Ceftriaxone (Rocephin) as their preferred choice. The majority who use Cefazolin are in public practice while all 5 surgeons who use Ceftriaxone are in private practice.
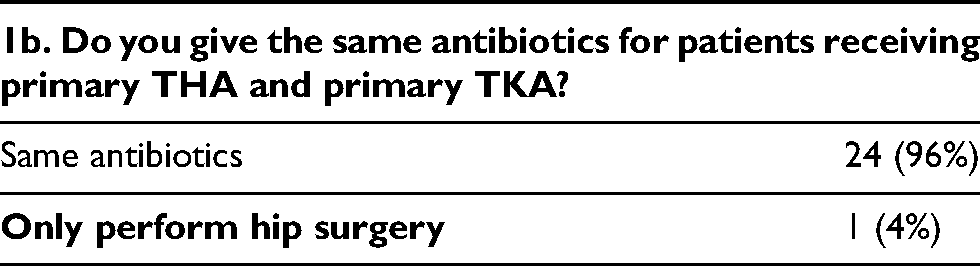
Nearly all (24/25) surgeons use the same choice of antibiotics for total hip arthroplasty and total knee arthroplasty, while 1 surgeon only performs total hip arthroplasty.
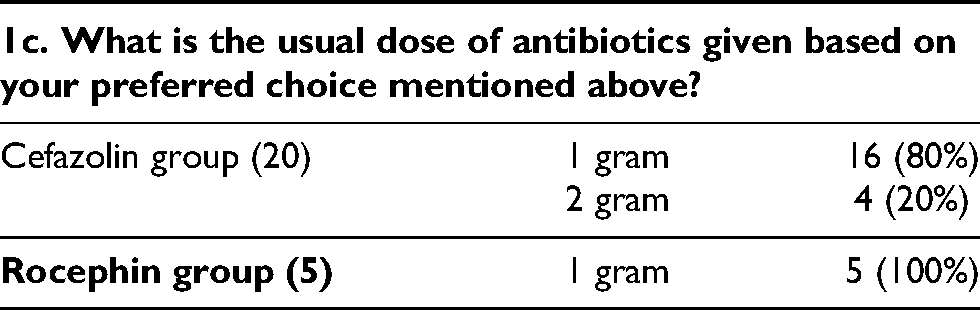
Regarding the preoperative dose of antibiotics given, 16/20 (80%) in the Cefazolin group give 1 gram of Cefazolin, while 4/20 (20%) routinely give 2 grams. All 5 surgeons who use Ceftriaxone prescribe 1 gram only.
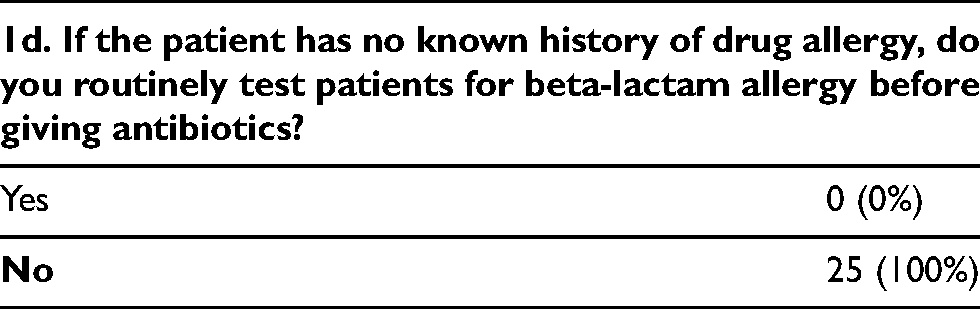
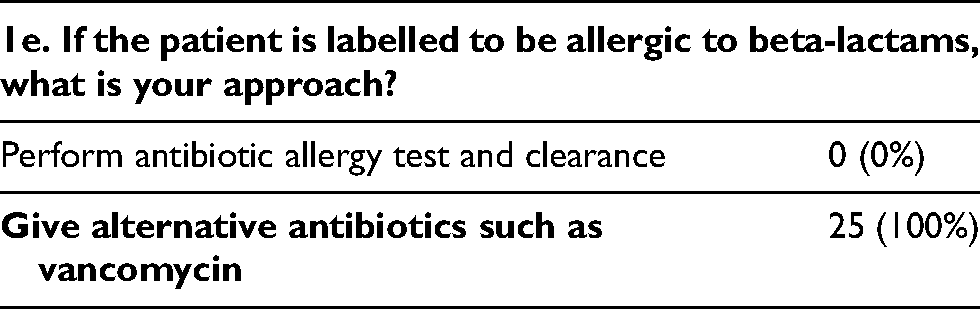
If the surgeon encounters a patient with no known history of drug allergy, none (0/25) of the surgeons will routinely test patients for beta-lactam allergy before prescribing beta-lactam group of antibiotics. If they encounter patients who are labelled to be allergic to beta-lactams, all surgeons (25/25) choose to give alternative groups of antibiotics such as vancomycin, rather than performing antibiotic allergy testing and clearance for the patient.
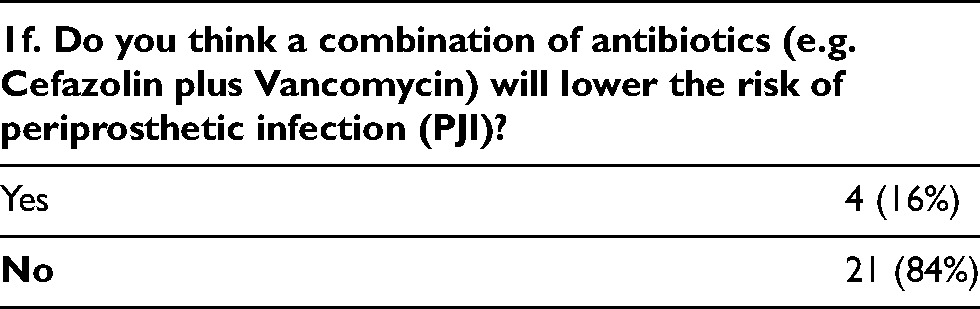
4 (16%) surgeons believe that a combination of antibiotics will lower the risk of PJI, while 21 (84%) think this method prescription has no impact on the risk of PJI.
Section 2 – Antibiotic dose
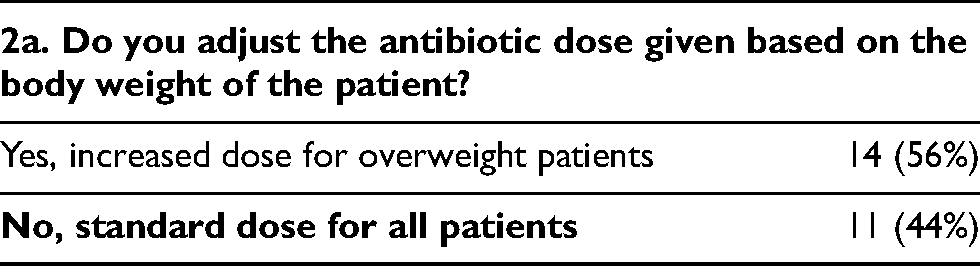
This section covers the surgeon’s approach to overweight patients – whether they will increase the dose for overweight patients and their criteria for increasing the dose.
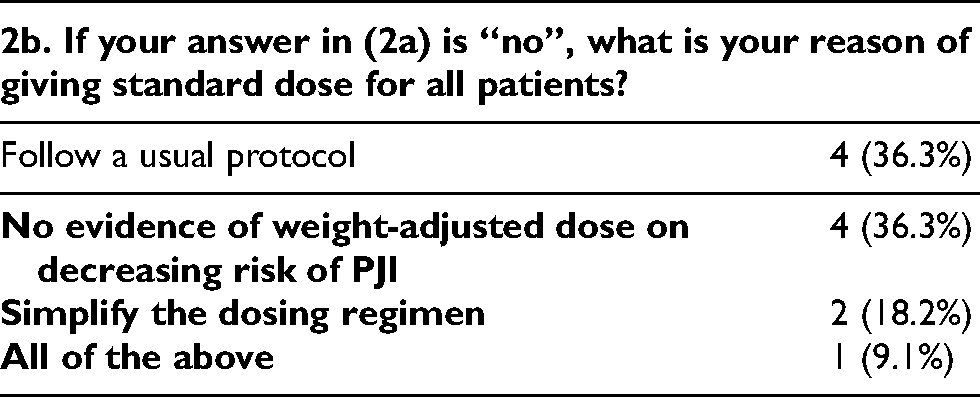
If the surgeon encounters overweight patients, 14 (56%) will prescribed increased dose of antibiotics, while 11 (44%) will keep a standard dose for all patients. The reason of giving standard dose for all patients is pretty diverse, including keeping a simplified regimen, following a usual protocol, and some believe increasing the dose in overweight patients will not affect the risk of PJI.
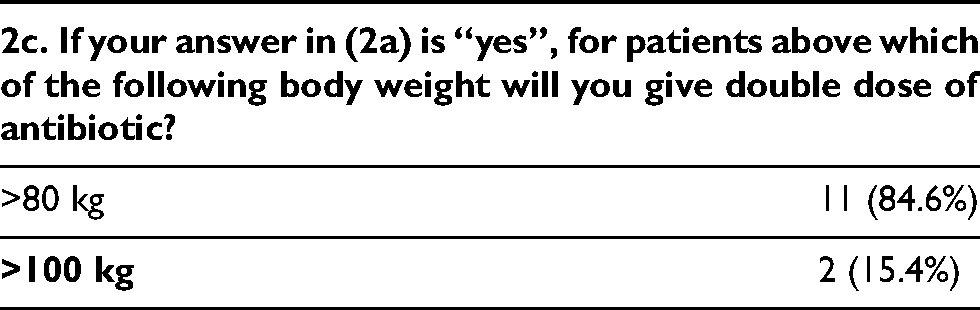
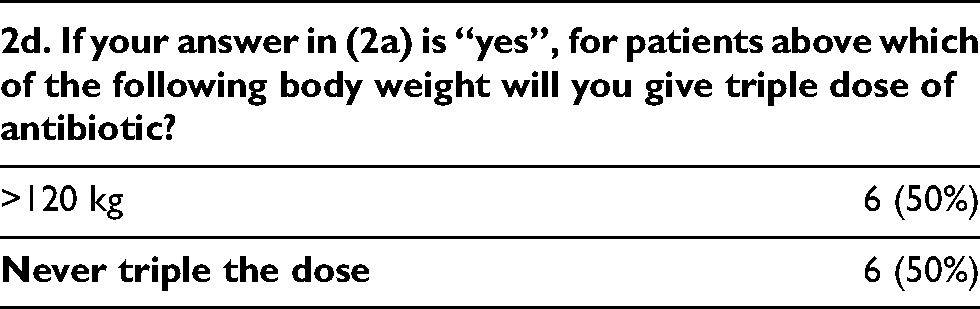
For those surgeons (n = 14) who will increase the dose for overweight patients, the majority use a cutoff value of body weight >80 kg as a criteria to give double dose of antibiotics. Half of the surgeons give triple dose of antibiotics when patient’s body weight is over 120 kg, while the other half will never triple the dose.
Section 3 – Antibiotic duration
This section covers the surgeon’s usual timing to give the preoperative dose of antibiotics, and the total duration of postoperative antibiotics given after skin closure.
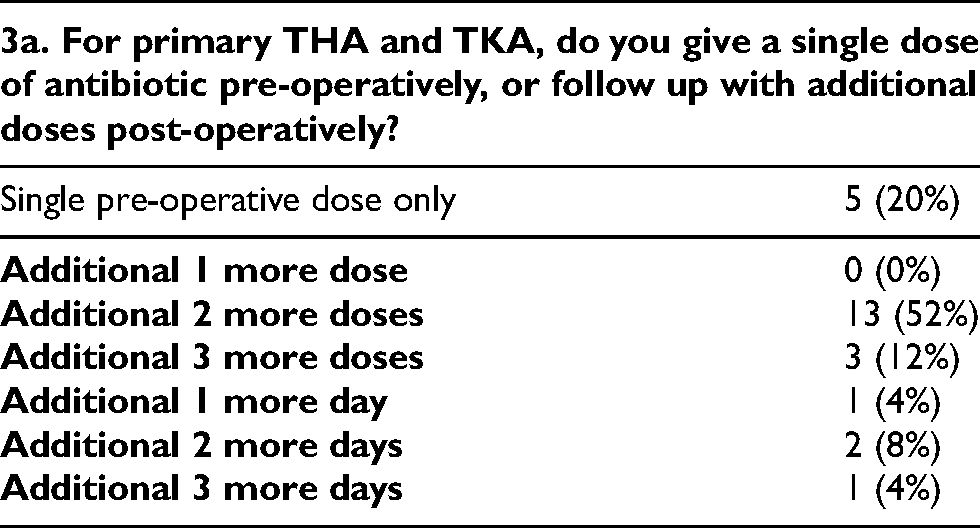
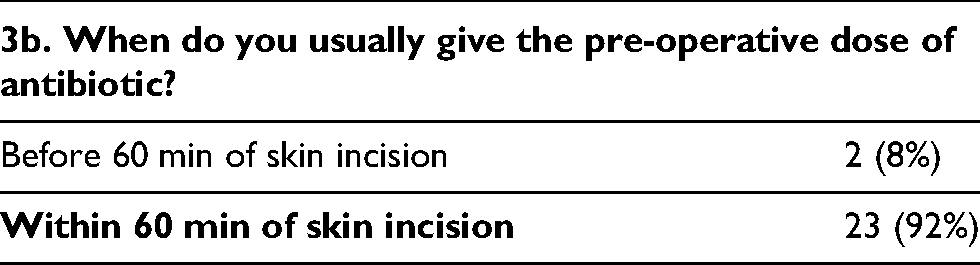
For primary total joint arthroplasty, only 5 (20%) surgeons give a single preoperative dose of antibiotics, while 20 (80%) will routinely give additional doses postoperatively. 2 (8%) surgeons usually give the preoperative dose of antibiotics before 60 min from skin incision, while 23 (92%) give the preoperative dose within 60 min of skin incision.
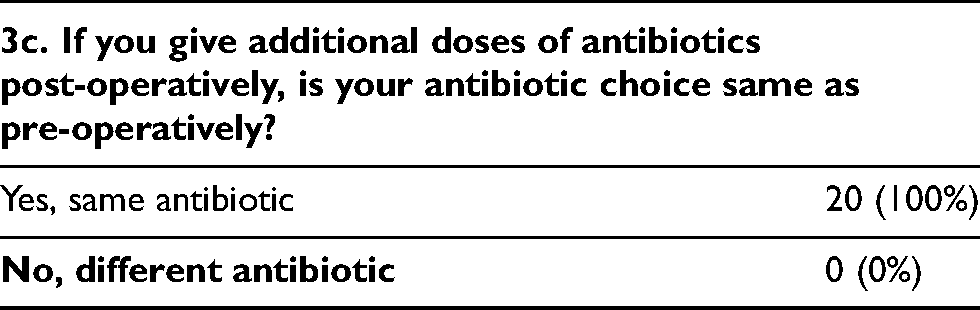
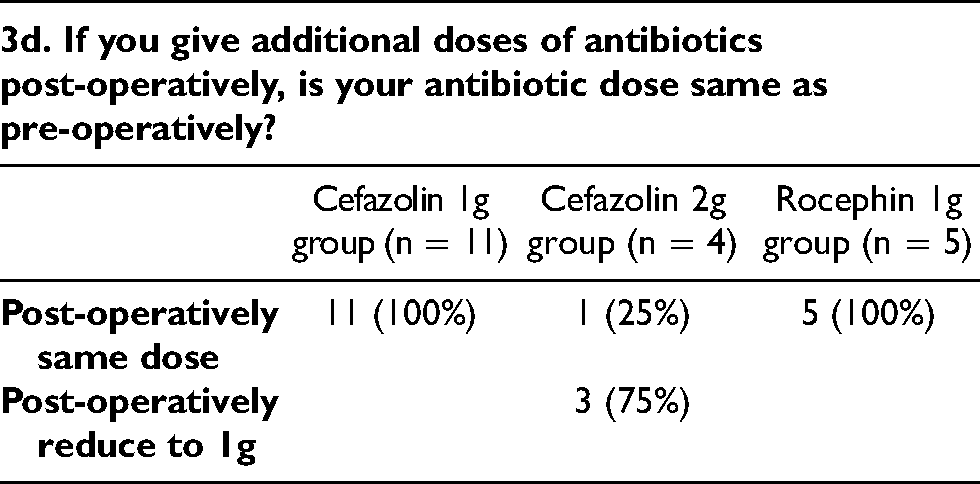
The choice and dose of preoperative and postoperative antibiotics are compared. All surgeons use the same choice of antibiotics preoperatively and postoperatively. For those who give 1 gram Cefazolin or 1 gram Rocephin as their preferred choice of antibiotics, their postoperative dose remains the same. However, for those who give 2 grams of Cefazolin (n = 4), 1 (25%) will keep the same dose (2 grams) postoperatively while 3 (75%) choose to reduce the postoperative dose to 1 gram only.
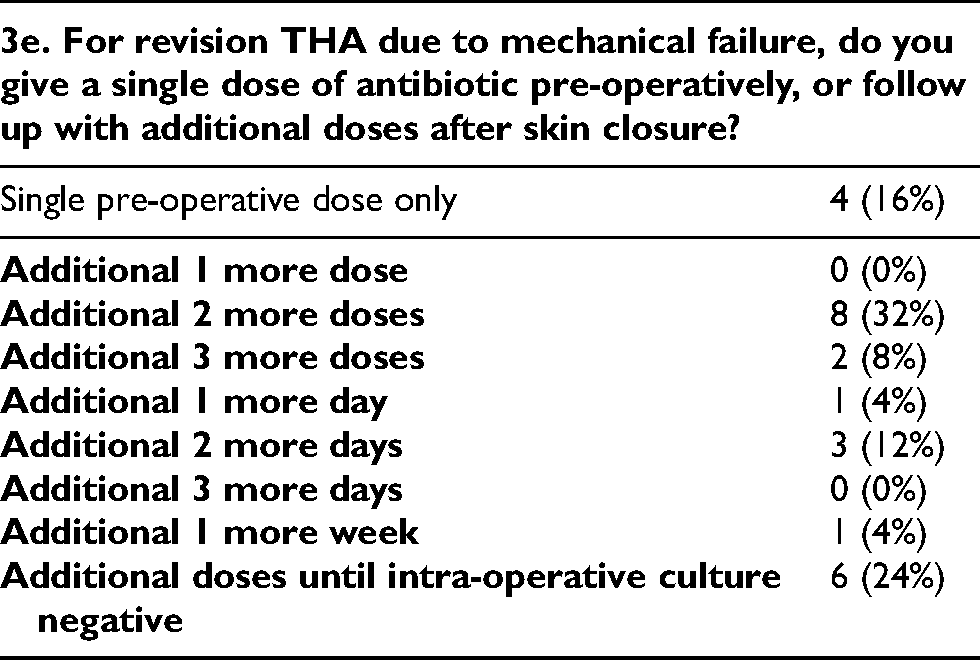
For revision total hip arthroplasty due to mechanical failure, 6 (24%) surgeons will continue to give postoperative antibiotics until intraoperative culture results are negative, instead of giving a standard number of doses or a standard duration.
Discussion
Periprosthetic joint infection (PJI) is a devastating complication following total joint arthroplasty. Administration of prophylactic antibiotics is well proven to lower the risk of PJI. Certain recommendations were created by different organizations across the world, such as WHO, 1 NICE guidelines 2 from UK and AAOS 3 from USA, based on existing evidence. However, individual surgeons still have full autonomy on prescription of antibiotics for their patients.
This is the first study conducted in Hong Kong analysing the usual practice of prescribing antibiotic prophylaxis among joint replacement surgeons. In some aspects, such as the choice of antibiotics, the majority of surgeons favours the same options, following universal recommendations. For example, all surgeons choose to use cephalosporin group of antibiotics (either Cefazolin or Ceftriaxone) as their preferred choice. However, when it comes to the details of the prescription, such as weight-adjusted dose and post-operative antibiotic regime, the results vary greatly and there is no consensus found between different surgeons. The surgeon’s individual choice may be related to the practice of their previous mentors or based on protocols at their own institutions.
For instance, in one of the earlier local studies in 2003, Tang et al. 4 reviewed the deep wound infection rate of 1367 primary total hip and total knee arthroplasties performed in the 1990s. Comparison was made between 2 groups of patients – those who received a single dose of Cefazolin and those who received 3 doses of Cefuroxime. There was no statistically significant difference in deep wound infection rate between the two groups. Single dose Cefazolin is proven effective and has since been widely used at the institution due to dosing convenience.
Among the many antibiotics available in Hong Kong, all surgeons choose to use either Cefazolin or Ceftriaxone (Rocephin) as their preferred choice of antibiotic prophylaxis. Looking into the pharmacokinetics of these two antibiotics, in the review by Thabit et al., 5 both Cefazolin and Ceftriaxone achieve excellent penetration into bone and soft tissues, with their average concentration in bone and synovial fluid exceeding the minimum inhibitory concentration against most pathogens. It is also believed that the easy availability of Cefazolin and Ceftriaxone in most hospitals in Hong Kong may have contributed to their popularity in their use by surgeons.
The result of Section 1 shows that surgeons in the public sector generally favours Cefazolin while surgeons in the private sector favours Rocephin. Patients who undergo total joint arthroplasties in public hospitals are often recruited into “pathways” that recommend prescription of Cefazolin unless otherwise contraindicated. Local guidelines such as IMPACT 6 also recommend the use of Cefazolin of Cefuroxime in total joint replacement surgeries with prosthesis. The favoured use of Rocephin in the private sector could be attributed to its lower cost (as private patients are paying for every drug cost), or due to the personal preference of individual surgeons.
Theories aside, does the choice of antibiotic actually affect the rate of periprosthetic joint infection? Wyles et al. 7 recently reviewed 29695 primary total hip arthroplasties and total knee arthroplasties in 22705 patients, and divided them into those receiving Cefazolin and non-Cefazolin group of antibiotics. Infection-free survivorship was significantly higher among arthroplasties receiving Cefazolin compared with Non-cefazolin antibiotics. Overall, the risk of PJI was 32% lower in patients treated with Cefazolin. The authors also recommended perioperative testing and clearance for all patients presenting with penicillin and cephalosporin allergies, which interestingly, none of our surgeons included it as their routine practice. Not all hospitals in Hong Kong offer the service of allergy testing. Moreover, referring for allergy testing and clearance may further postpone the arthroplasty surgery. This could be the reason most surgeons choose to give an alternative class of antibiotics instead.
Another interesting situation is when surgeons encounter overweight patients. The overall opinion is pretty diverse, from whether the dose of antibiotics should be adjusted for overweight patients, to cutoff value for doubling or tripling the dose. Rondon et al. 8 retrospectively reviewed 17393 primary total joint arthroplasties receiving Cefazolin as prophylaxis. They found out that underdosing is common, especially for patients weighing over 120 kg. Moreover, underdosed patients were more likely to develop periprosthetic joint infection. Orthopedic surgeons should pay attention to the weight-based dosing of antibiotics in the perioperative period to avoid increasing risk of PJI.
Regarding the total duration of antibiotics given, the result ranges from a single pre-operative dose up to a few doses or a few days after the operation. This debate not only occurs between surgeons, but between health organizations as well. In 2017, the Center for Disease Control and Prevention (CDC) published their Guideline for the Prevention of Surgical Site Infection. 9 Regarding post-operative antibiotics in total joint arthroplasty, they stated, “In clean and clean-contaminated procedures, do not administer additional prophylactic antimicrobial agent doses after the surgical incision is closed in the operating room, even in the presence of a drain (Category IA–strong recommendation; high-quality evidence)”. This was met with a strong positional statement published by the American Association of Hip and Knee Surgeons (AAHKS) 10 in November 2017, stating the CDC recommendation was based on heterogenous evidence, and the citations used appear to be underpowered to discern the true safety of withholding the post-operative antibiotics. The consensus was to limit antibiotic use beyond 24 hours, to balance the risk between PJI and emergence of resistant organisms. Further Level I study is required to elucidate the effect of single prophylactic antibiotic dosing versus 24-hr antibiotic dosing.
Conclusion
Most joint replacement surgeons in Hong Kong use either Cefazolin or Rocephin as their choice of antibiotic prophylaxis in total joint arthroplasty. However, there is still a wide variability among surgeons regarding the actual prescription. Future studies may aim at correlation between rate of PJI and specific aspects of antibiotic prescription, such as underdosing and post-operative antibiotic use. If there is a significant difference in PJI rate from different prescriptions, recommendations should be given to surgeons to guide perioperative antibiotic usage in total joint arthroplasties.
Footnotes
Conflicts of interest statement
The authors declare that there is no conflict of interest.
Funding
No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical review statement
This study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (HKU/HA HKW IRB).
IRB reference number: UW 20-484.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.