
Abstract
Purpose:
Maintaining independence after hip fracture repair is important for geriatric patients and general welfare. We investigated the effects of anesthetic methods on postoperative activities of daily living (ADLs) following hip fracture surgery in elderly patients.
Methods:
The medical records of 12,342 patients aged ≥65 years who underwent typical surgeries for hip fracture using either general anesthesia or spinal anesthesia were reviewed. To adjust for baseline differences and minimize selection bias for the chosen method of anesthesia, patients were matched by propensity scores. Factors affecting the deterioration in ADLs during hospital stay were also investigated in all subjects using a multivariate logistic regression analysis. Eating, grooming, toileting, bathing, and walking were selected as the ADL parameters, as they are considered important for an independent life.
Results:
Of the 12,342 patients, 6918 (56.1%) received general anesthesia and 5424 (43.9%) received spinal anesthesia. After the propensity score matching, the anesthesia types were not associated with ADL scores except toileting at discharge. Results from the multivariate logistic regression analysis showed that the types of anesthesia were not associated with deterioration in ADL scores. Advanced age, male sex, high Charlson Comorbidity Index scores, psychiatric disease, no administration of nonsteroidal anti-inflammatory drugs, and short length of hospital stay were associated with deterioration in ADL scores.
Conclusion:
The anesthesia types were not associated with ADL dependency except toileting at discharge. Spinal anesthesia adversely affected toilet use at hospital discharge. However, anesthesia types were not factors that affected deterioration in ADL during hospital stay in elderly patients who underwent hip fracture surgery.
Introduction
Hip fractures are a global public health concern. Approximately 1.6 million hip fractures are reported to occur annually worldwide, and the incidence is expected to drastically increase several times over the next three decades due to the aging population. 1,2 Most hip fractures are treated with surgical repair, which requires general or regional anesthesia. 3 Several investigations have attempted to determine the type of anesthesia that is optimal for hip fracture, but the evidence remains conflicting. 3 –9 General anesthesia enables patients to be completely free from mental stress during the surgeries. Covert and Fox reported that general anesthesia significantly reduced hypotensive episodes and blood loss when compared to regional anesthesia. 10 Hypotension and/or blood loss may preclude adequate oxygen delivery to the central nervous system during surgery. Anemia is reported to be a factor related to a poor outcome after hip fracture surgery. 11,12 On the contrary, spinal anesthesia can keep the patient at a consistent level of consciousness through the perioperative and operative periods. A systematic review reported that general anesthesia, compared to regional anesthesia, might increase the risk of developing postoperative cognitive dysfunction. 13 It is widely known that cognitive impairment is a risk factor for poor functional outcomes in geriatric trauma patients. 14 –16
Thus far, the main comparisons between general anesthesia and regional anesthesia methods have been mortality and morbidity, as it is difficult to investigate the changes in intellectual faculties, or in the ability to live independently, using large-scale retrospective studies. However, these factors are speculated to be associated with recovery, and poor outcomes require increased utilization of social financial assistance. 17 Since 2002, data have been accumulated for 10 parameters of activities of daily living (ADLs) in many Japanese hospitals using the diagnosis procedure combination (DPC) system. We speculated that the parameters for ADLs within the nationwide administrative claims database are indicators of postoperative physical and mental status, both of which have serious effects on both quality of life and the social welfare budget.
The purpose of this study was to investigate the effects of anesthetic technique (general or spinal) on five ADL parameters (independent eating, grooming, toileting, bathing, and walking), at discharge, and on the changes in the ADL parameters during the hospital stay in elderly patients who had undergone surgery for hip fracture.
Materials and methods
This retrospective cohort study was approved by the ethics review board of the Kasumigaura Medical Center and National Hospital Organization (NHO).
Following the Japanese ethics guidelines for human medical research, this study protocol was made available to the general public via the NHO website to obtain patient objections. To protect patient privacy, all types of personal identification were encrypted in a security room of the NHO data bank. The requirement for individual informed consent was waived due to the anonymous nature of the data.
Data sources
The study period was from April 1, 2012, to March 31, 2016. We used data from the Japanese DPC administrative claims database that was obtained from 69 hospitals of the NHO group. The DPC database is a diagnosis-dominant, case-mix system administered by the Ministry of Health, Labor, and Welfare of Japan and linked with a lump-sum payment system. We obtained hospital characteristics data from the 2016 resident recruitment guidebook of the NHO and the website of the Japanese Society of Anesthesiologists.
Selection of patients and variables
The inclusion criteria were that all patients had to be aged 65 years or older and should have undergone surgery for hip fracture (transcervical, intertrochanteric, and subtrochanteric femoral fracture) during the study period. The surgery type included total or hemiarthroplasty and other typical hip fracture procedures (plate/screw or intramedullary implant). Only patients undergoing either general anesthesia or spinal anesthesia were selected. Patients receiving unknown, mixed spinal and general, or other anesthesia types were excluded. Furthermore, we excluded 90 cases of atypical surgeries (repair of previous implanted plate, etc.) and 2347 cases for missing baseline characteristics data. This left 12,342 patients of an initial 14,779 for the analysis.
Data from the DPC database included age, sex, height, weight, fracture type, surgical procedure, comorbidities at admission, complications after admission, medications during admission, and functional status, which was based on the patient’s ability to perform tasks related to ADL both at admission and at discharge. Body mass index (BMI) was calculated from height and weight. Functional status included the following 10 parameters: self-feeding, transfer, grooming, toilet use, bathing, mobility, use of stairs, dressing, defecation, and micturition. 18 We chose 5 parameters (eating, grooming, toileting, bathing, and walking) from the 10 ADL abilities as indicators of independence. ADL scores for eating and toileting were defined as totally dependent (score 0), partially dependent (score 1), and independent (score 2). ADL scores for grooming and bathing were defined as dependent (score 0) and independent (score 1). ADL scores for walking were defined as totally dependent (score 0), partially dependent (wheelchair using; score 1), partially dependent (walking; score 2), and independent (score 3). The change in ADL was determined by deducting the baseline ADL score (at admission) from the ADL score at hospital discharge. A negative number (−3, −2, or −1) indicated deterioration, zero indicated no change, and a positive number (3, 2, or 1) was indicative of improvement.
A modified Charlson Comorbidity Index (CCI) was calculated for each patient based on the Quan coding algorithms. 19 Hospitals authorized by the Japanese Society of Anesthesiologists have full-time, certified staff as well as residents in training. Data regarding the use of anesthetics and postoperative medication for analgesics and sedation were evaluated. Of the analgesics, 20 kinds of nonsteroidal anti-inflammatory drugs (NSAIDs) were included: aspirin, celecoxib, diclofenac, dimetotiazine mesilate, emorfazone, etodolac, flurbiprofen, ibuprofen, indomethacin, isopropylantipyrine, ketoprofen, lornoxicam, loxoprofen, mefenamic acid, meloxicam, naproxen, salicylate, sulindac, tiaramide, and zaltoprofen. Haloperidol was used as an antipsychotic drug. The postoperative hospital length of stay (LOS) was defined as the number of calendar days from operation to discharge.
Propensity score matching
The propensity score-matched analysis was used for reducing the selection bias and potential baseline differences between the general and the spinal anesthetic groups. Scores were calculated using a binary logistic regression analysis with type of anesthesia as the dependent variable and 23 preoperative factors as predictor variables. The independent variables were age, sex, BMI, the modified CCI, length of hospital stay after surgery, fracture type, surgery type, hospital type (scale and level of anesthesiology), five ADL parameters (eating, grooming, toileting, bathing, and walking) at hospital admission, and baseline comorbidities (malignancy, anemia, endocrine/metabolism, mental, neurologic, circulatory, respiratory, digestive, and renal/urinary). The score was defined as probability of a patient receiving general anesthesia based on covariates. After adjustment with the scores, none of the preoperative variables remained statistically different between the two groups. The multivariate regression model of propensity for a patient given general anesthesia had a C-statistic of 0.67. (C-statistic is a standard measure of the predictive accuracy of a logistic regression model.)
Statistical analysis
Patient and operating characteristics were compared between the general and the spinal anesthesia groups using the t-test or the paired t-test for continuous variables and the χ 2 test for categorical variables. The ADL scores at hospital discharge were assessed using the Pearson χ 2 test after the propensity score matching. Multivariate logistic regression analysis was performed between the deterioration and the nondeterioration (no change and improvement) groups to analyze the effects of various factors. In addition to anesthesia methods, the following were selected for the model: age, sex, modified CCI, psychiatric disease (F00), NSAIDs, antipsychotic drugs, and LOS. These variables have been previously suggested to affect the prognosis. 20 –29 Odds ratios and 95% confidence intervals were determined. A p value of <0.05 was considered significant for all statistical tests. All statistical analyses were carried out using SPSS software version 24 (IBM, Armonk, New York).
Results
Of the 12,342 patients who underwent hip surgery during the 4-year observation period, 6918 (56.1%) received general anesthesia and 5424 (43.9%) received spinal anesthesia. Table 1 compares the characteristics of the two groups. Before propensity score matching, 18 of the 23 baseline factors differed significantly between the two anesthesia groups. After 1:1 matching, there was a total of 3949 patients in each anesthetic group, with no significant baseline differences.
Demographic and clinical characteristics of patients who underwent hip fracture surgery.

BMI: body mass index.
Table 2 summarizes the ADL score for independence at hospital discharge in the matched sample. Anesthesia types were not associated with ADL scores for eating, grooming, bathing, and walking. Patients in the spinal anesthesia group had a significantly higher percentage of total dependence for toileting than did patients in the general anesthesia group (spinal vs. general: 40.3% vs. 36.7%; p < 0.003). A total of 174 patients died and were excluded from the analysis: 109 (1.6%) in the general anesthesia group and 65 (1.2%) in the spinal anesthesia group. This difference in mortality rates was not significant (p = 0.078).
ADL at hospital discharge.

ADL: activity of daily living.
Results from the multivariate regression models showed that the type of anesthesia was not associated with deterioration in the ADL scores for eating, grooming, toileting, bathing, and walking after hip surgery. Nonadministration of NSAIDs was associated with deterioration in all ADL scores. In addition, advanced age, male sex, high CCI scores, psychiatric disease, and short length of hospital stay were associated with deterioration in four ADL (eating, grooming, toileting, and walking) scores (Table 3).
Multivariate analysis: Factors affecting ADL deterioration during hospital stay.
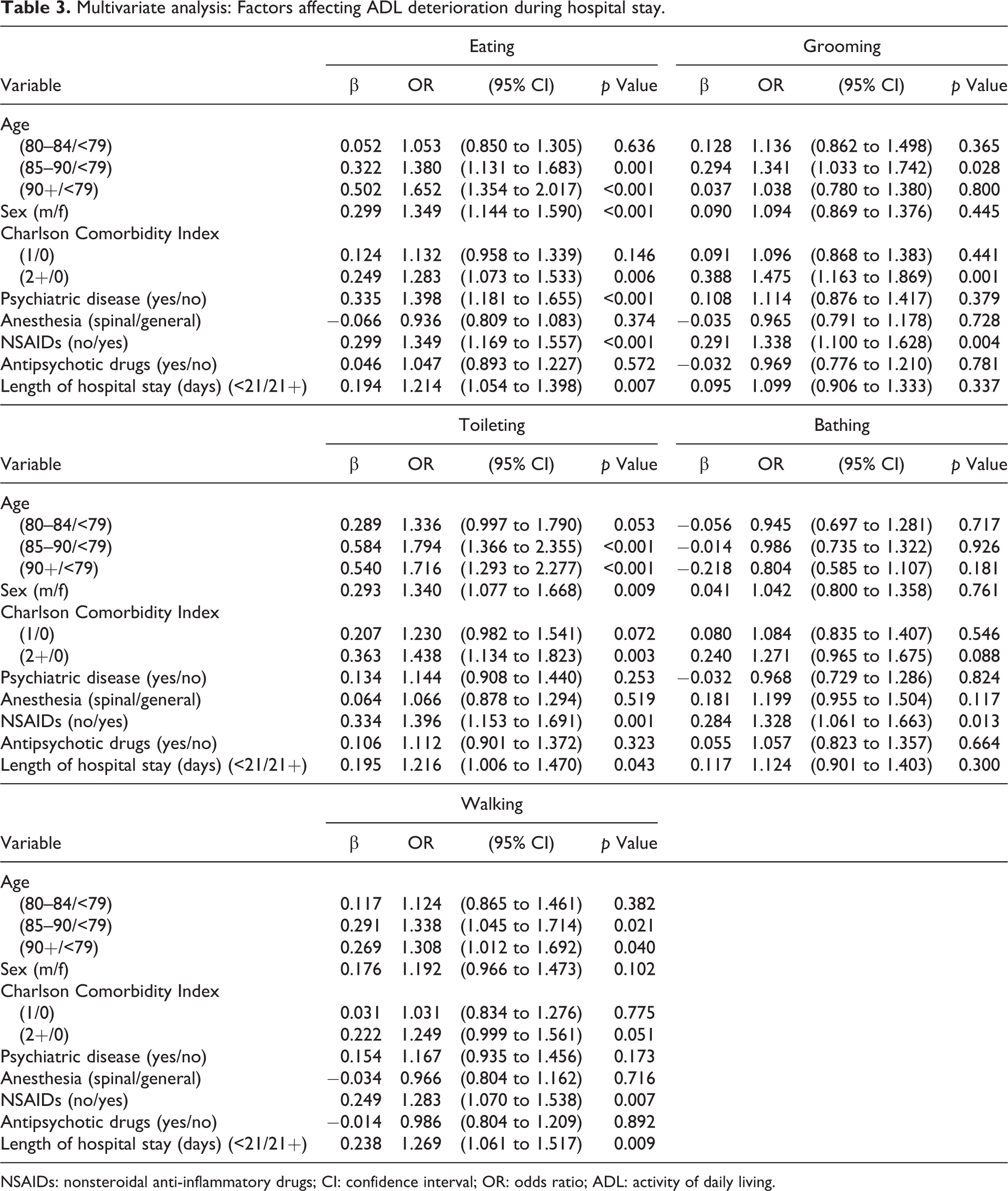
NSAIDs: nonsteroidal anti-inflammatory drugs; CI: confidence interval; OR: odds ratio; ADL: activity of daily living.
Discussion
Using the DPC database of the NHO group and a propensity-matched analysis, we studied the impact of anesthesia type on ADL (eating, grooming, toileting, bathing, and walking) scores for independence at hospital discharge and changes in the ADL scores during the hospital stay following surgery for hip fracture. After the propensity score matching, anesthesia types were not associated with ADL functions except toileting. Results from the multivariate logistic regression analysis showed that anesthesia types were not factors affecting ADL deterioration during hospital stay.
There are many studies evaluating levels of ADL after hip fracture. 30 –35 However, to our knowledge, only one group investigated the effect of anesthetic technique on ADL variables in their small-scale study. 36 They reported that no differences were observed in ADL (feeding, dressing, bathing, toileting, walking, etc.) scores between general and regional anesthesia groups at 3, 6, and 12 months after hip fracture. Although we used data for ADL scores at the time of hospital discharge, almost all of our results were in accordance with that of the long-term outcome study.
In the present study, patients in the spinal anesthesia group had a significantly higher percentage of total dependence for toileting than did patients in the general anesthesia group. Spinal anesthesia is reported to cause a clinically significant disturbance in bladder function. 37,38 Intrathecal local anesthetics cause an interruption in the micturition reflex by blocking both afferent nerves and efferent fibers. Since the micturition reflex is a very delicate system, spinal anesthesia might confuse the reflex and slow the recovery of bladder function in this study.
Alarcon et al. reported that the probabilities of recovering the previous functional performance level in grooming and eating at the time of hospital discharge were 41.6% and 47.98%, respectively. 32 Since they excluded nonambulatory patients with serious conditions from their study, the previous functional level is speculated to be independent. In our study, the probabilities of independence in grooming and eating were about 32% and 46%, respectively. Although the probabilities determined from our data are slightly lower than those of Alarcon et al.’s study, we think the results are compatible with their data as we did not exclude patients with serious conditions.
Deterioration in a patient’s ability to eat independently was not associated with the type of anesthesia in our multivariate logistic regression analysis. Sandman et al. stated that elderly people who were totally dependent on assisted feeding were more disabled with regard to other ADL functions. 39 Feeding problems might be a terminal phenomenon in the hierarchical loss of ADL functions. Furthermore, Siebens et al. reported that loss of independence in eating was associated with an increased risk of mortality within 6 months. 40 Thus, self-feeding may have to be considered as the most important item in the Barthel’s ADL Index. We speculate that the type of anesthesia might have no impact on the overall deterioration in ADL, because it is not related to deterioration in eating independently.
A common factor for deterioration in independent eating, grooming, and toileting was a higher CCI score. An increase of more than two points in the CCI increases the rates of deterioration by 28% for eating, 48% for grooming, and 44% for toileting. This result is in accord with the finding of previous studies. 31,35 Advanced age, male sex, and psychiatric disease were associated with deterioration in some ADL scores. Penrod et al. reported that advanced age and psychiatric disease (dementia and stroke) had a negative impact on ADL functions after hip fracture. 34 Advanced age is commonly recognized to be a determinant factor for loss of independence, 30,31,35 whereas opinions are divided on the gender effect on independence as measured by ADL functions. 20,41
The probability of regaining prior levels of autonomy 6 months after surgery is reported to be only 33.6% even in previously independent elderly patients. 42 Bertram et al. reported in their review that 29% of elderly patients did not reach their prefracture levels 1 year postfracture and went on to experience lifelong disability. 43 It is not easy for elderly patients to regain prefracture functional levels. Patients lose their confidence and independence due to long-term disability after a hip fracture. Thus, medical factors related to postoperative deterioration in ADL functions are important. In the present study, no administration of NSAIDs was associated with deterioration in all ADL scores. Hip pain was reported to be a risk factor related to functional dependence. 28,35 The present study reconfirms that postoperative analgesia is important. Kawano et al. reported that ketoprofen prevented the development of surgery-associated memory deficits via its pain-relieving effects. 44 Delirium is also a risk factor for failure to regain prefracture levels of function. 45 In human and animal studies, postoperative cognitive dysfunction has been reported to be associated with a neuroinflammatory response triggered by surgery. 46 –48 NSAIDs might reduce the risk of poor functional recovery via their anti-inflammatory mechanisms.
Our study had some limitations. Our data did not include several important data such as physical status as categorized by the American Society of Anesthesiologists, details of intraoperative hemodynamics, bleeding volume, and oxygen saturation. Our ADL data were collected only from hospitals. The ADL scores at hospital administration might be underestimated, because they are easily influenced by environment and/or social lifestyle. Additionally, not all our results may be generalizable to other races and countries because this study population was mainly Japanese.
Conclusion
In the propensity score matching analysis, anesthesia types were not associated with ADL (eating, grooming, bathing, and walking) scores at discharge. Results from the multivariate logistic regression analysis showed that the type of anesthesia was not associated with deterioration in the ADL scores. Spinal anesthesia adversely affected the toilet use at hospital discharge. However, it was not a deterioration factor for toileting. Advanced age, male sex, high CCI scores, psychiatric disease, no administration of NSAIDs, and short length of hospital stay were associated with deterioration in ADL scores. In addition to the patient’s factors (CCI, age, sex, and coexisting disease), further investigation of additional medical factors should be considered in order for elderly patients to maintain independence after hip fracture surgery.
Footnotes
Acknowledgment
The authors thank Chiharu Okada, MD, PhD, MBA (National Hospital Organization Headquarters, Department of Hospital Management Assistance) for arranging this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.