
Abstract
Purpose:
This historical cohort study aims to determine the relationship between premorbid functional status and functional decline in hip fracture patients.
Methods:
Eighty-two hip fracture patients were divided into Group A (good rehabilitation potential) and Group B (fair rehabilitation potential) based on four premorbid functional assessments: Modified Functional Ambulation Category (MFAC), Modified Barthel Index (MBI), Hong Kong Montreal Cognitive Assessment 5-Minute and functional prognosis predictive score. Declines in MFAC and MBI after rehabilitation were compared.
Results:
Sixty-seven percent of patients in Group A had up to one category decline in final MFAC, whereas 66% in Group B had more than one category decline. Similarly, median decline in final MBI was seven in Group A versus 22 in Group B.
Conclusion:
Hip fracture patients with good rehabilitation potential have significantly fewer functional declines. It is possible for them to be directly discharged from acute hospital for outpatient rehabilitation.
Introduction
Owing to increasing life expectancy and prevalence of osteoporotic fracture, the demand for intensive rehabilitation after hip fracture becomes an ongoing challenge to public hospitals services. Inpatient rehabilitation of hip fracture is considered completed if there is no further improvement in mobility and basic activities of daily living after a reasonable period of hospitalisation. Those who cannot return to independent functional status will require fulltime carer or institutionalisation on discharge. However, if discharge planning depends solely on rehabilitation progress and could not be predicted in advance, hospitalisation will be prolonged, which is a health economic issue. In our locality, the cost per patient per day for general inpatient services in public hospitals exceeds 5000 Hong Kong dollars. 1
In our experience, rehabilitation potential after hip fracture is highly related to and limited by the premorbid functional status. For many years, various functional outcome measures have been widely used in monitoring the progress of rehabilitation in hip fracture. 2 In the literature, age, cognitive and motor scores at admission and premorbid comorbidities were reported to be significant predictors of discharge mobility and self-care scores among hip fracture patients. 3,4 To the best of our knowledge, there were only limited studies investigating the relationship between premorbid functional status and functional outcomes in Chinese patients with hip fracture.
In this historical cohort study, hip fracture patients were divided into two groups with different rehabilitation potentials based on four functional assessment tools. Final functional outcomes, declines in functional outcomes and discharge destination were compared. Our null hypothesis is that there is no statistically significant difference in the absolute functional declines between the two groups.
Methods
The hospital database was reviewed on hip fracture patients admitted to our hospital from August 1, 2016 to March 31, 2017. A total of 106 patients were identified. Our inclusion criteria were as follows: 1. Chinese patients aged 50 years or above; 2. with neck of femur, pertrochanteric and subtrochanteric fracture and 3. who received operative treatment with either fixation (including dynamic hip screws or proximal femoral nail in pertrochanteric/subtrochanteric fracture and screw fixation in undisplaced femoral neck fracture) or hemiarthroplasty (including cemented bipolar/unipolar hemiarthroplasty, Austin Moore arthroplasty and cemented Thompson prosthesis in displaced femoral neck fracture) performed.
Our exclusion criteria were as follows: patients who had 1. nonoperative treatment due to high anaesthetic risks (3 patients excluded); 2. perioperative stroke, intracranial haemorrhage or myocardial infarction which affect functional outcomes (3 patients excluded); 3. associated upper limb fracture that affects functional outcomes (3 patients excluded); 4. postoperative complications (such as prosthetic hip dislocation or wound infection) requiring second operations and prolonged hospitalisation (4 patients excluded); 5. revision operation for complications after initial operation (2 patients excluded) and 6. failed functional assessments due to noncommunicable status (9 patients excluded). After exclusion, 82 patients aged from 55 years to 100 years remained for further statistical analysis.
Premorbid functional assessments were performed, including ambulatory level using Modified Functional Ambulation Category (MFAC), and premorbid comorbidities using functional prognosis predictive score (FPPS) by physiotherapists, independence in basic activities of daily living (ADL) using the Modified Barthel Index (MBI) and cognitive status on admission using Hong Kong Montreal Cognitive Assessment 5-Minute (HK MoCA 5-Min) by occupational therapists.
Modified Functional Ambulation Category
MFAC is a mobility outcome measure commonly used to classify walking capacity. It was first described in 1984 and later expanded to include seven categories: I (lyer), II (sitter), III (dependent walker), IV (assisted walker), V (supervised walker), VI (indoor walker) and VII (outdoor walker). 5,6 It demonstrated good content validity, discriminative power and interrater reliability in Chinese patients with hip fracture and stroke. 6,7 Final MFAC of V (supervised walker) is chosen as the cutoff for satisfactory mobility outcome in our study as it is the minimum requirement for a patient to ambulate at home without a full-time carer.
Modified Barthel Index
The MBI is one of the most widely used assessments on a person’s ADL performance. It consists of 10 items: ambulation or wheelchair, chair–bed transfer, stair climbing, personal hygiene, bathing, dressing, feeding, toileting, bowel control and bladder control, with standardised rating criteria. 8–10 It was developed from the Barthel Index, which was first published in 1965 and further modified by Shah et al to the MBI to improve discriminative power for each item with increased sensitivity, higher content reliability and internal consistency. 9,11 The Chinese version that we used, which has culture-specific description of 10 items, showed satisfactory structural validity, interrater reliability and high interrater consistency. 10
Hong Kong Montreal Cognitive Assessment 5-Minute
Most studies supported that prefracture cognitive impairment of geriatric patients is negatively associated with their functional recovery after hip fracture. 12 –17 Montreal Cognitive Assessment (MoCA), which was developed in 2005, has become one of the most widely used screening tools for cognitive dysfunction internationally. 18 It had better sensitivity in detecting mild cognitive impairment and equivalent specificity when compared with another wellknown assessment tool, Mini-Metal State Examination. 19,20 A brief version of MoCA in our locality (HK MoCA 5-Min) was developed to shorten the administration time at bedside. 21 It assesses four cognitive domains: attention, verbal learning and memory, executive function or language and orientation. Similar to full version, HK MoCA 5-Min retained a 30-point scoring with cutoff scores at 16th, 7th and 2nd percentiles according to one’s education level and age to represent different levels of cognitive function (Table 1). 22
Ageand education-corrected normative data of total score of HK MoCA 5-Min.
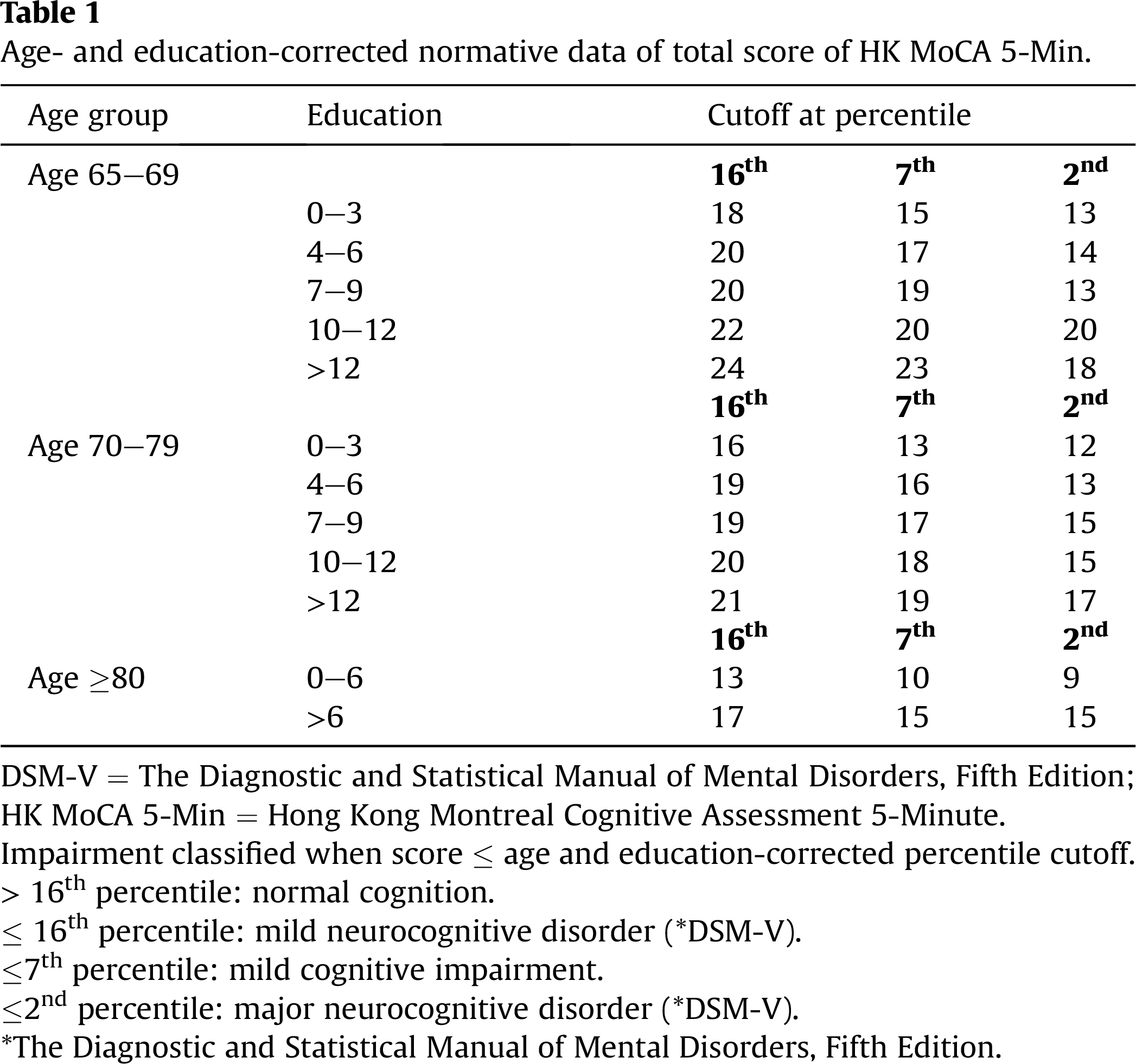
DSM-V = The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; HK MoCA 5-Min = Hong Kong Montreal Cognitive Assessment 5-Minute.
Impairment classified when score ≤ age and education-corrected percentile cutoff.
>16th percentile: normal cognition.
≤ 16th percentile: mild neurocognitive disorder (*DSM-V).
≤ 7th percentile: mild cognitive impairment.
≤ 2nd percentile: major neurocognitive disorder (*DSM-V).
*The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Functional Prognosis Predictive Score
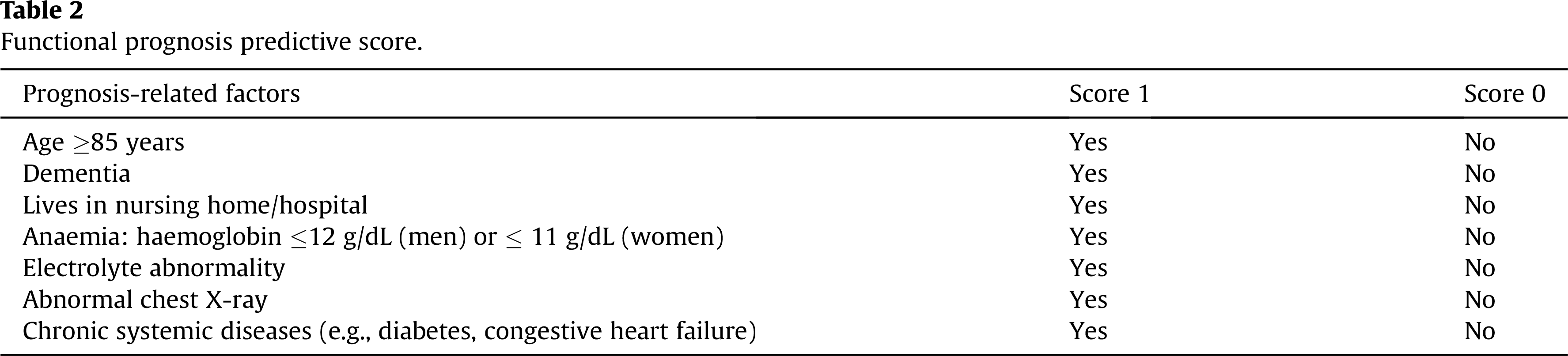
FPPS is a scoring tool developed in Japan by Hagino et al, which is used to predict ambulation prognosis in the elderly after hip fracture (Table 2). 23 It consists of seven prognosis-related factors, presence of each will score 1 and the maximum score is 7. The higher the score is, the more number of comorbidities the patient has, which also imply on the underlying frailty, polypharmacy and chance of developing perioperative medical complications in geriatric hip fracture patients. Hagino et al showed that the postoperative ambulatory group had a significantly lower FPPS than the nonambulatory group. Similar results were also obtained by our physiotherapy team, in which a significant negative correlation was found between FPPS and final MFAC (p value <0.001), making FPPS as a good prediction tool for better use of limited rehabilitation resources. 24,25 Patients with intermediate (3–4) or high (5–7) score will require more intensive rehabilitation than those with low score (0–2).
Functional prognosis predictive score.
After premorbid functional assessment (MFAC, MBI, HK MoCA 5-Min and FPPS) and operation, all patients received intensive mobility and ADL training according to the standardised rehabilitation protocol. Most of them (74 patients) were transferred to a convalescent hospital for further rehabilitation, whereas some of them (8 patients) were directly discharged from an acute hospital and referred to outpatient rehabilitation. The progress of rehabilitation was monitored weekly using MFAC and MBI. Rehabilitation was considered completed when there was no further improvement in MFAC and MBI. Final MFAC and MBI on discharge were documented, and declines in MFAC and MBI were calculated. Operation types (grouped into fixation or hemiarthroplasty), length of stay (in acute and convalescent hospitals) and discharge destination (return home or transfer to nursing home) were recorded. Most patients (49 patients) discharged from the convalescent hospital received further ambulatory rehabilitation in a geriatric day hospital, except those who refused the service, having dementia or with social reasons such as transport difficulty (25 patients). Fracture liaison service (including fall prevention program and antiosteoporotic treatment for selected patients) was provided in a geriatric day hospital and fragility fracture clinic.
Preliminary statistical analysis was performed using IBM® SPSS® Statistics 21 , to determine the correlation between the four premorbid functional assessment scores (MFAC, MBI, HK MoCA 5- Min and FPPS) and functional outcomes (final MFAC and MBI). All of them showed statistically significant correlation to each other, with the correlation coefficients ranging from 0.41 to 0.54 (p value < 0.001). On the other hand, correlations between the four scores were relatively weak (correlation coefficients 0.23–0.45, p value < 0.05), meaning that no single score could explain the overall premorbid functional status of a hip fracture patient. For example, some elderly patients with dementia (HK MoCA 5-Min ≤2nd percentile) and multiple comorbidities (e.g., FPPS 4) could able to walk unaided outdoor (e.g., MFAC 7 and MBI 91). As a result, we decided to use a combination of all four scores for the prediction of functional outcomes.
Patients were then divided into two groups based on the four premorbid functional assessment scores (Table 3). Those with MFAC from VI to VII, MBI from 91 to 100, HK MoCA 5-Min above 7th percentile and FPPS from 0 to 2 belonged to Group A. Otherwise, those with MFAC less than VI, MBI below 91, HK MoCA 5-Min equal to or less than 7th percentile or FPPS more than 2 belonged to Group B. In essence, we defined Group A as those with good premorbid functional status and presumably good rehabilitation potential, whereas Group B with a few premorbid comorbidities and presumably fair rehabilitation potential.
Patient groups.
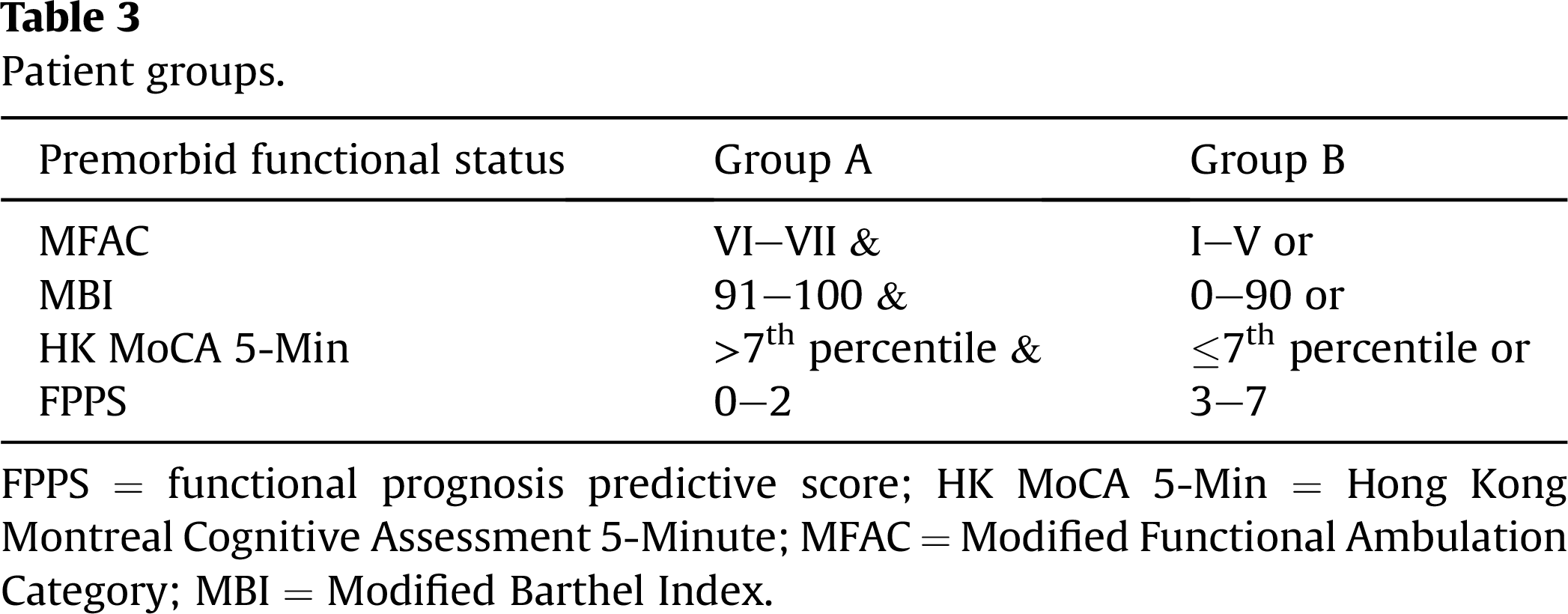
FPPS = functional prognosis predictive score; HK MoCA 5-Min = Hong Kong Montreal Cognitive Assessment 5-Minute; MFAC = Modified Functional Ambulation Category; MBI = Modified Barthel Index.
Data were analysed with corresponding statistical tests. For continuous variables (including age, length of stay, final MBI and decline in MBI), because they were tested nonnormally distributed, Mann–Whitney U test was used. For categorical variables (including gender, operative methods, final MFAC, decline in MFAC and discharge destination), Chi-square test was used. A p value ≤ 0.05 was considered statistically significant.
Results
There were 24 patients in Group A and 58 patients in Group B. There were no significant differences in gender, operation types and length of stay between the two groups. Patients in Group A were, however, significantly younger than those in Group B (Table 4).
Patient characteristics.
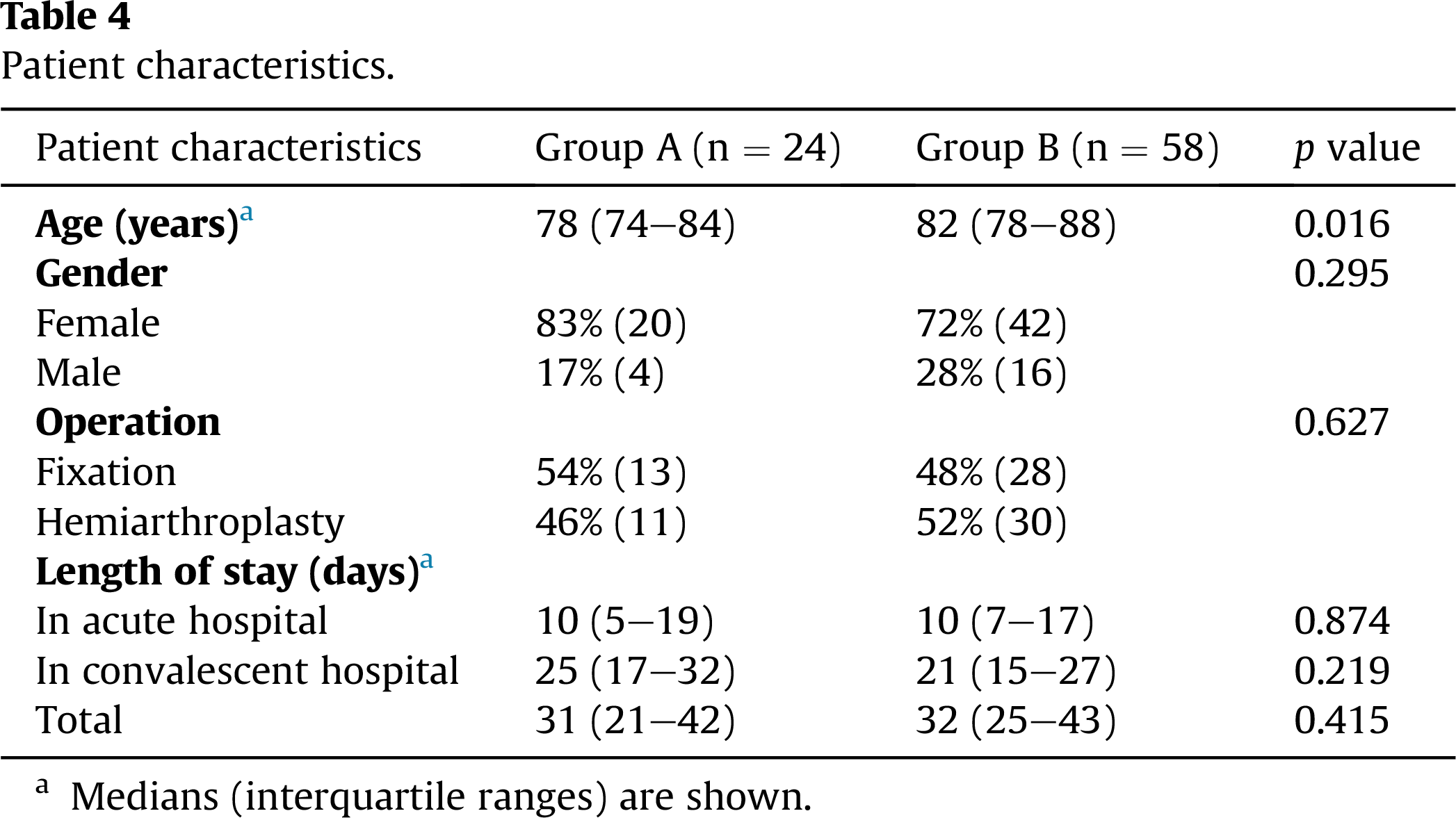
a Medians (interquartile ranges) are shown.
Functional outcomes are shown in Table 5. Group A achieved a significantly better ambulatory level in terms of final MFAC greater than or equal to V (supervised walker). Most patients in Group A had a decline in MFAC up to one category. For independence in basic ADL in terms of MBI, Group A achieved a median score of 91 which is classified as slight dependence and significantly better than Group B. The decline in MBI is also significantly less in Group A. All the patients in Group A returned home, in which six of them (25%) could be directly discharged from the acute hospital with the mean length of stay of 17 days. On the other hand, around one in four in Group B required nursing home on discharge, of which five of them were originally residents in nursing home before fracture.
Functional outcomes.
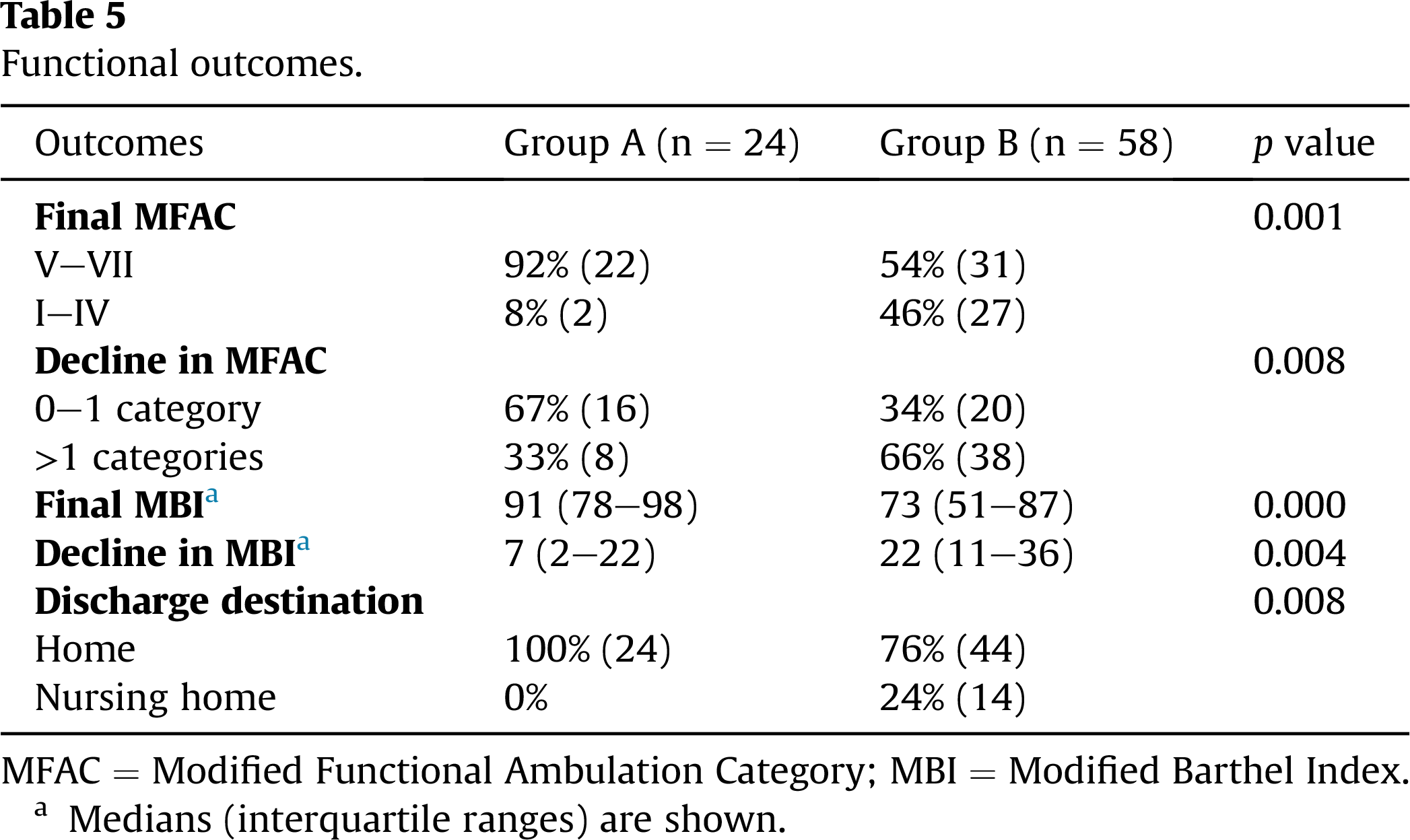
MFAC = Modified Functional Ambulation Category; MBI = Modified Barthel Index.
a Medians (interquartile ranges) are shown.
Discussion
In this study, we have two observations. First of all, hip fracture patients with good premorbid functional status were associated with better final MFAC and MBI. In other literature, advanced age and low prefracture functional level were also found to be strong predictive factors for poor functional outcomes. 26,27 Moreover, there were significantly fewer declines in final MFAC and MBI for those with good premorbid functional status. Our findings were different from those of the study by Beloosesky Y et al in which there was no significant difference in the decline of Functional Independence Measure scores between three groups of patients with different levels of prehospital functional dependency and cognitive impairment. 4
There are some implications for no significant difference in the length of stay between the two groups. In clinical point of view, inpatient rehabilitation deserves a reasonable period of hospitalisation for assessment, optimisation, training and review. For those with good rehabilitation potential and progress, the clinical team tended to provide further inpatient training until maximal functional improvement reached, whereas for those with limited rehabilitation potential and progress, early discharge was suggested. In study’s point of view, both the groups received same intervention (similar period of inpatient rehabilitation), but one group that has good premorbid functional status (Group A) performed significantly better than the other (Group B) and was able to return home.
In this historical cohort study, discharge planning was based on rehabilitation progress. The question becomes whether the length of stay could be shortened in future by advanced predication of functional outcomes and proactive discharge planning. Over a decade, clinical pathway for geriatric hip fracture has been implemented in public hospitals in our locality to reduce preoperative length of stay and improve clinical outcomes through multidisciplinary approach. 28,29 To our knowledge, patients in major centres will be directly transferred to convalescent beds for further rehabilitation, irrespective of rehabilitation potential. 28–30 Whether direct discharge from acute hospitals for outpatient rehabilitation is an alternative pathway for patients with good rehabilitation potential was not thoroughly discussed in their studies. Based on our findings, we propose a new clinical pathway to guide rehabilitation and discharge planning (Figure 1). Our selection criteria are different from those in the case-mix system proposed by Chin et al using Functional Independence Measures and Abbreviated Mental Test because both of them are not our preferred functional assessment tools. 30
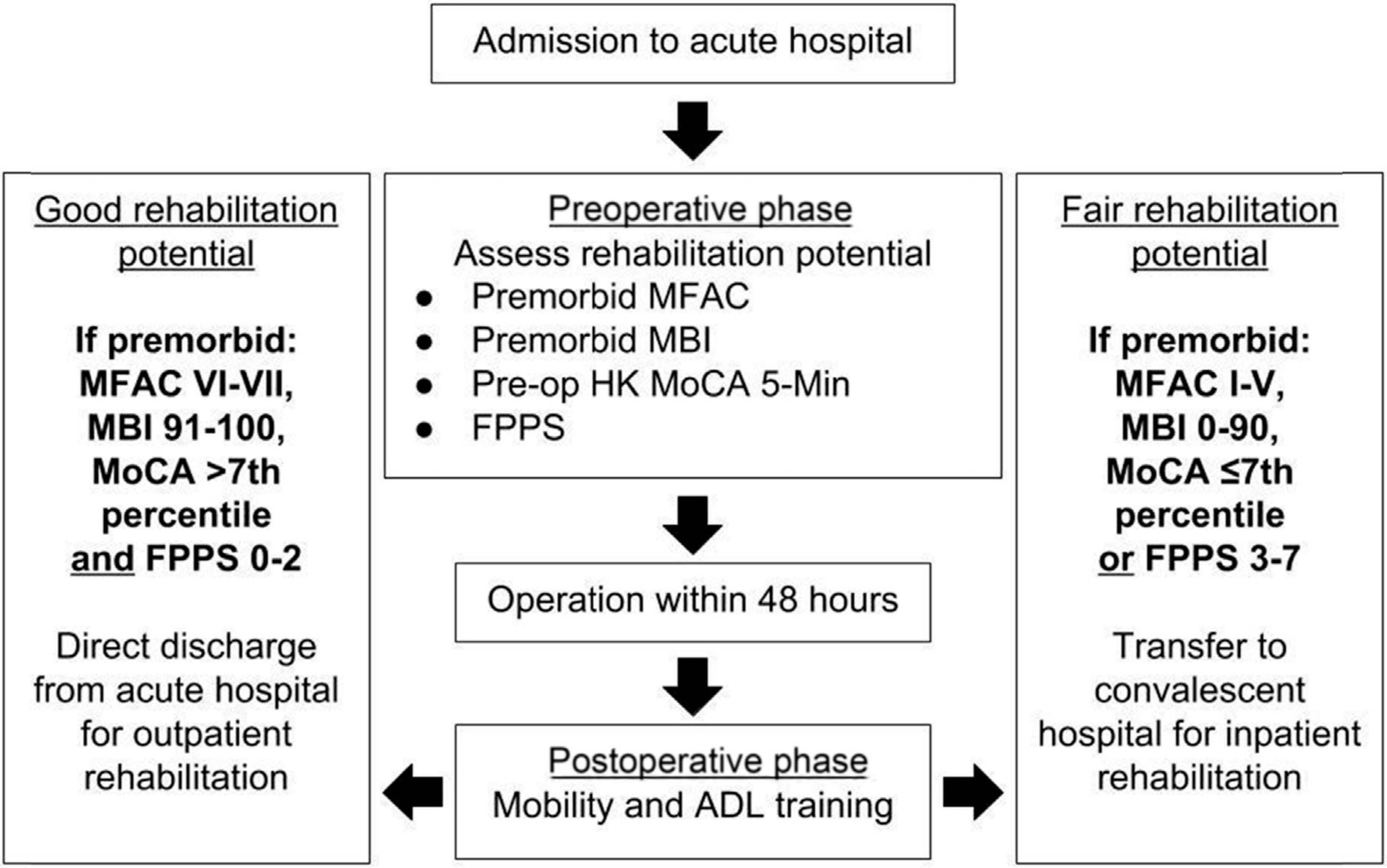
Clinical pathway for geriatric hip fracture rehabilitation. ADL = activities of daily living; FPPS = functional prognosis predictive score; MoCA = Hong Kong Montreal Cognitive Assessment 5-Minute; MFAC = Modified Functional Ambulation Category; MBI = Modified Barthel Index.
Our study showed that decline in MFAC is unequal in the two groups. Hypothetically, we propose a sigmoid curve model of final MFAC against premorbid MFAC, based on our clinical observation for years. For those with premorbid MFAC VI–VII (e.g., independent elderly), the slope (decline in MFAC) is low, meaning that they are likely to ambulate independently after hip fracture. For those with premorbid MFAC III–V (e.g., partially dependent elderly), the slope becomes steep, meaning that final MFAC may decline significantly after hip fracture as their physical reserve is marginal and can be greatly compromised by frailty, deconditioning and medical complications. This group of patients will be most benefited by intensive rehabilitation and geriatrician’s care in convalescent hospitals. For those with premorbid MFAC I–II (e.g., totally dependent elderly), the slope flattens again because no further decline or improvement is allowed. Similarly, a sigmoid curve model of final MBI against premorbid MBI is also expected. To the best of our knowledge, this sigmoid curve model of “functional decline after hip fracture”(Figure 2) was never proposed in the literature. Unfortunately, the ideal sigmoid curve was not well demonstrated in our statistical analysis, possibly due to insufficiently large sample size. Verifying this hypothetical curve is the future direction of research by our rehabilitation team.
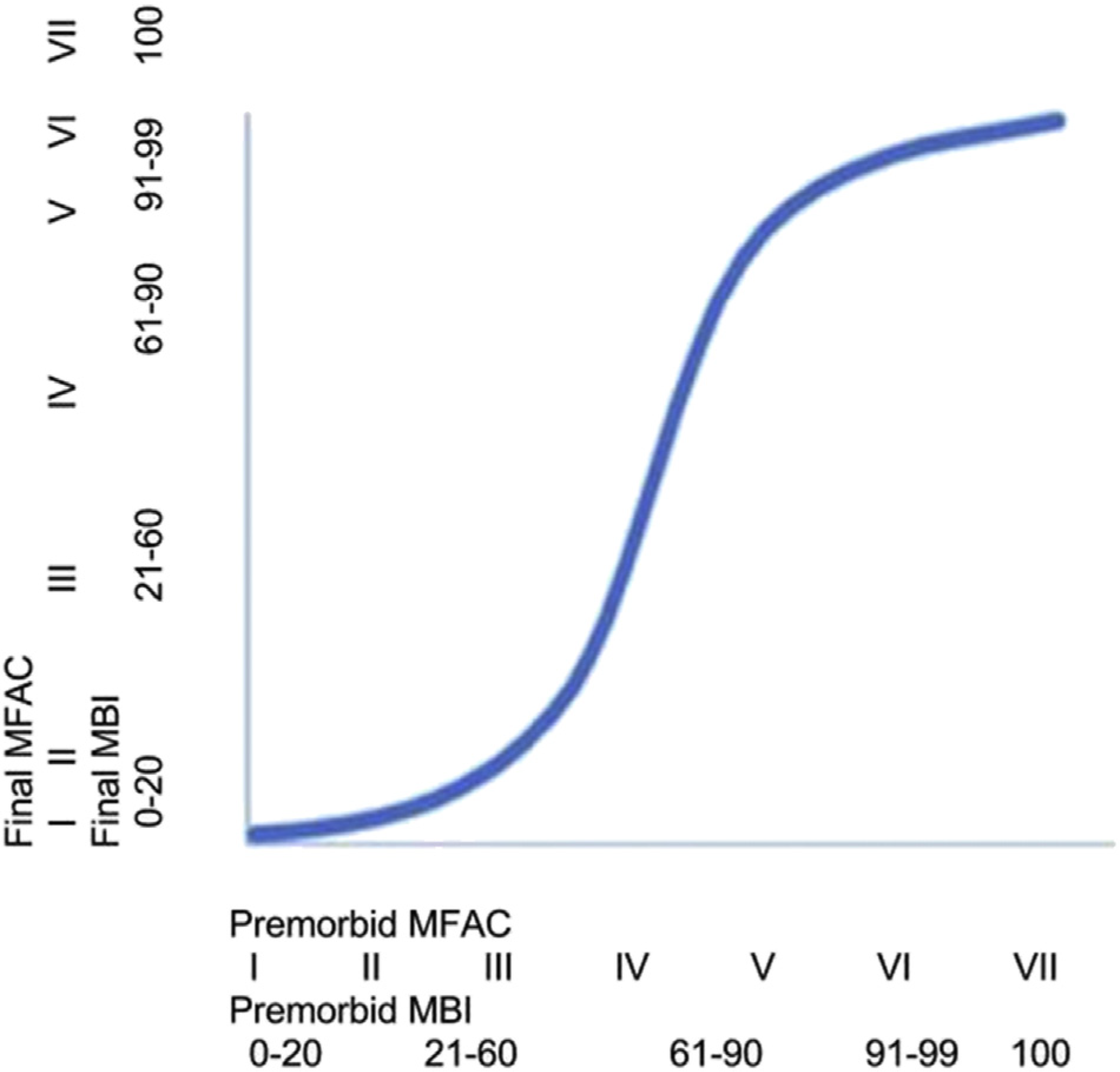
Functional decline after hip fracture. MFAC = Modified Functional Ambulation Category; MBI = Modified Barthel Index.
Limitations
There are several limitations in our study. It is a historical cohort study but not a prospective study. The sample size is reasonable but not large because our study is purposefully piloting before a largescale prospective cohort study. Both MFAC and MBI were assessed by different therapists. There might be recall bias in assessing premorbid MFAC and MBI, whereas other biases were insignificant because of good interrater reliability of the assessment tools. It was assumed that cognitive status remained the same on discharge (as perioperative stroke was excluded and delirium eventually resolved), and it is not routinely reassessed. The psychosocial factors of patients affecting total length of stay and discharge destination were not measured and actually unquantifiable. On one hand, whether patients could be discharged early and return home depends heavily on social support from their family. On the other hand, functional outcomes and social support are independent to each other. To reiterate, our stratification aims to select those who will have less functional decline, so that this group of patients will be more likely to ambulate and perform ADL as much as their premorbid functional status, without additional social support, making direct discharge from acute hospital a possible clinical pathway.
Conclusion
Hip fracture patients with good premorbid functional status in terms of MFAC, MBI, HK MoCA 5-Min and FPPS have significantly less functional decline and more likely to return home. Further prospective cohort study is recommended to verify our proposed clinical pathway and functional decline curve.
Footnotes
Conflicts of interest statement
The authors declare that they have no financial or nonfinancial conflicts of interest related to the subject matter or materials discussed in the manuscript.
Acknowledgements
The authors would like to thank Dr Lee Yuen-Lun and Dr Leung Yuen-Fai for their great support in this study and all the physiotherapists and occupational therapists in Tseung Kwan O Hospital and Haven of Hope Hospital for patient assessment and data collection.