
Abstract
Objective
To compare the functional status and quality of life (QoL) between patients who underwent an early mobilization scheme and those who underwent a late mobilization scheme after hip fracture fixation surgery in elderly Chinese patients.
Methods
This was a prospective cohort study. Patients (≥65 years old) with unstable intertrochanteric fractures treated with intramedullary nails were recruited from nine centers in China. Study centers either performed early mobilization or late mobilization scheme. All patients performed immediate in-bed mobilization after surgery and followed a standardized daily exercise program at home during the first 12 weeks. Functional status was measured by the Modified Barthel Index at postoperative visit, 6 weeks, and 12 weeks. QoL was measured by the EuroQol-5D (EQ-5D) at 12 weeks.
Results
One hundred and forty-eight patients were enrolled to early mobilization, and 136 to late mobilization. At 6 weeks, early mobilization resulted in a significantly better Modified Barthel Index than late mobilization (mean [SD]: 83.7 [12.0] vs. 67.0 [17.5], p < .001). Adjusted mixed effects model showed significantly higher Modified Barthel Index for early mobilization at postoperative visit, 6 weeks, and 12 weeks (all p < .001). Patients in the early mobilization group had slightly better EQ-5D Index at 12 weeks than patients in the late mobilization group (mean: 0.91 vs 0.87, p = .002).
Conclusions
Early postoperative mobilization resulted in better functional outcomes up to 12 weeks. QoL was rated statistically significantly better in the early mobilization group, but the difference was small and may not be clinically relevant.
Introduction
The primary goal of treating hip fractures in previously ambulatory elderly patient is to establish a functional painless limb as quickly as possible. With modern hip fracture fixation devices, the stability achieved by the fixation construct should allow for early mobilization. Since 1997, 5 studies, including one randomized controlled trial (RCT), investigated the time to mobilization (ambulation) after hip surgery and its effects on different outcomes such as mortality and function.1–5 All five studies found that early mobilization or short immobilization is more beneficial than delayed mobilization. Such benefits include better function at different time points,3–5 a higher probability of being discharged directly home,1,3 less bed rest–related complications,1,2 shorter length of hospital stay,1–3 and lower mortality at 6 months1,4 It is unclear whether in-house mobilization and physiotherapy is more effective than home-based therapy. Early discharge from hospital and dedicated home-based care programs appear to generate slightly better short-term outcomes, while a longer hospital stay may be associated with lower mortality.6–11
There is currently no consensus on what constitutes early mobilization after hip surgery. Different studies may use different time intervals to define “early” and “late” mobilization. Worldwide, regional differences exist with respect to how to integrate early mobilization into rehabilitation programs and clinical care pathways.12,13 In China, the general practice is rather conservative, and more than 30 days of delay in weight-bearing exercise has been reported. These could be due to multiple factors such as differences in clinical management, patients' psychosocial function or fear of falling, and patients' mobility habits.
The primary objective of this study was to compare the functional status of patients who underwent a pre-defined early mobilization scheme followed by a standardized home-based rehabilitation program after hip fracture fixation to those who underwent a late mobilization scheme in elderly Chinese patients. Secondary objectives were to compare quality of life (QoL), length of hospital stay, and adverse events (AEs) between the two mobilization schemes.
Materials and methods
Study design and patient population
This was a multicenter prospective cohort study. Patients were recruited from nine study centers in China between April 2015 and April 2017. Inclusion criteria were (1) 65 years and older, (2) sustaining an unstable intertrochanteric fracture (AO/OTA 31-A2 or 31-A3), (3) treated with fracture fixation of an intramedullary nail, (4) able to walk independently or with a walking aid before injury, and (5) willing to provide written informed consent. Patients were excluded if any of the following criteria were met: (1) severe dementia, (2) a history of substance abuse that precluded reliable assessment, (3) prisoners, and (4) participating in another study that could influence the results of this study. The study protocol was approved by the ethics committees of each study center. All patients provided written informed consent prior to study procedures. The study is registered on ClinicalTrials.gov with the number NCT02296086.
Mobilization schemes
Patients were recruited from two types of clinics: those implementing early mobilization scheme (early mobilization group) and those implementing late or standard mobilization scheme (late mobilization group) after hip fracture fixation. Early mobilization scheme was defined as transferring from bed to a sitting chair within 2 days after surgery, standing up with both feet on the ground within 4 (±2) days after surgery, and walking (walking aids allowed) starting within 5 (±2) days after surgery. Late mobilization scheme was defined as weight-bearing walking (with or without walking aids) starting more than 7 days after surgery as per local standard. Patients in both groups performed immediate in-bed mobilization after surgery. After discharge, all patients followed a standardized daily exercise program at home during the first 12 weeks. The total follow-up time was 1 year from the day of surgery. The postoperative visit was performed 4 (±2) days after the surgery. Patients attended clinic follow-up visits at 6 and 12 weeks. The 1-year visit was conducted via a telephone interview.
Primary outcome
The primary outcome was patients' functional status evaluated by the Modified Barthel Index14–16 at 6 weeks after surgery. The Modified Barthel Index comprises 10 component questions, each of which describes a daily activity. 15 Each activity is scored on a five-point ordinal scale which varies from item to item. The final score is calculated as the sum of all component questions and ranges from 0 to 100, with higher scores for greater functional independence. The structural validity and reliability of the Chinese version have been previously demonstrated. 17 For this study, if answers to any of the component question were missing, the total score was set to missing. The Modified Barthel Index was also measured at the postoperative and 12-week visit. Preinjury values for the Modified Barthel Index were collected retrospectively at the postoperative visit.
Secondary outcomes
QoL was evaluated with the three-level EuroQol-5D 18 (EQ-5D) at 12 weeks. Preinjury values of EQ-5D were collected retrospectively at the postoperative visit. The EQ-5D consists of a visual analog scale (VAS) and a descriptive system. 19 The VAS records the patients' self-rated health status on a graduated (0–100) scale, with higher scores for better QoL. The descriptive system comprises five dimensions of health (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and can be converted into an index score by applying scores from the EQ-5D value set elicited from the general population. The EQ-5D Index score ranges from 0 (dead) to 1 (perfect health), although negative values are possible. For this study, the Chinese value set 20 was used to convert to the EQ-5D Index score, and when missing values were present for any of the dimensions, the index value was set to missing.
Other secondary outcomes were length of hospital stay and the mobilization status during hospitalization and at 12 weeks. AEs occurring during the 1-year follow-up were recorded.
Sample size calculation
The sample size calculation was based on the minimal clinical important difference (MCID) of 10 in the mean Modified Barthel Index at 6 weeks between the study groups (μearly mobilization group = 85 and μlate mobilization group = 75). With a significance level of 5%, a power of 80%, an expected standard deviation (SD) of 25, and an allocation ratio of 1:1, we calculated a sample size of 198 patients (99 per group). Assuming an attrition rate of 20%, a total of 248 patients (124 per group) were required.
Statistical analyses
The full analysis population included all enrolled patients who were eligible and started the mobilization scheme. The per protocol population was a subset of the full analysis population and was limited to patients with no major deviations, who were compliant to their assigned mobilization schemes, and in whom study assessments were within the pre-defined visit windows.
We used univariable statistical tests to evaluate differences between the two groups in sociodemographic data, smoking and drinking habits, comorbidities, and injury-related characteristics. The primary endpoint was the difference in Modified Barthel Index at 6 weeks between the two groups, analyzed by a one-sided two-sample Welch’s t-test with a margin of 10, which is the MCID of Modified Barthel Index. We used mixed effects linear regression models to analyze and compare between the two groups the changes of Modified Barthel Index (postoperative visit, 6 weeks, and 12 weeks) and EQ-5D (preinjury and 12 weeks) with adjustments of the following potential confounding factors: age, sex, Charlson Comorbidity Index, 21 AO/OTA Fracture and Dislocation Classification, 22 and implant type. For the model of Modified Barthel Index, preinjury values of Modified Barthel Index were also used for the adjustment. The models included the fixed categorical effects of treatment, visit, and treatment-by-visit interaction. The models were calculated using unstructured covariance (on patient level) and fitted using restricted maximum likelihood estimation. We performed subgroup analyses to examine whether changes of Modified Barthel Index depended on sex and age group. Descriptive statistics were used to summarize patients' mobilization status during hospitalization and at 12 weeks as well as AEs occurring during the 1-year follow-up. Fisher’s exact test was used to compare the risk of having at least one AE between the two groups.
Apart from the Welch’s t-test, all statistical tests were two-sided and based on adjusted least-squares means with a 5% significance level. Analyses were performed using SAS software (version 9.4, SAS Institute Inc, Cary, North Carolina).
Results
Patient disposition and baseline characteristics
A total of 284 eligible patients were enrolled, 148 in the early mobilization group and 136 in the late mobilization group. Patients in the early mobilization group were less compliant to their mobilization scheme than those in the late mobilization group (54.7% [81/148] vs. 91.9% [125/136]). During the 1-year study, 29 patients dropped out, 5 from the early mobilization group and 24 from the late mobilization group. Reasons for dropout and numbers of patients available throughout the study are provided in Figure 1. Five patients from the early mobilization group and three from the late mobilization group died during the 1-year study period. Flowchart of patient enrollment and follow-up.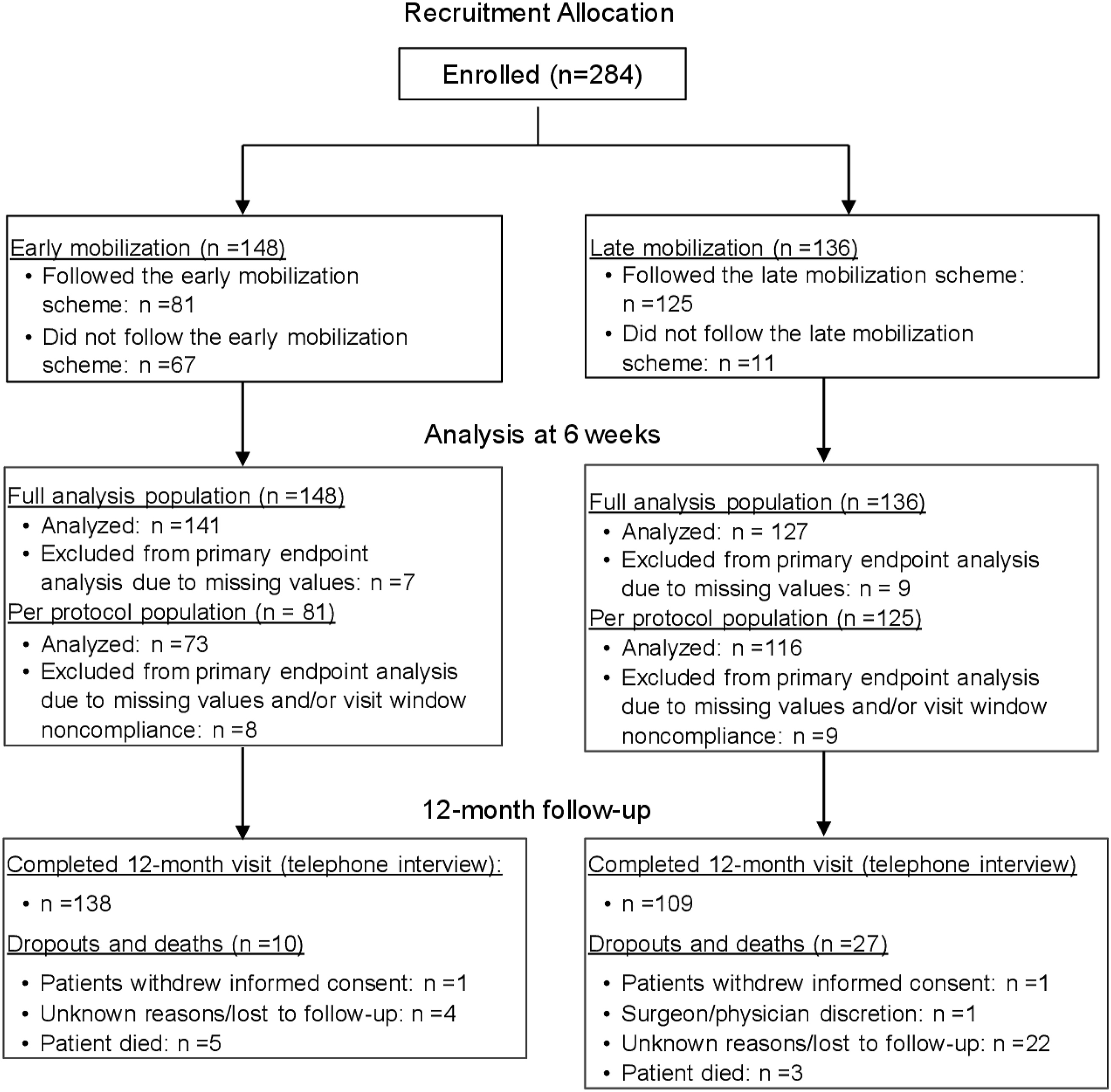
Sociodemographic characteristics, comorbidities, and injury details.
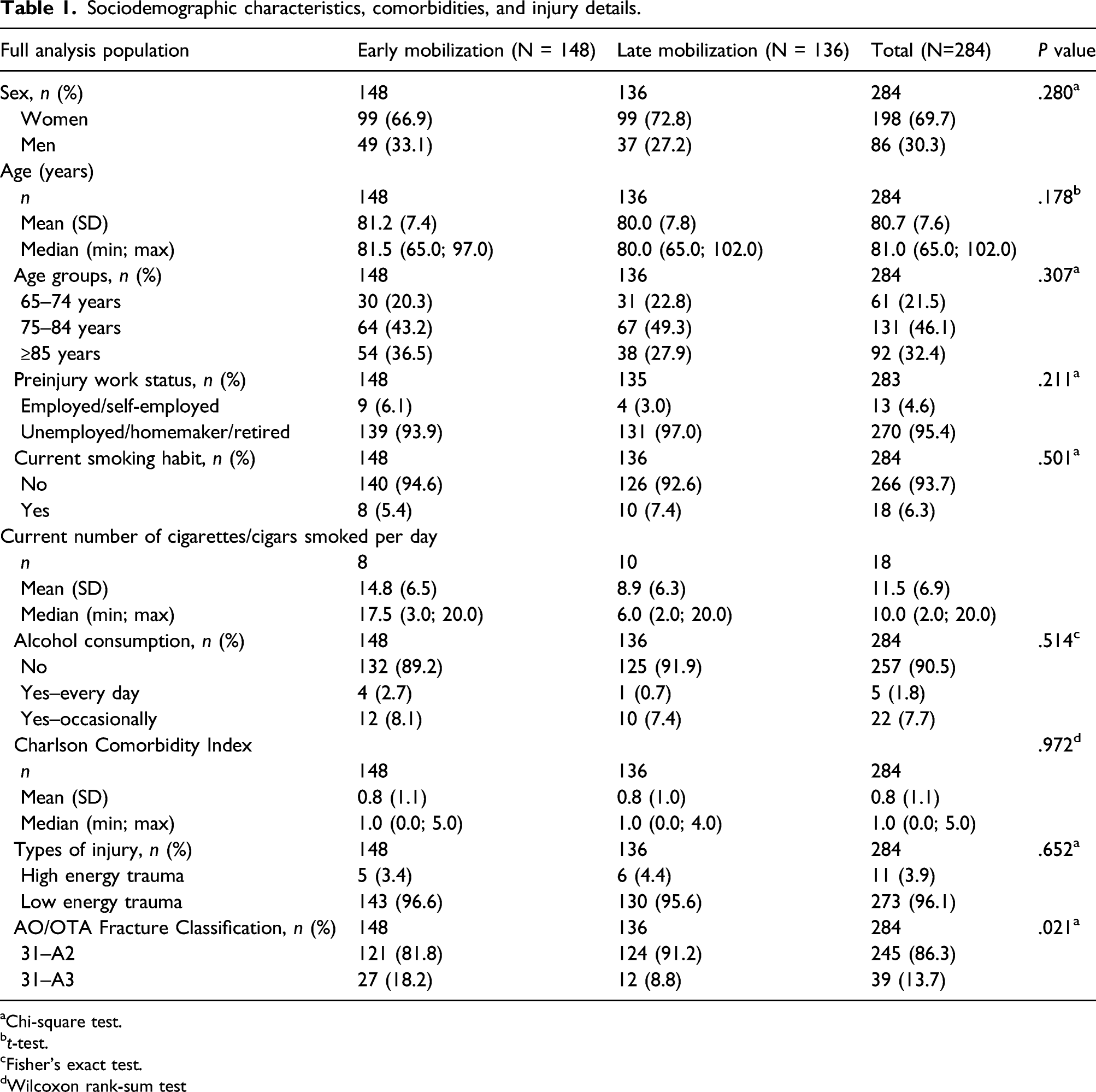
aChi-square test.
bt-test.
cFisher's exact test.
dWilcoxon rank-sum test
Modified Barthel Index
Modified Barthel Index at 6 weeks.
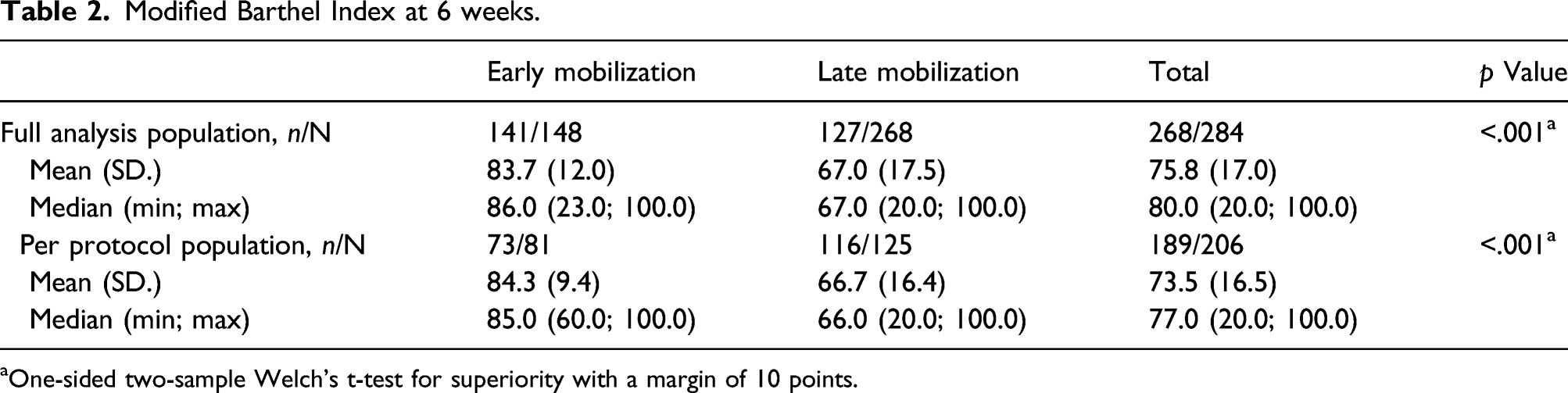
aOne-sided two-sample Welch’s t-test for superiority with a margin of 10 points.
Mixed effects linear regression models analyzing changes in the Modified Barthel Index over the course of follow-up, adjusting for age, sex, Charlson Comorbidity Score, AO/OTA Fracture Classification, and the preinjury Baseline Modified Barthel Index.

CI: confidence interval.
ap value comparing mean values at each visit between the treatment groups.
bp value comparing change from postoperative visit within each treatment group.
Mixed effects linear regression models of subgroup analyses of Modified Barthel Index over the course of follow-up by sex and age group after adjusting for age, Charlson Comorbidity Score, AO/OTA Fracture Classification, implant type, and the preinjury Modified Barthel Index in the full analysis population.

CI: confidence interval.
ap value comparing change from postoperative visit within each group.
bp value comparing mean values at each visit between the two groups.
Quality of life
Mixed effects linear regression modeling analyzing changes in EQ-5D VAS and EQ-5D Index over the course of follow-up, adjusting for age, sex, Charlson Comorbidity Score, AO/OTA Fracture Classification, and implant type.

CI: confidence interval.
ap value comparing mean values at each visit between the two groups.
bp value comparing change from preinjury visit within each group.
Other secondary outcomes
In-hospital mobilization in the full analysis population.

Mobilization status at 12 weeks.

aDerived from a combination of data from patients for whom the exact date of (partial) weight bearing (with or without walking aids) was known and for whom the exact date was not known but only time frames were available. Patients who did not start (partial) weight bearing at all were not included.
bCochran-Armitage test for trend.
Summary of adverse events on adverse event level.

Discussion
We confirmed our hypothesis and showed that patients with a hip fracture who were mobilized early after surgery had a better functional status 6 weeks after surgery than patients who were mobilized later, with a difference in mean Modified Barthel Index of 16.7 between the two groups (p < .001). Patients in the early mobilization group still performed better after 12 weeks than patients in the late mobilization group despite suffering more severe fractures. Notably, both groups showed significant improvement in their functional status up to 12 weeks (p <.001). A 12-week follow-up should better reflect the impact of the mobilization scheme than a later time point which could be confounded by other factors such as patients' mobility habits. QoL measured by EQ-5D was overall good. Unlike the patients in the late mobilization group, patients in the early mobilization group did not return to their preinjury level of EQ-5D Index. We found no differences in the length of hospital stay and risk of AEs between the two groups. Upon following the standard of care, mobilization was indeed earlier in the early mobilization group than in the late mobilization group.
Early mobilization positively impacts the functional status up to 12 weeks after surgery, especially in the elderly. Our results confirm the results of earlier studies, in which patients' age and measures of the functional status were different from ours. Oldmeadow et al. 3 conducted an RCT in 60 patients (mean age [range]: 79.4 years [53–95]) who underwent surgical fixation of an acute femoral neck fracture. Patients were randomized to the early ambulation group where they walked for the first time on postoperative day 1 or 2 or to the delayed ambulation group where they only started walking on postoperative day 3 or 4. All patients were transferred to sitting out of bed as early as possible after surgery. They found that patients in the early ambulation group walked further than those in the delayed ambulation group (p = .03) 1 week after surgery and required less assistance to transfer (p < .01) and walk a step (p = .23). 3
In a cross-sectional analysis of data from the English National Hip Fracture Database, Su et al. 5 found that mobilization, defined as sitting or standing out of bed on the day of surgery or the following day, was associated with better mobility 30 days after discharge in patients aged 60 years and older. The authors used a 30-day mobility score to measure mobility with higher scores for less mobility. 5 A cohort study in 532 patients with hip fractures aged 50 years and older found that patients with a shorter duration of immobility (2.0 days) had a significantly better mean (95% CI) Functional Independence Measure score for locomotion than patients with longer immobility (a duration of 8.3 days; 7.2 [6.7; 7.6] vs. 6.2 [5.7; 6.6], p < .01) at 2 months but not at 6 months (short vs. long immobility: 8.4 [8.0; 8.9] vs. 7.8 [7.4; 8.3], p = .14). 4
Our data did not show further benefits for the earlier mobilized patients such as earlier discharge from the hospital and fewer AEs or deaths, especially bed rest– and hospital-related AEs. We found statistically significant differences between the two groups in EQ-5D Index scores at preinjury and 12 weeks. Walters and Brazier reported a mean (range) MCID of 0.074 (−0.011; 0.140) for the EQ-5D Index 23 and therefore the differences found in our study may not be clinically relevant.
The study has several limitations. First, the main limitation of our study is the observational design. Treatment assignment was on the study center level. Patients were allocated to study groups by admission to either a clinic that performed early mobilization or late mobilization. No randomization was performed. Analyses of baseline characteristics showed that the two groups differed significantly in fracture severity. Between-group differences in other characteristics that were not measured in the study could not be excluded. This reflects the limitation of an observational design in addressing clinical questions related to the efficacy of a certain therapy. Second, the findings from the full analysis population were subjected to the bias due to the uneven rate of compliance to the allocated mobilization schemes between the two groups. Therefore, the analyses using the per protocol population were conducted to test the robustness of the findings. Results from these two sets of analyses were consistent. Patients in the early mobilization group were less likely to adhere to the allocated mobilization scheme. The most common reasons were pain and unfit general condition. This reflects that even under the principle of early mobilization, the best care should still be adapted according to the patients’ condition. Third, the follow-up rate at 1 year was lower in the late than in the early mobilization group (80.1% [109/136] vs. 93.2% [138/148]). As the occurrence of AEs was assessed within 1 year after surgery, this uneven follow-up rate could have led to an underestimated risk of AE in the late mobilization group. Most of the losses to follow-up in the late mobilization group occurred in one study site. This indicated data missing not at random, which could potentially introduce selection bias and influence the study validity. 24 Fourth, preinjury Modified Barthel Index and QoL could only be assessed retrospectively as patients were recruited after the injury. However, in all cases, the preinjury values were collected retrospectively within a few days after injury; therefore, the recall bias should have little effect. There was a 2.1 difference in the mean of preinjury Modified Barthel Index between the study groups. To address this issue, we considered the preinjury Modified Barthel Index as a confounding factor and used it as a covariate for adjustment in the mixed effects models. Fifth, both the caretaker and the patient could fill in the EQ-5D, and several questionnaires had been completed by two different persons. Sensitivity analyses including only data completed by the same person at preinjury and at 12 weeks showed similar conclusions (data not shown). Finally, our study was conducted in several tertiary healthcare centers in China. Quality of healthcare provided in these centers might not be representative of that provided by primary or secondary healthcare centers. Future randomized controlled trials that recruit patients from healthcare centers of different levels are needed to confirm our results.
A major strength of the study was the overall good execution, which increased the quality of our data. Recruitment after the start of the study went largely according to plan, and the sample size was achieved. The overall follow-up rate remained higher than 87% throughout the study visits, with a high visit window compliance (≥90%) and a lower-than-expected dropout rate (10.2%).
Conclusions
In conclusion, in Chinese patients with unstable intertrochanteric fracture undergoing intramedullary nail fixation, early postoperative mobilization resulted in better functional outcomes up to 12 weeks without increasing the risk for AEs. Self-perceived QoL was rated statistically significantly better in the early mobilization group but the difference may not be clinically relevant.
Footnotes
Acknowledgments
The authors would like to thank Christian Knoll and Sergey Burnos (AO Innovation Translation Center [AO ITC], AO Foundation) for statistical analysis and Andrea Blumenthal (Fitji Healthcare Communications) and Tracy Y Zhu (AO ITC, AO Foundation) for medical writing services.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the AO Foundation via AO Trauma. Leung F has received reimbursement of traveling costs and lecture fees from AO Trauma.
Data availability statement
The datasets used and/or analyzed during the current study can be made available from the corresponding author/sponsor on reasonable request.