
Abstract
Introduction
Surgical fixation of hip fractures in older adults is associated with significant morbidity and mortality. We investigated whether regional anesthesia, which excluded epidural, spinal, or combined epidural-spinal, was associated with lower postoperative complication rates compared to general or spinal anesthesia in patients aged 50 years and older undergoing hip fracture surgery.
Methods
A retrospective analysis was conducted using the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) Targeted Hip Fracture dataset from January 1, 2016, to December 31, 2022. Propensity score matching was used to compare regional anesthesia with general and spinal anesthesia. Given the NSQIP database excludes epidural, spinal, and combined epidural-spinal anesthesia from the regional classification, it was presumed that the remaining regional anesthesia patients received a peripheral nerve block. The primary outcome measure was a 30-day composite of death, myocardial infarction, or stroke.
Results
The study analyzed 54,623 patients, from which 323 received regional anesthesia. These were separately matched with 323 cases of general anesthesia and 323 cases of spinal anesthesia. Regional anesthesia was associated with a lower incidence of the primary composite outcome compared to both general anesthesia (3% vs 7%, risk ratio 0.3, 95% CI: 0.2 to 0.6, P < 0.001) and spinal anesthesia (3% vs 7%, risk ratio 0.5, 95% CI: 0.3 to 0.9, P = 0.01). A subgroup effect was detected, with high-risk patients (ASA IV–V) experiencing the greatest protective benefit from regional anesthesia.
Conclusions
Regional anesthesia techniques, excluding epidural, spinal, or combined epidural-spinal techniques, were associated with lower rates of major postoperative complications in older adults undergoing hip fracture surgery compared to general or spinal anesthesia. This benefit was more pronounced in high-risk patients. Our findings suggest that regional anesthesia, most likely administered via a peripheral nerve block, may offer benefits beyond pain control in this population, potentially improving postoperative outcomes.
Keywords
Introduction
Hip fractures in older adults pose a significant healthcare challenge, often resulting in substantial morbidity and mortality. 1 The choice of anesthesia for hip fracture surgery can significantly affect a patient’s postoperative outcomes and risk of complications. Traditionally, general and spinal anesthesia have been the primary choices for this surgery.2,3 However, peripheral nerve blocks are emerging as a promising alternative or adjunct, potentially offering benefits beyond perioperative pain control. 4
Peripheral nerve blocks are an established modality for managing acute pain, but the broader impact on clinical outcomes, especially in high-risk patients, remains uncertain. 5 To address this knowledge gap, a retrospective analysis was conducted using the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) Targeted Hip Fracture dataset. Previous studies using this database have focused on comparing spinal and general anesthesia in older adults with hip fractures.3,6 However, the NSQIP database contains data on several additional anesthesia techniques that these studies did not examine. While the database has no specific category for peripheral nerve blocks, the ‘regional anesthesia’ treatment variable in NSQIP excludes epidural, spinal, combined epidural-spinal techniques, and local anesthesia, thus suggesting that NSQIP reporting of regional anesthesia most likely represents predominantly peripheral nerve blocks. 7
The primary objective of this study was to estimate the effect of peripheral nerve blocks by comparing the association between postoperative complication rates of older adults who received NSQIP-reported regional anesthesia vs those who received either general or spinal anesthesia for hip fracture surgery. The study hypothesized that older adults receiving regional anesthesia as their primary anesthetic for hip fracture surgery would have a lower 30-day incidence of a composite outcome mortality, myocardial infarction (MI), or stroke compared to those receiving either general or spinal anesthesia.
Methods
Data Source
This study was a retrospective analysis of data from the ACS NSQIP Targeted Hip Fracture dataset. The analysis included data from the ACS NSQIP 2022 Participant Use Data File (PUF), selecting patients aged 50 years or older who underwent hip fracture surgery. The ACS NSQIP database is a comprehensive resource that tracks patient demographics, preoperative risk factors, surgery type, primary anesthesia type, and postoperative outcomes for 30 days after surgery. 7 The reliability of the data is ensured by trained and certified surgical clinical reviewers who use standardized methods to extract information from medical records. The research was exempt from Institutional Review Board review.
Study Population
This study analyzed data from 54,623 patients aged 50 years and older who underwent hip fracture surgery between January 1, 2016, and December 31, 2022. The ACS NSQIP Target Hip Fracture database identifies these procedures using specific Current Procedural Terminology (CPT) codes: 27236, 27244, and 27245. The database categorizes primary anesthetic techniques as general, epidural, spinal, combined spinal-epidural, regional, monitored anesthesia care (MAC), intravenous (IV) sedation, or local. 7 At case completion, anesthesiologists record one primary anesthetic technique for billing purposes. For cases involving multiple techniques, the database follows a reporting hierarchy: general anesthesia takes precedence when used with any other technique, followed by neuraxial, and other techniques are designated as primary only when serving as the main anesthetic method. 7 Since all neuraxial techniques are categorized separately, the ‘regional anesthesia’ designation in the database is presumed to be a reliable surrogate description for peripheral nerve blocks. Exclusion criteria for the study were patients under 50 years of age, cases where anesthesia type was not reported, patients who received primary anesthesia with combined spinal-epidural, epidural anesthesia, local anesthesia, or MAC, and patients with incomplete perioperative data.
A comprehensive set of baseline patient characteristics and risk factors were extracted from the database. These included demographic information (age, sex, race, and body mass index), lifestyle factors (smoking status), and various medical conditions (diabetes mellitus, chronic obstructive pulmonary disease, congestive heart failure, hypertension, acute renal failure, current dialysis status, bleeding disorders, preoperative dementia or delirium, and disseminated cancer). Important anesthetic and surgical factors such as ASA classification, functional status, and type of hip fracture (nondisplaced femoral neck fracture, displaced femoral neck fracture, intertrochanteric, and subtrochanteric) were extracted. To ensure consistency and reliability in data interpretation across the study, all variables were defined according to the standardized definitions provided in the NSQIP User Guide.
Outcomes
The primary outcome measure was a composite endpoint consisting of death, MI, or stroke occurring within 30 days post-surgery. These outcomes were defined according to the NSQIP database criteria, with MI characterized by new Q waves on electrocardiogram or typical symptoms with elevated cardiac enzyme, and stroke is defined as a cerebral event resulting in persistent neurological dysfunction. This composite outcome was selected to maintain consistency with previous NSQIP research comparing anesthetic techniques in hip fracture surgery, facilitating direct comparison between studies. 3 Additionally, it captures major adverse events affecting patient health and its established use as a standard measure in high-risk surgeries among older adults.3,8,9
A comprehensive set of secondary outcomes was evaluated to provide a more complete picture of patient experiences following hip fracture surgery with different anesthesia types. These included the incidence of specific postoperative complications, including mortality, stroke, MI, pneumonia, pulmonary embolism, deep vein thrombosis, sepsis, postoperative delirium, and surgical site infections. The analysis included several perioperative and recovery-related factors. These included the duration of the surgical procedure, reoperation rates, length of hospital stay, and discharge disposition.
Statistical Analysis
Sample size calculation showed that 680 patients would provide 70% power to detect a decrease in the primary composite outcome from 10% to 5% at a significance level of 5%. We performed propensity score matching to create two separate comparison cohorts: one comparing regional anesthesia to general anesthesia and another comparing regional anesthesia to spinal anesthesia. Propensity score matching was used to balance potential confounding factors between anesthesia cohorts, including patient demographics (age, sex, race), comorbidities (eg, hypertension, diabetes, chronic obstructive pulmonary disease), clinical factors (type of hip fracture), and surgical characteristics (eg, type of procedure performed). In both cohorts, we used 1:1 optimal matching without replacement using probit regression models. Covariate imbalance before and after matching was assessed using standardized means differences, achieving between-group differences of 0.20 or less. 10 Outcome models were fit using logistic or linear regression, depending on the outcome distribution. Each model included treatment by covariate interactions for double robust estimators if there were an adequate number of events for model convergence. For low-event models, only the treatment indicator within the matched cohort was included. Model parameters were used to calculate average marginal effects with clustered standard errors and reported binary outcomes as risk ratios and continuous outcomes as mean differences with 95% confidence intervals. The threshold for statistical significance was alpha = 0.05. No adjustments were made for multiple testing, and therefore, all secondary outcomes are interpreted as exploratory. For the subgroup analyses, the treatment indicator was interacted with the ASA classification and reported the primary endpoint results stratified by the ASA classification. All statistical analyses were performed using R Version 4.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Regional Anesthesia versus General Anesthesia Patient Characteristics by Treatment Group before and after Matching
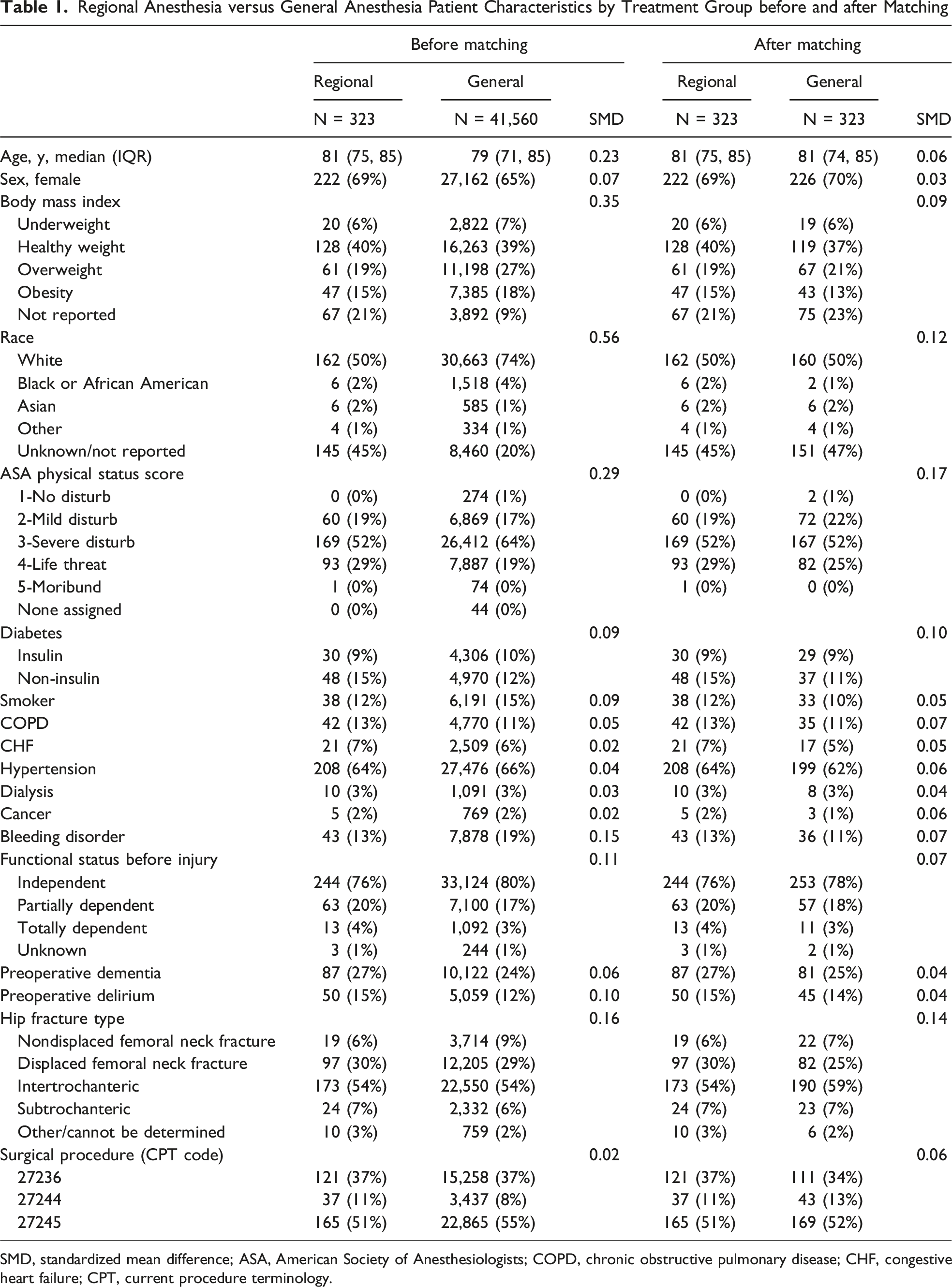
SMD, standardized mean difference; ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; CPT, current procedure terminology.
Association of Regional Anesthesia Versus General Anesthesia on Study Outcomes
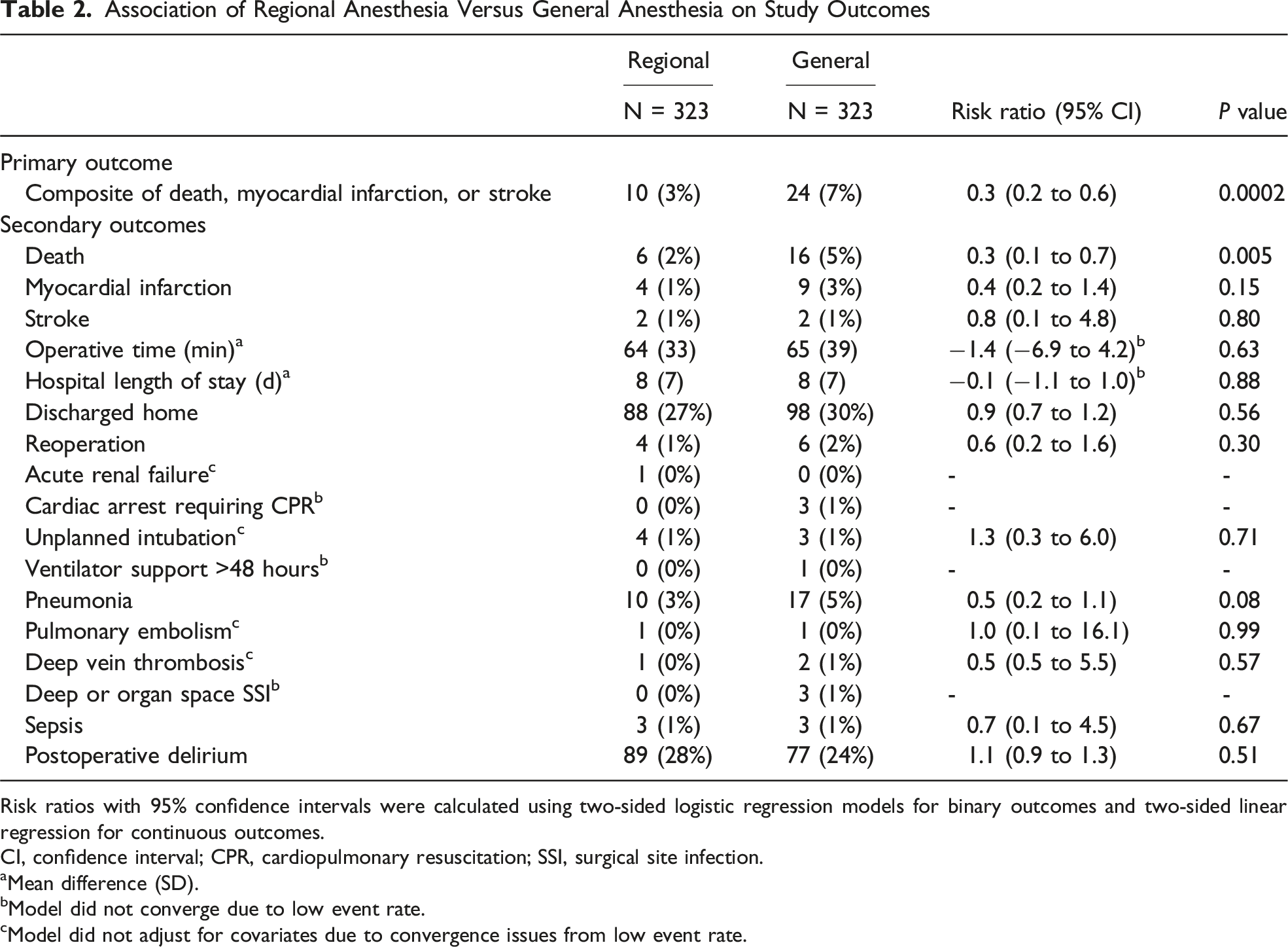
Risk ratios with 95% confidence intervals were calculated using two-sided logistic regression models for binary outcomes and two-sided linear regression for continuous outcomes.
CI, confidence interval; CPR, cardiopulmonary resuscitation; SSI, surgical site infection.
aMean difference (SD).
bModel did not converge due to low event rate.
cModel did not adjust for covariates due to convergence issues from low event rate.
Regional Anesthesia vs General Anesthesia
Regional Anesthesia Versus Spinal Anesthesia Patient Characteristics by Treatment Group Before and After Matching

SMD, standardized mean difference; ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease; CHF, congestive heart failure; CPT, current procedure terminology.
The stratified analysis of the primary outcome by ASA classification consistently favored regional anesthesia over general anesthesia for older adults with hip fractures across all risk groups (Figure 1). High-risk patients with the most severe baseline comorbidities (ASA IV–V) benefited the most from regional anesthesia, showing significantly lower postoperative event rates (3%) compared to general anesthesia (16%) (RR 0.2, 95% CI: 0.1 to 0.5, P < 0.001). Low-risk (ASA I–II) and moderate-risk (ASA III) patients had fewer events with regional anesthesia, but these differences were not statistically significant due to wide CIs. Association of Regional Anesthesia Versus General Anesthesia on the Composite Endpoint of Death, Myocardial Infarction, and Stroke Within 30 Days, Stratified by ASA Physical Status Score. Statistical Comparisons Were Performed Using Two-Sided Stratified Logistic Regression Models.
Regional Anesthesia vs Spinal Anesthesia
Association of Regional Anesthesia Versus Spinal Anesthesia on Study Outcomes

Statistical comparisons were performed using two-sided stratified logistic regression models.
aMean difference (SD).
bModel did not converge due to low event rate.
cModel did not adjust for covariates due to convergence issues from low event rate.
A stratified analysis of the primary outcome by ASA classification, comparing regional anesthesia to spinal anesthesia, suggests that the benefits of regional anesthesia increase with patient risk (Figure 2). High-risk patients (ASA IV–V) had even greater benefits with regional anesthesia compared to spinal anesthesia (3% vs 11%; RR 0.3, 95% CI: 0.1 to 1.0, P = 0.04). Intermediate-risk patients (ASA III) showed point estimates favoring regional anesthesia, but comparisons did not reach statistical significance. Low-risk patients (ASA I–II) had identical event rates (2%) for both techniques. Association of Regional Anesthesia Versus Spinal Anesthesia on the Composite Endpoint of Death, Myocardial Infarction, and Stroke Within 30 Days, Stratified by ASA Physical Status Score. Statistical Comparisons Were Performed Using Two-Sided Stratified Logistic Regression Models.
Discussion
Peripheral nerve blocks, a form of regional anesthesia, may provide benefits beyond acute pain management in hip fracture surgery for older adults. Patients receiving this type of regional anesthesia had lower rates of death, MI, and stroke compared to those receiving general or spinal anesthesia. Furthermore, the benefits of regional anesthesia were more pronounced in patients with severe systemic disease (ASA IV or V), suggesting this technique may be particularly beneficial for older hip fracture patients with multiple comorbidities.
The results align with previous research demonstrating that peripheral nerve blocks are beneficial in reducing adverse outcomes compared to other methods of analgesia.5,11 Morrison and colleagues’ multi-center trial of 153 patients showed that preoperative peripheral nerve blocks provided improved analgesia, reduced opioid-related side effects, and enabled earlier mobilization compared to oral and parenteral analgesic therapy. 4 Hamilton and colleagues’ population-based study observed a modest decrease in postoperative hospital length of stays with peripheral nerve block use, an effect believed to be driven by fewer postoperative complications. 11 The systematic review and meta-analysis by Guay and Kopp 5 strongly supported the use of peripheral nerve blocks for pain management in adults with hip fractures. Their findings demonstrated that peripheral nerve blocks effectively reduced preoperative pain and potentially decreased chest infections and acute confusion. 5 While these studies mostly report on PNB as multimodal anesthesia and analgesia, they highlight that PNB work differently than neuraxial and the mechanism alone, whether primary or multimodal will need further research to strengthen the evidence base, particularly regarding serious outcomes such as MI and mortality. 5
Our analysis extends the existing literature by demonstrating a potential protective effect of regional anesthesia, presumably peripheral nerve blocks, in high-risk patients (ASA IV or V) undergoing hip fracture surgery. The avoidance of systemic effects seen with general and spinal anesthesia suggests that regional anesthesia with a peripheral nerve block may offer benefits beyond pain control. This is particularly important in older adults whose impaired physiological reserves limit their ability to maintain homeostasis during the stress of fracture and surgery. Previous studies have shown that frailty and comorbidities can further impair adaptive and homeostatic responses to physiological instabilities, such as perioperative variations in blood pressure and pulse pressure in response to stress.12,13 The reduced adverse events in the high-risk regional anesthesia cohort may stem from targeted pain control and subsequent reduced physiologic stress. 12
Although regional anesthesia with a peripheral nerve block has established benefits for acute pain relief in hip fracture patients, its potential advantages beyond pain control warrant further investigation. 5 Of particular interest is its targeted sensorineural blockade, which reduces both afferent and efferent signaling between the injury site and the brain.4,14 This bidirectional blockade may offer wide-ranging benefits, including decreased central sensitization, reduced muscle spasms, reduced inflammatory response, improved blood flow, and modulated sympathetic and neuroendocrine responses to surgery. These effects potentially result in more stable hemodynamics, reduced catecholamine release, and better glycemic control, which could contribute to improved outcomes, particularly in high-risk patients. The modulated response may also offer organ-specific protection, especially for the cardiovascular, pulmonary, and renal systems. These findings highlight the need for further research to understand the mechanisms at play and to optimize regional anesthesia techniques. Future studies could expand this research by focusing on the type of nerve block, the use of continuous infusions, and long-term follow-up assessments of mortality and cardiovascular impacts.
This study has several notable strengths. It leverages the large, nationally representative ACS NSQIP Targeted Hip Fracture dataset to compare outcomes between common anesthesia types for hip fracture surgery in older adults. The assessment of covariate balance after propensity score matching suggests a similar distribution of potential confounders between the comparison groups, implying reduced biased treatment effect estimators. The clinically relevant primary outcome—a composite of death, MI, or stroke within 30 days—along with a comprehensive set of secondary outcomes, provides a thorough assessment of potential postoperative complications. Stratifying the analysis by ASA classification reveals a differential treatment effect with higher potential benefits for the sickest patients. Finally, conducting an analysis of regional anesthesia that excludes neuraxial anesthesia allows us to examine the likely benefits of peripheral nerve blocks.
This study has several limitations. While the separate categorization of other regional techniques strongly supports our assertion that regional anesthesia reported in the ACS NSQIP database represents peripheral nerve blocks, this interpretation lacks explicit confirmation in the database structure. Additionally, the database omits clinical details including specific peripheral nerve block types, timing of block placement relative to surgery, local anesthetic agents used, sedation methods, direct oral anticoagulants, and multimodal approaches combining peripheral nerve blocks with general or spinal anesthesia. These data limitations constrain the ability to estimate more complex treatment effects. Furthermore, despite using a large database, our assessments are based on a relatively small sample size. Although we used propensity matching, this is not a randomized trial and residual confounding can lead to imprecise treatment effect estimates. Regardless, if indication bias exists, higher-risk patients are typically more likely to receive peripheral nerve blocks, which would lead to a further underestimation of its benefits. Finally, despite our statistical adjustments, other unmeasured confounders, such as individual practitioner preference or experience, could influence both anesthesia choice and patient outcomes. Without clinical trial data, these sources of bias cannot be excluded. These limitations underscore the need for further research with larger sample sizes and more prospective data collection to more confidently measure the effect of peripheral nerve blocks as primary anesthetics on outcomes in hip fracture surgery.
Conclusion
This study found that regional anesthesia, presumably using peripheral nerve block techniques, may offer advantages beyond pain control, with potential protective benefits in high-risk hip fracture patients. While these results are promising, study limitations necessitate cautious interpretation. Future clinical trials should examine peripheral nerve block benefits beyond pain management, identify mechanisms of action, determine optimal techniques for different risk profiles, and assess long-term outcomes. By combining the insights from this study with carefully designed future research, researchers can work towards developing more effective, patient-centered approaches to anesthesia for older adults undergoing surgical fixation of hip fractures.
Footnotes
Acknowledgements
The authors would like to thank the American College of Surgeons National Surgical Quality Improvement Program and participating hospitals for their data.
Ethical Considerations
The research was exempt from University of Maryland Institutional Review Board review.
Author Contributions
AMT, GPS, and NNO contributed to conceptualization, investigation, project administration, and resources; NNO contributed to data curation, methodology, formal analysis, visualization; SG and RVO contributed to validation; all authors contributed to writing and review of the final work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this publication was partially supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number K24AR076445. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GPS is a paid consultant for Smith and Nephew and Zimmer, unrelated to this work. RES received an honorarium from Butterfly Inc. for evaluating an ultrasound probe, unrelated to this work. RVO is a paid consultant for Stryker, receives stock or stock options from Imagen, and receives royalties from Lincotek, all unrelated to this work. NNO receives stock or stock options from Arbutus Medical Inc., unrelated to this work.
Data Availability Statement
Study data will be made available upon reasonable request to the corresponding author.