
Abstract
The aims of this study were to identify the location of the A1 pulley combining palpation technique with superficial palm landmarks and to determine the efficacy and safety of A1 pulley percutaneous release with a 19-gauge needle. Fourteen fresh frozen cadaveric specimens were used: 56 fingers and 14 thumbs. The location of the A1 pulley was based on anatomical landmarks and was identified in all digits. Complete release of the A1 pulley occurred in 60 of the 70 digits (85.7%). The length of the A1 pulley in thumbs was 5.7 mm and in other fingers 4.5 mm. There were no signs of neurovascular bundle injuries. The mean distance between needle pathway and neurovascular bundle was 4.3 mm in the thumbs and 6.5 mm in the other fingers. There were no total flexor tendon injuries. The location of the A1 pulley can be predicted with success. Percutaneous release of the A1 pulley with a 19-gauge needle shows acceptable results in both safety and efficacy.
Keywords
Introduction
As shown in literature reviews, open surgical treatment for trigger finger is considered the gold standard, because it has high success and low complication rate. 1 –4 Percutaneous release of the A1 pulley has recently become an alternative method for treating trigger finger. However, lack of direct visualization of the A1 pulley, during release, has a greater risk of neurovascular bundle injury, tendons or partial release of the A1 pulley. 4 –6 The primary purpose of this study was to identify the location of the A1 pulley using superficial palm landmarks and palpation technique, and the secondary was to determine the efficacy and safety of A1 pulley percutaneous release with a 19-gauge needle in a cadaveric model.
Methods
Fourteen fresh frozen cadaveric specimens below the elbow were used. Knowledge of the typical location of the A1 pulley was based on anatomical landmarks described by Wilhelmi et al. 7 The proximal and distal palmar creases were marked. All digits were in slight abduction position (except middle finger). The midline of each finger was marked along the palm to the carpal tunnel through the palmar creases (Figures 1 and 2). The relative location of the A1 pulley was marked beneath a line drawn from the radial end of proximal palmar crease to the ulnar end of the distal palmar crease at the marked midline level (Figure 3). The palpation technique using surface landmarks palpation was performed along the marked A1 pulley combined with finger flexion and extension. The correct location of the A1 pulley can be felt at the point of the noticeable thickened structure. The A1 pulley location was marked combined with relative surface landmarks and palpation technique.
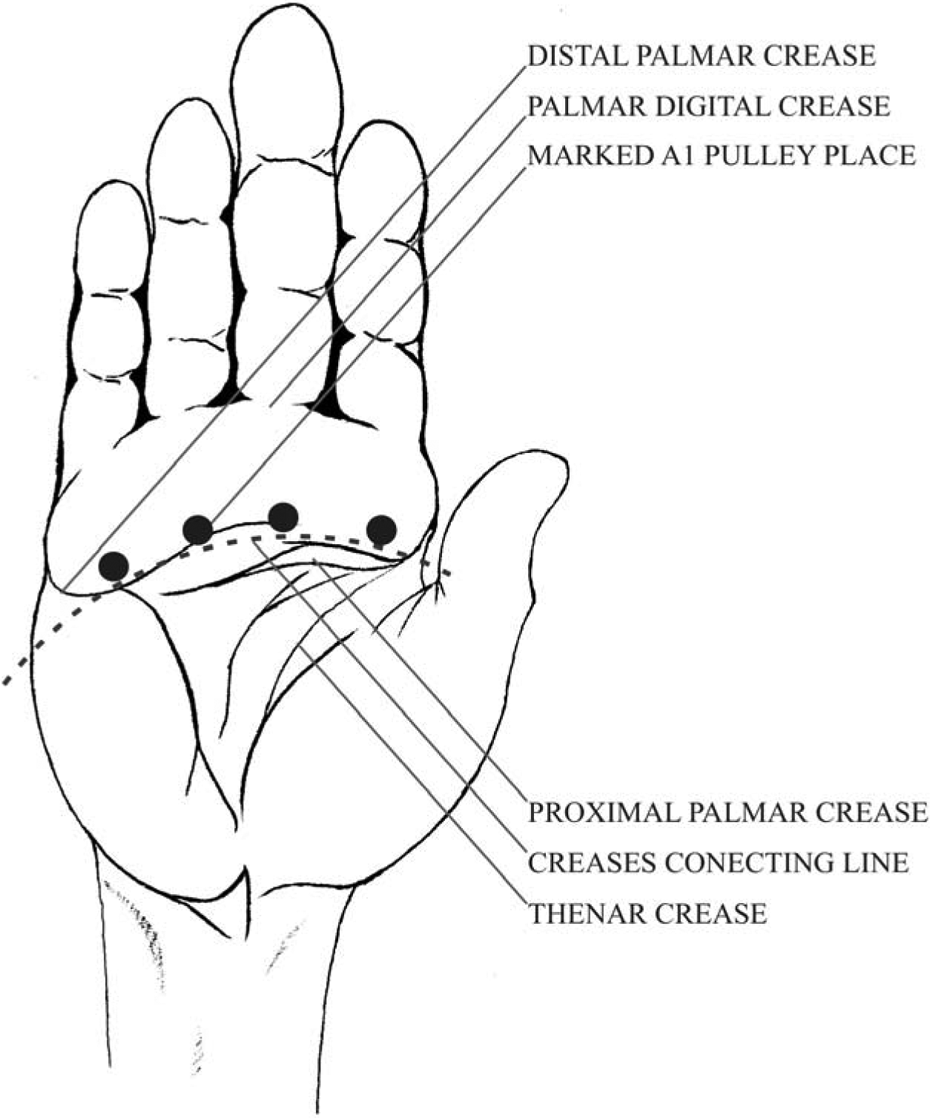
Palmar creases.
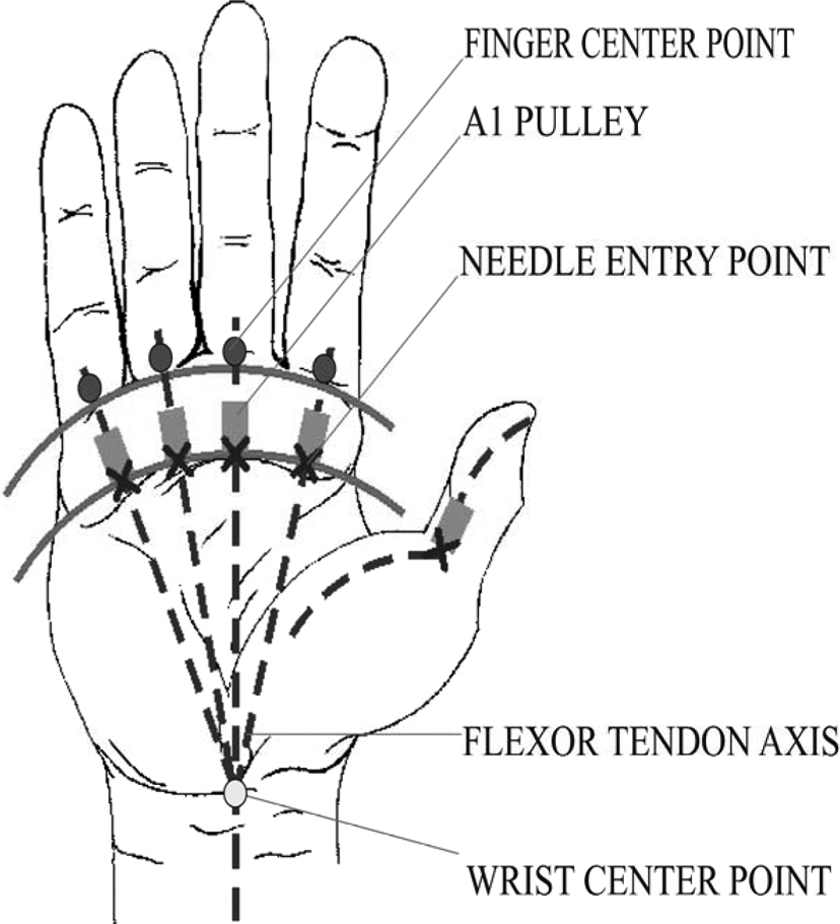
Anatomical landmarks with needle entry point.

Sagittal digit view.
Thumb method
With the thumb in the hyperextension position, the midline of the thumb was marked vertically to transverse the MCP joint crease. The same palpation technique was performed to determine the correct position of the A1 pulley in relation to surface landmarks. The flexor pollicis longus tendon and the A1 pulley were marked. Also, the thumb digital nerves were marked a few millimeters near the tendon.
Percutaneous release technique
The marked proximal edge of the A1 pulley was the needle insertion point. To determine the required depth of the needle into the tendon, the needle was inserted until it began to move or rub slightly while flexing the finger. The needle was then retracted slightly prior to being manipulated proximally and distally parallel to the tendon to release the A1 pulley.
The specimens were cross-sectioned at the A1 pulley, avoiding alternations to the neurovascular anatomy. All specimens were examined for any tendon or neurovascular injuries and completeness of the A1 pulley release. The length of the released A1 pulleys and the needle tract distance to neurovascular bundles was measured using a digital electronic micrometer ruler.
Results
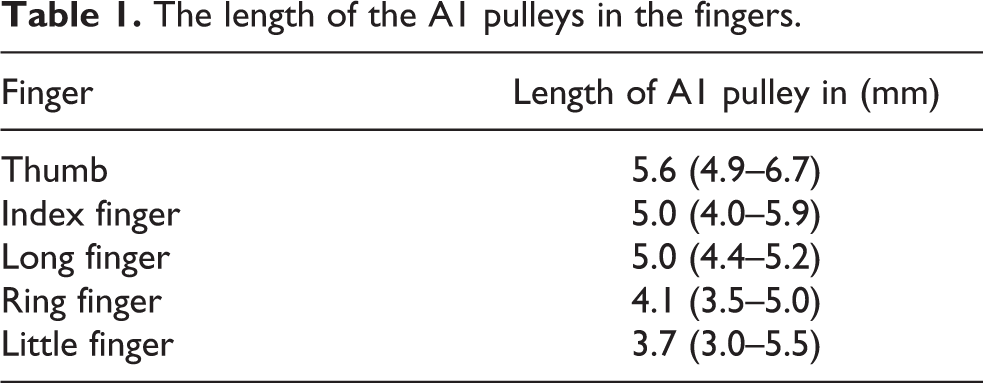
Fourteen palms were examined:14 thumbs and 56 fingers. Using palm landmarks and palpation technique in all digits, including thumbs, the location of the A1 pulley was identified. Total release of the A1 pulley occurred in 60 of 70 digits (85.7%). In four long fingers, two ring fingers, one little finger, and three thumbs, there was a partial release of the A1 pulley. The length of the A1 pulley in thumbs was 5.7 mm (standard deviation (SD) = 0.6) and in other fingers 4.5 mm (SD = 0.8; see Table 1). There were statistically significant differences in the A1 pulley lengths when comparing the thumbs to the others fingers (p = 0.005, analysis of variance (ANOVA)).
The length of the A1 pulleys in the fingers.
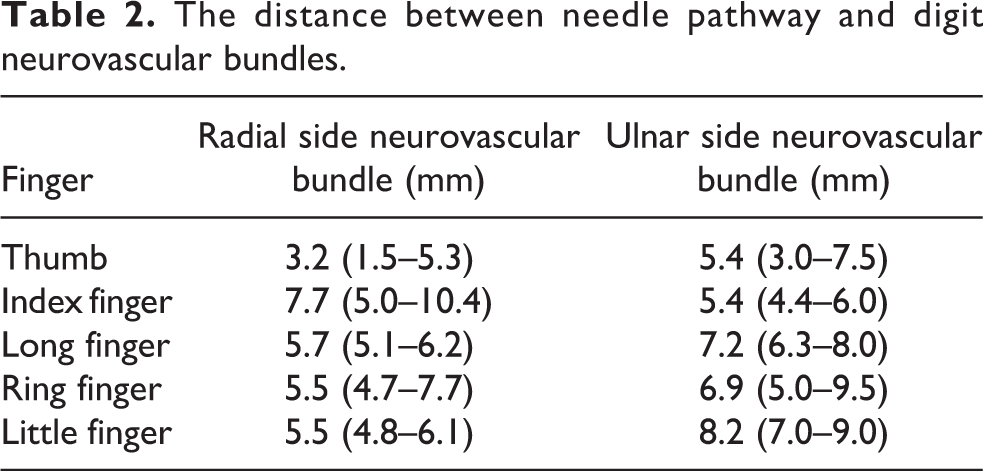
There were no signs of neurovascular bundle injuries in any digits following the procedure. The distance between needle pathway and digit neurovascular bundles was 4.3 mm (SD 1.8) in the thumbs and 6.5 mm (SD 1.4) in the fingers (see Table 2). There were statistically significant differences between the distances of the needle pathway and the digit neurovascular bundle in the thumbs compared to the other fingers (p = 0.001, ANOVA).
The distance between needle pathway and digit neurovascular bundles.
In 26 of the 70 digits (37.1%), there were superficial longitudinal injuries of the flexor tendons and 10 (14.3%) deep injuries along the tendon fibers. In 6 of the 14 thumbs (42.8%), there were longitudinal superficial injuries along the tendon fibers but no oblique flexor tendon injuries. There were no total flexor tendon injuries.
Discussion
In the past few years, percutaneous release of trigger finger became an alternative method of treatment. Lack of direct visualization of anatomical structures discouraged the wide use of percutaneous release technique. But knowing the anatomy of the pulley system and anatomical palm landmarks makes this method safe and effective. 7 All studies investigating different release techniques had the same aim—to make percutaneous release method less complicating and more effective. 8,9 Majority of studies have comparable results, but the best technique remains unknown. The advantage of this study is that combining the palpation technique with surface anatomical palm landmarks provides enhanced reliability to safely locate the A1 pulley, thereby reducing the probability of complications of neurovascular bundle injuries.
Recently published studies show promising results using different materials: special knifes, scalpels, needles, and ultrasound guide. 4,5,8 –10 Eastwood et al. successfully achieved percutaneous release in 33 of 35 fingers (94%) with a 21-gauge hypodermic needle. 11 Hoang et al. reported a success rate of 74% on cadavers with restored perfusion using an 18-gauge needle. 12 There are studies by Gilberts et al. who announce a success rate of 100% with an angiocath needle. 13 Ha and Park used a special blade with a hook to percutaneously release the A1 pulley with a success rate from 91% up to 93%. 9 Also, there are discouraging studies using needles: Dunn and Pess and Smith et al. reported comparative studies (needle vs. knife technique) showing the results were significantly better in knife technique (88% up to 98% vs. 32% up to 38%). 14,15 In this study, 19-gauge needles were used because the majority of outpatient clinics are equipped with this kind of needles and the 19-gauge needle has enough resistance to deformation forces while proceeding with percutaneous release.
The most common complications were deep and superficial flexor tendon injuries and partial release of the A1 pulley. The main reason for the complications was the learning curve. Initially, it was particularly difficult to locate the A1 pulley using the palpation technique and to precisely mark the surface landmarks on the fresh frozen cadaveric hands due to the decreased turgor of soft tissue and the absence of thickened pulleys. Knowledge of the average length of the A1 pulleys in various fingers aids in determining the correct location needed to perform complete percutaneous release. In a hand with “trigger finger,” adequate percutaneous release of the A1 pulley can be confirmed through active motion of the finger. If triggering remains, percutaneous release can be repeated. Further investigation is required as there were no cadaveric hands with trigger fingers available during this study. Flexor tendon injury is common in percutaneous release using the needle technique, 6,12,16,17 but Pope and Wolfe claimed it is not a sufficient complication. 18 To reduce the risk of flexor tendon injury, it is necessary to locate the needle tip superficially to the tendon, as described in this study. This is accomplished by flexing the finger. If there is no paradoxical movement of the needle, it is safe to push the needle parallel to the A1 pulley, but not deep down. In concern about thumb nerve injury, 7,16 –18 we preciously used marked guidelines, the needle was inserted at the midline point of the flexor tendon, and approximation to the radial side was avoided. 17,19,20 In this study, no digital nerves were injured.
The limitations of this study were as follows: cadaveric hands have no thickened pulleys and decreased turgor of soft tissue, so percutaneous release with a 19-gauge needle may be more demanding in the clinical practice.
Conclusions
The location of the A1 pulley can be predicted with success, using palmer anatomical landmarks combined with palpation technique. Percutaneous release of A1 pulley with a 19-gauge needle shows acceptable results in both safety and efficacy. Further investigation is warranted to determine whether this technique may be used in outpatient clinics with a simply equipped procedure room.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.