
Abstract
Background:
Combining osteotomies and soft tissue procedures is believed to reduce sesamoids in their anatomical position and maintain long-term correction when treating hallux valgus deformity. This study determines if a radiologic association exists between a radiolucent sign and a full percutaneous adductor tendon release (PATR), including a cadaveric study and a consecutive case series. Another aim was to determine the intra- and interobserver reliability of these observations.
Methods:
A prospective observational study was made between 2018 and 2019. First, a PATR was done on cadaveric specimens and, after the procedures, dissected to correlate what was seen fluoroscopically. The clinical group included 39 feet that presented mild-to-moderate HV deformity and were treated with percutaneous osteotomies associated with PATR.
Results:
Observers 1 and 2 saw a radioscopic radiolucent sign in 100% of cadavers and the patient population. They also observed a triangle-shaped image with an incidence of 75%, which we have named the “triangle sign.”
Conclusion:
The triangle sign may be helpful in the intraoperative confirmation of PATR and latero-plantar capsule release using this percutaneous technique.
Level of Evidence:
Level II, development of diagnostic criteria.
Introduction
Combining osteotomies and soft tissue procedures is believed to biomechanically reduce sesamoids in their anatomical position—under the first metatarsal head—and maintain long-term correction when treating hallux valgus (HV) deformity.1,21,38 Several studies have failed to describe which soft tissue structures were released. Additionally, which structures must be detached remains unclear.5,10,26,36 These data, among other reasons, may explain the persistent high overall recurrence rate of HV deformity (2.7% to 73%).2,4,9,31,33
According to some authors, adductor tendon release (ATR) indications are irreducible metatarsophalangeal (MTP) joints 23 and mild to severe HV deformities.1,8,21,22,25,34,35,37,38 Some authors prefer an isolated adductor tendon release,3,7,18,28 and others add a partial lateral capsulotomy.6,24,29 The percutaneous ATR (PATR) recently provided powerful and quantifiable correction of hallux valgus deformity, as shown in a biomechanical study. 12 However, the question of how and when remains partially unanswered, mainly because of the lack of comparative studies and confusion in the terminology used.
In addition to these problems regarding the indication of lateral release and objectification of the released structure, confirming whether a lateral release has been successfully performed is challenging because of the location of the targeted structures. It is even more complicated in percutaneous (minimally invasive) surgery, with no direct exposure to the anatomical structures. Surgeons would benefit from a direct or indirect sign that can predict which structures are being released, which has not been reported. The study hypothesized that there would be a direct relationship between a PATR12,14,15 and a radiolucent image in most of the cases included in a cadaveric and clinical study. Another aim was to determine the intra- and interobserver reliability of these observations.
Material and Methods
A prospective observational study was made between June 2018 and April 2019, divided into 2 stages. First, the purpose was to perform a PATR on cadaveric specimens and, after the procedures, dissect them to correlate what was seen fluoroscopically. A total of 11 specimens with HV deformity were included. The cadavers were selected from a study that mainly addressed the risk of nerve and tendon lesions 12 and the correcting power after the PATR technique. 14 In this study, the adductor tendon was released (mainly the oblique portion) in 100%; thus, a correlation of the radiologic sign can be made accurately. The lateral collateral ligament was released in 36.4%. The second stage of the study included a group of 39 feet that presented mild to moderate HV deformity and were treated with percutaneous osteotomies16,17 associated with PATR. 12 The adductor tendon was released in both studies, so these results were used to continue with radioscopic observation. The principal author performed all the PATR procedures and used the same technique.
The outcome measurements were collected as follows: a radiolucent sign was searched on radiographic images on both groups (cadaveric and clinical group). Two independent observers (foot and ankle surgeons with 3 and 7 years’ experience, both fellowship-trained) visualized each image twice (separated for at least 1 week). The observers were trained to recognize whether or not an image was radiolucent. The radiolucent images obtained were defined as “triangle sign” or “other shape” (eg, round, rectangular).
The cadaveric images were assessed using a XiScan 4400 model 6″ 450 fluoroscopy unit for extremities. The device uses a maximum power of 70 kV. The image captured by the display unit was black and white, with a 1:1 ratio size and a resolution of 1296 × 966.
A Philips BV Endura device with an image intensifier of 9″ was used to evaluate the postoperative data from patients. This uses a fixed anode tube with active heat management and a nominal power of 3.15 kW: 110 kV (max), 30 mA. The image captured by the display unit was black-and-white, with a 1:1 ratio size and 2 megabytes of digital information.
Description of Technique (Cadaveric and Clinical study)
The patient was seated with the foot hanging over the table’s edge. Using a surgical scalpel blade (SM64 Swann-Morton), a 3-mm first-web portal was made at the level of the first MTP joint, which was localized using fluoroscopy (Figure 1). The blade was advanced with a coronal orientation of 60 degrees until a quarter of the blade (not more) was inside the joint (Figure 2). Then, the blade was rotated outward 90 degrees to face the adductor tendon, which was then cut with a frontal movement. At the same time, the first toe was driven into varus (Figure 3). A click sound can be heard as confirmation of soft tissue release. The procedure should produce the adductor tendon’s complete detachment and the lateral plantar capsule release, confirmed by fluoroscopy with dynamic views in forced varus (Figure 4). In the cadaveric study, an anatomic dissection was made to assess which structure was released.

(A) A 3-mm first-web portal was made at the level of the first metatarsophalangeal joint, (B) which was localized using fluoroscopy.
(A-C) The blade was advanced with a coronal orientation of 65 degrees until a quarter of the blade (not more) was inside the joint.

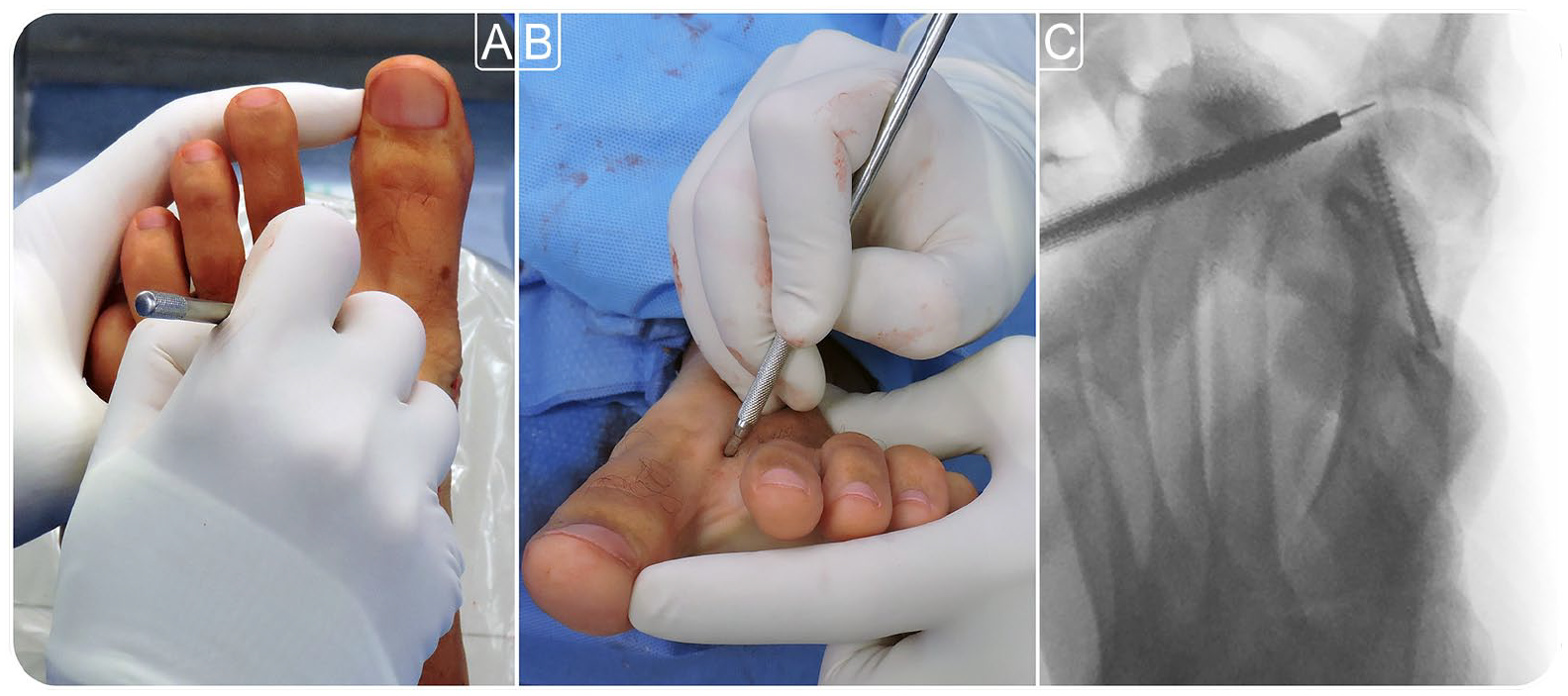
The blade was rotated outward 90 degrees to face the adductor tendon, which was then cut with a frontal movement, while the first toe was driven into varus. (A) Clinical dorsoplantar view. (B) Anteroposterior radiographic image. (C) Clinical frontal view.

Radiologic confirmation of the lateral release with dynamic views in forced varus. (A) Triangle sign. (B) Nontriangular radioscopic radiolucent image.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics, version 20.0 (IBM, Armonk, USA). The interobserver reliability of the observations was determined. The interobserver agreement was assessed by the method of total count (77.7%). Each measurement was collected in a digital file and sent for analysis. The Spearman correlation and McNemar tests (significance of changes) were used to compare results between observers. A Fisher exact independence test was applied to compare the visualizations of observers 1 and 2. A P value of less than .05 was considered to be statistically significant.
Results
Observers 1 and 2 saw a radioscopic radiolucent sign (Figure 4) in 100% of cadavers and the patient population. The triangle sign was seen by observer 1 on an average of 78%, ranging from 76 (observation 1) to 80% (observation 2) (Figure 4A). The other radiolucent images were identified as “other shape.” The triangle sign was seen by observer 2 on an average of 72% ranging from 70 (observation 1) to 74% (observation 2). The Spearman correlation test between observations 1 and 2 was statistically significant for the first observer (P < .001) and slightly significant for the second observer (P = .05179). This indicates no substantial difference between what each observer saw the first and second time. The McNemar test for the change’s significance was insignificant in both cases (P = .72 and .48).
The Fisher test for comparing the average of observations for both observers was not significant (P = .06656), reinforcing the lack of differences between observers 1 and 2.
Based on the results of the cadaveric study, the triangle sign was confirmed after the full release of the adductor tendon and the lateroplantar capsule (Figure 5).

(A) Dissection of metatarsophalangeal joint showing the adductor tendon (1). (B) Adductor tenotomy has been performed and the first toe is driven into varus, showing the triangle formed by the tendon release (2), which translates radiographically into the triangle sign.
Discussion
The most important finding of the present study is that a radiolucent sign (mainly a triangle sign) was seen in all cases when performing a PATR. Based on the results obtained and the previous cadaveric studies published,12,14 if the surgical technique is done as described, and a radiolucent image is observed, we can ensure that surgeons release the adductor tendon completely.
Recently, PATR was shown to be a reproducible and safe technique, as the adductor tendon was completely released in every foot in a cadaveric study. In addition, no neurovascular lesions were observed. 12 This procedure also produced a powerful valgus correction in the MTP joint. However, no changes were found in the correction of sesamoid subluxation, first metatarsal, and proximal phalanx pronation after PATR on cadaveric specimens. 14 Using the information provided by published studies, PATR needed indirect tools to be a more reliable procedure, more than anything, because it is a percutaneous and soft tissue procedure. The radiolucent sign helps to achieve this objective.
Intraoperative radiographic signs have proved helpful and showed excellent interobserver reliability and validity.11,20,30 This study found a radiolucent sign, which we named the “triangle sign,” associated with the intraoperative confirmation of percutaneous adductor tendon release and lateroplantar capsule. Given the prevalence observed, surgeons should repeat the procedure if no radiolucent sign is observed.
According to some authors, the indication for ATR is irreducible MTP joints 23 and mild to moderate HV1,4,8,14,15,21,22,25,37,38 and severe deformities.32,34,35 Kim et al 23 described a selective lateral soft tissue release based on passively correcting the HV after a distal chevron osteotomy. This technique produced safe and stable corrections. Seo et al 35 showed that less than 20 degrees of varus shift when doing a stress test was optimal for performing adductor tendon and metatarsosesamoid capsular release. In a recent meta-analysis, Yammine and Assi 38 concluded that there might be a beneficial effect of lateral soft tissue release (including the lateral capsule of the first metatarsophalangeal joint, the sesamoid suspensory ligament or lateral sesamoid metatarsal ligament, and the transverse metatarsal ligament) in all cases of HV deformity, and a probable efficacy of an added adductor hallucis tendon release when the deformity is moderate to severe. PATR has proven helpful in correcting mild to moderate deformities associated with a percutaneous, intraarticular chevron osteotomy. 17 According to the literature, no objective maneuver or sign was published to help adductor tendon release when treating hallux valgus deformities.
There is still some debate about when an ATR must be performed (before or after the bony correction procedure). According to some authors, this procedure can be made before4,8,13,23,24,35 or after the osteotomies.3,19,25 Those who prefer to do it pre-osteotomy indicate this procedure if passive correction of the HV deformity is possible (between 0 and 20 MTP varus position).4,5,23,35 Surgeons that advocate ATR post-osteotomy indicate a lateral release if there is residual incongruence19,26 or the sesamoids are not relocated. 27 In contrast, others perform the technique in all patients regardless of the MTP congruency. The authors of this study prefer to do PATR post-osteotomy to stabilize the first metatarsal head when shifting laterally. 17 There were no statistically significant differences between what was seen by observers of both groups: in the cadaveric study, the PATR was performed without an osteotomy, and in the clinical series, post-osteotomy. This concludes that the osteotomy does not modify the outcomes, and the sign can help in both scenarios.
As the release of the lateral collateral ligament was assessed only in the cadaveric study, it is difficult to reach a definite conclusion. The section of this anatomical structure may add a stronger radiolucent image or be rectangular rather than a triangle shape. In a previous cadaveric study evaluating the PATR, 12 a lateral collateral ligament was released entirely in 4 of 11 specimens. When comparing the radiolucent images with those in which the ligament was sectioned, no specific shape was associated with either group. Further studies may help assess the need for lateral collateral ligament release or the treatment of hallux valgus and its possible symptomatic metatarsophalangeal instability.
There are some concerns about the design of this study. First, it may be difficult to reproduce the sign because it was found in a canned environment (a surgeon with 14-year experience in percutaneous technique who had performed more than 1000 PATRs using 2 radioscopic devices and the same instruments). Second, the authors cannot certainly confirm what they released in the patients. Finally, we recognize that using fluoroscopy to assess soft tissue structures may be unreliable in some specific environments. On the other hand, using 2 different devices may represent a benefit or a disadvantage, depending on subjective opinions. We believe it is advantageous because of the diversity of surgeons, hospitals, and devices; thus, it could be adapted to different settings.
Conclusion
A radioscopic radiolucent sign was seen in 100% (75%, triangle shape) of cadavers and the patient population. This means that these objective signs may be helpful in the perioperative confirmation of percutaneous adductor tendon release and lateroplantar capsular release.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241241269 – Supplemental material for A Radiologic Triangle Sign for Percutaneous Adductor Tendon Release (PATR): Cadaveric Study and Case Series
Supplemental material, sj-pdf-1-fao-10.1177_24730114241241269 for A Radiologic Triangle Sign for Percutaneous Adductor Tendon Release (PATR): Cadaveric Study and Case Series by Jorge Javier Del Vecchio, Eric Daniel Dealbera, Lucas Nicolás Chemes, Gastón Slullitel, Juan Pablo Calvi and Miki Dalmau-Pastor in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
The authors express their gratitude to the generosity of the body donors of the Dissection Room and Body Donors Service of the University of Barcelona.
Ethical Approval
The Bioethics Committee of our institution approved the cadaveric study (IRB number 00003099). Approval from the Institutional Review Board was obtained and in keeping with the policies for a retrospective review, informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.