
Abstract
Purpose:
The purpose of this study was to compare the results of blind versus ultrasonography-guided percutaneous A1 pulley release for treatment of trigger finger.
Methods:
This prospective study included 21 patients (25 fingers) who underwent blind release and 20 patients (23 fingers) who underwent ultrasonography-guided release. The visual analog scale (VAS) score, proximal interphalangeal joint contracture, complications, and patient satisfaction were compared between the groups.
Results:
At the final follow-up, triggering had disappeared in all patients who underwent ultrasonography-guided release, whereas three patients who underwent blind release required revision surgery for postoperative triggering. No complications were observed. VAS score was significantly different between groups at 2 and 4 weeks postoperatively. All patients who underwent ultrasonography-guided release were satisfied, whereas three patients who underwent blind release were not satisfied.
Conclusion:
Ultrasonography-guided percutaneous A1 pulley release for treatment of trigger finger reduces postoperative pain and complications, such as incomplete release, compared with a blind procedure.
Introduction
Trigger finger refers to stenosing tenosynovitis of the flexor tendon at the A1 pulley and is a common cause of finger pain, triggering, and locking. 1,2 Trigger finger is usually treated conservatively with splints, physical therapy, anti-inflammatory medication, and corticosteroid injections. If such treatment fails, open surgical release of the A1 pulley is indicated, which is successful in 83–98% of patients. 1,2 However, complications, including long recovery time, wound dehiscence, infection, stiffness, flexor tendon bowstringing, and scar tenderness, have been reported. 1,3
Blind percutaneous A1 pulley release was first introduced by Lorthior. 4 Compared to the open procedure, the advantages of this procedure include a shorter recovery time, avoidance of scar tenderness, and application in the outpatient setting. 1,4 –8 However, because the surgeon cannot visualize the surrounding structures directly, there is a potential risk of injury to the tendon and neurovascular structures, and complete release cannot be confirmed. 6,7 Conversely, ultrasonography-guided percutaneous A1 pulley release can identify the anatomical structures in real time, which can prevent injury and reduce the likelihood of incomplete release. 9 –12 Jou and Chern, in their study of ultrasonography-guided percutaneous A1 pulley release, reported satisfactory results in all 107 digits studied. 9 In another study, Nikolaou et al. 13 reported comparable results between ultrasonography-guided percutaneous release and open release.
However, few studies have compared blind and ultrasonography-guided percutaneous release techniques. Therefore, the purpose of this study was to assess the safety and efficacy of blind versus ultrasonography-guided percutaneous A1 pulley release.
Methods
Materials and methods
A total of 97 patients (108 fingers) diagnosed with trigger finger between February 2015 and December 2015 were included in this prospective randomized controlled trial.
The inclusion criteria were patients in whom no effect of conservative treatment, such as corticosteroid injection, was seen for at least 6 months. We excluded patients less than 20 years of age and those with severe osteoarthritis, rheumatoid arthritis, or combined disease, such as de Quervain disease, in the same hand. The degree of symptoms was classified into five stages according to the Quinnell classification 2 (Table 1). Patients with grades 0 and 1 were excluded.
Grading of trigger finger with Quinnell’s classification.

Randomization
Of 97 patients (108 fingers), 44 patients (47 fingers) were excluded due to an improvement in symptoms after conservative treatments. And five patients (five fingers) refused to participate in the clinical research. Two patients (three fingers) were excluded due to rheumatic arthritis. Finally, a total of 46 patients (53 fingers) were included in this study. Patients were divided into two groups by computerized randomly. Twenty-four patients (28 fingers) included in group A underwent blind percutaneous A1 pulley release, while 22 patients (25 fingers) included in group B underwent ultrasonography-guided percutaneous A1 pulley release. A total of five patients were lost in the last follow-up. So, 21 patients (25 fingers) in group A and 20 patients (23 fingers) in group B were analyzed (Figure 1).
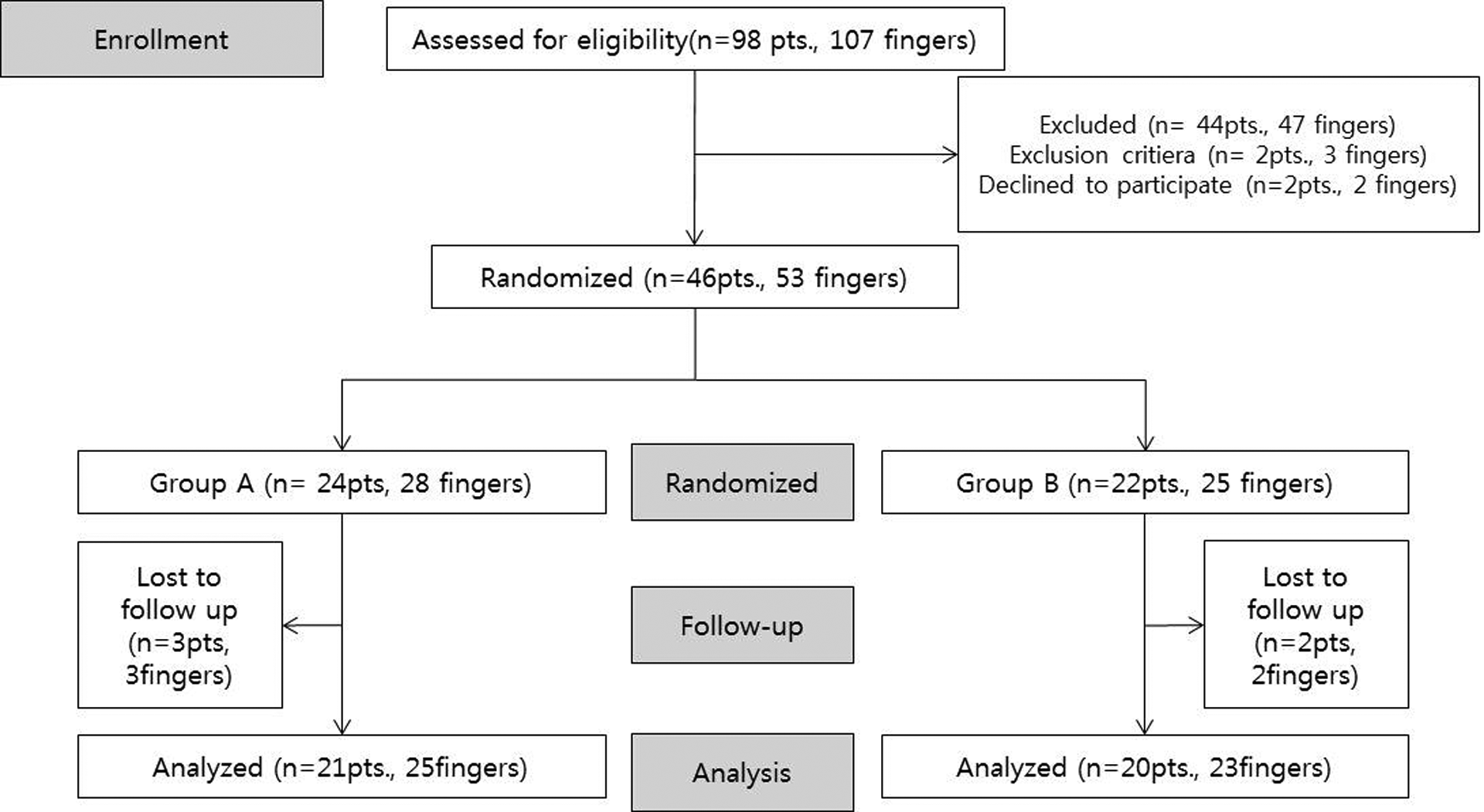
Patients’ flowchart.
Surgical methods
All surgeries were performed by an experienced surgeon.
Blind percutaneous release technique
Blind percutaneous release was performed using a HAKI knife (BK Meditech Inc., Seoul, Korea) under local anesthesia 7 (Figure 2(a)). The patient was placed in the supine position with the affected hand sterilized and draped. A total of 2 cc of lidocaine (lidocaine hydrochloride 2%; Daihan, Seoul, Korea) was injected subcutaneously in the distal portion of the A1 pulley.
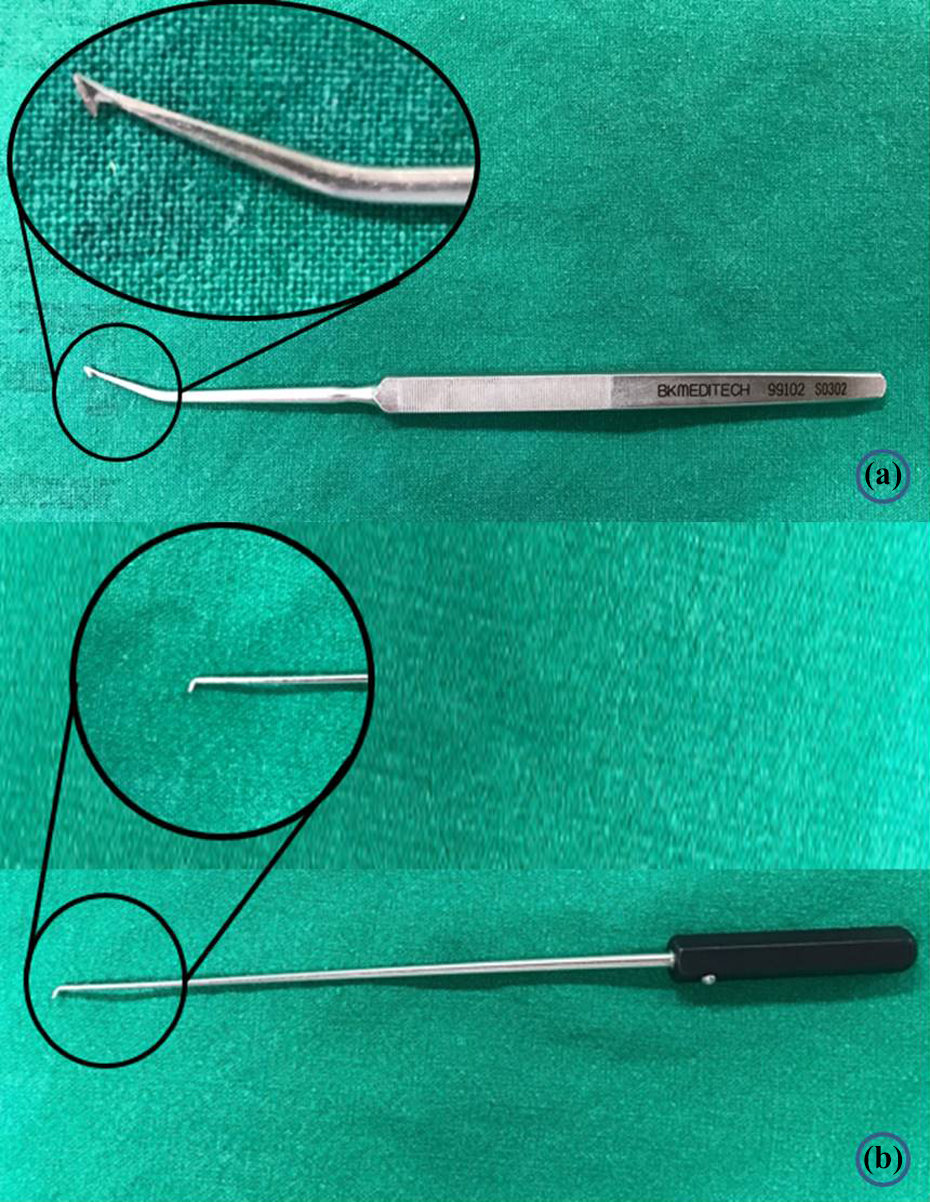
(a) Blade of HAKI knife (BK Meditech Inc.) and (b) small probe (90 mm small joint probe, 70° tip, Linvatec).
The HAKI knife was inserted 0.5 cm distal to the metacarpal crease for the thumb, between the proximal palmar crease and basal crease of the finger for the index finger, and between the distal palmar crease and basal crease of the finger for the other fingers (Figure 3). After the HAKI knife touched the fibrous pulley, it was advanced proximally along the flexor tendon. At the proximal end of the pulley, the HAKI knife was hooked onto the pulley and then pulled from proximal to distal to incise the pulley. The patient moved his/her fingers to confirm that the triggering had disappeared. To evaluate whether the A1 pulley was completely released, a small probe (90 mm, 70° tip; Linvatec, Largo, Florida, USA; Figure 2(b)) was inserted to contact the flexor tendon at the proximal end of the A1 pulley and then glided distally to check for a hooking sensation. If any suggestion of incomplete release persisted, the procedure was performed again.
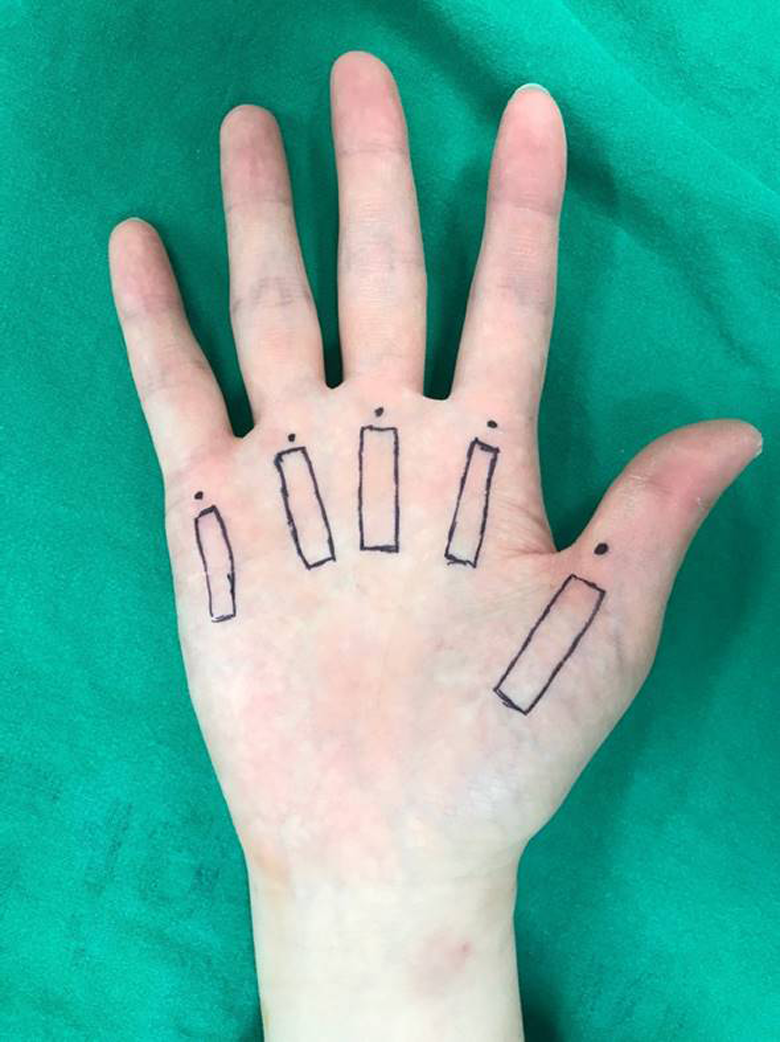
Knife insertion point (dot) and location of linear transducer placed (square).
Compressive bandaging with a short-arm splint was applied with the finger in extension. Two days after surgery, the wound was checked in the outpatient department and range of motion exercise was started. In the case of flexion contracture, a night extension splint was worn for 1–2 weeks.
Ultrasonography-guided percutaneous release technique
Ultrasonography-guided percutaneous release was performed using a linear transducer (Accuvix XG, 7–15 MHz; Samsung, Seoul, Korea) under local anesthesia. Under an axial view, the ulnar and radial digital vessels and midline of the flexor tendon were marked on the A1 pulley area (Figure 4(a) and (b)). Under a sagittal view, the proximal and distal ends of the A1 pulley were marked (Figure 4(c)).

(a) and (b) Axial sonography for marking digital artery. (c) Initial ultrasonography (sagittal view, A1 pulley). White arrow: A1 pulley; PP: proximal phalange; MC: metacarpal bone.
The linear transducer was inserted into sterilized vinyl foil, and sterilized gel was applied to the patient’s hand under local anesthesia. The HAKI knife was inserted in the same position as for blind percutaneous release. Under an axial view, the blade of the HAKI knife was placed at the center of the flexor tendon. Then, while holding the HAKI knife in place, the transducer was rotated for a sagittal view. The blade was advanced proximally to the proximal end of the A1 pulley under ultrasonographic guidance. After hooking the HAKI knife onto the proximal end of the A1 pulley, the knife was pulled from proximal to distal to incise the pulley (Figure 5).
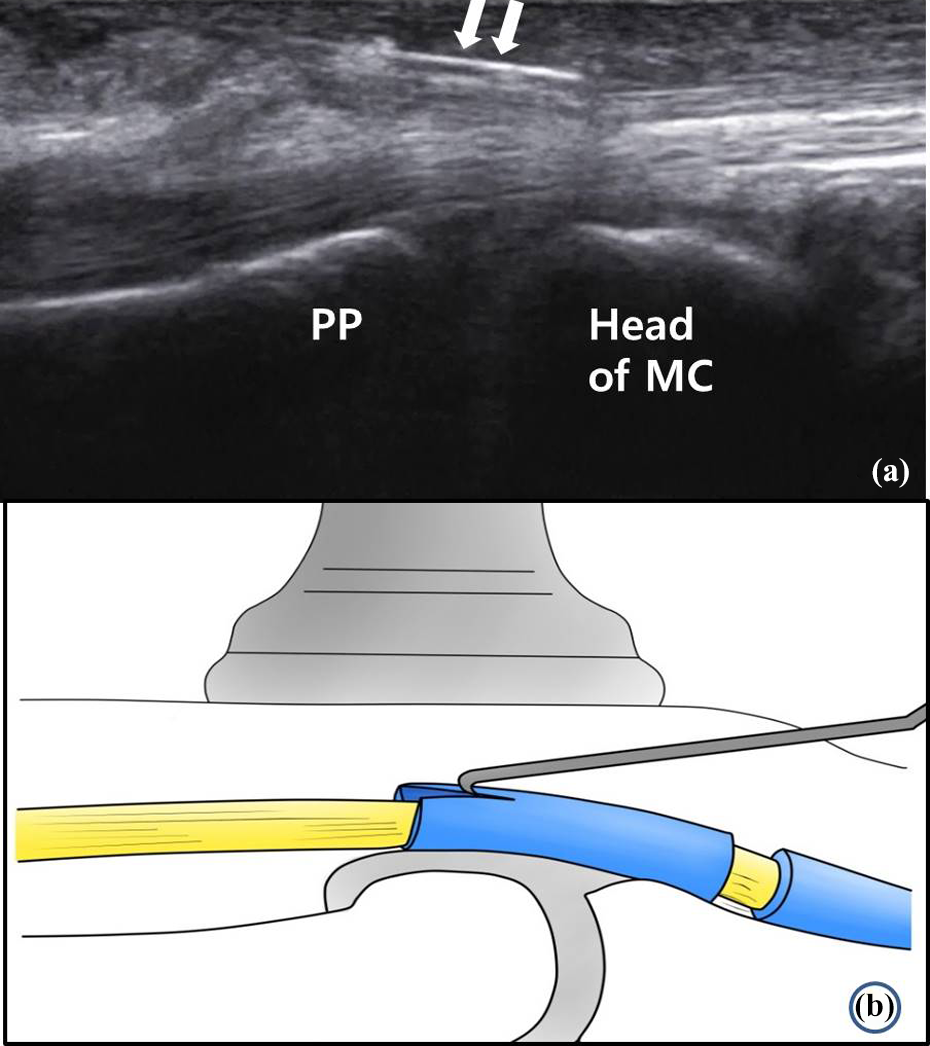
(a) HAKI knife placed in the proximal margin of A1 pulley (white arrow). (b) The diagram of this procedure. PP: proximal phalange; MC: metacarpal bone.
To evaluate whether the A1 pulley was completely released, a small probe (90 mm, 70° tip; Linvatec, Largo, Florida, USA; Figure 2(b)) was inserted to contact the flexor tendon at the proximal end of the A1 pulley and then glided distally to check for a hooking sensation (Figure 6). If there was a hooking sensation, the HAKI knife was reinserted to re-incise the A1 pulley (Figure 7).

(a) Incomplete release of A1 pulley (hollow white arrow), probe (filled white arrow) was used to check incomplete release. (b) The diagram of incomplete release of A1 pulley. PP: proximal phalange; MC: metacarpal bone.

(a) Complete release of A1 pulley. (b) The diagram of Complete release of A1 pulley. PP: proximal phalange; MC: metacarpal bone.
Disappearance of triggering was confirmed by active finger motion by the patient, and postoperative care was the same as that for blind percutaneous release.
Outcomes
To evaluate the functional and clinical results, postoperative visual analog scale (VAS) score was recorded at 2 and 6 weeks postoperatively and at the final follow-up. At the final follow-up, residual triggering and range of motion of the proximal interphalangeal joint were evaluated, and patient satisfaction was assessed according to Patel and Moradia grading 14 (Table 2). During follow-up, complications, such as tenderness around the scar, loss of sensation, and presence of infection, were recorded.
Grading the results of percutaneous release.

VAS: visual analog scale.
Statistical analysis
Differences in clinical outcome were analyzed using the Student’s t-test and Mann–Whitney U test. A p value of <0.05 was considered statistically significant. When a power analysis was performed to evaluate the power of clinical outcomes between the two groups, this study achieved a power of 0.73 for detecting differences with an actual α = 0.05. G*Power 3.0.10 was used for the power analysis.
Results
Age, sex, mean follow-up, number and involvement of digits, and grade of triggering were evaluated as demographic factors. No significant differences were found in demographic characteristics between the two groups (Table 3).
Demographics of patients.a

a No significant differences between two groups.
All patients showed significant improvement in clinical outcomes such as VAS score, postoperative proximal interphalangeal joint (PIP) contracture (p < 0.05). In addition, the ultrasonography-guided group showed significantly better VAS score at 2 and 4 weeks postoperatively compared with the blind group. However, no significant differences were found between the two groups (Table 4).
Results of blinded release versus ultrasonography-guided percutaneous release.

VAS: visual analog scale.
Triggering disappeared in all patients who underwent ultrasonography-guided release, whereas triggering continued in three patients who underwent blind release. Open A1 pulley release was performed in these three patients at 6 weeks postoperatively. In two cases, incomplete release was observed at the distal part of the A1 pulley. In the other case, the pulley was completely incised, but longitudinal tear and adhesion of the flexor tendon were observed.
In addition, in one patient who underwent ultrasonography-guided release and in two patients who underwent blind release, the VAS score was 3 points or more and tenosynovitis was found at 6 weeks postoperatively. After infection was excluded, a steroid was injected under ultrasonographic guidance. Subsequently, the symptoms improved.
All patients who underwent ultrasonography-guided release were satisfied (excellent in 17, good in 3), whereas three patients who underwent blind release were not satisfied (fair in 1, poor in 2). Other complications, such as nerve injury and wound infection, were not observed (Table 4).
Discussion
Our results showed that ultrasonography-guided percutaneous release resulted in a better success rate, a higher VAS score, and greater patient satisfaction compared with blind percutaneous release for treatment of trigger finger.
Several instruments have been used for percutaneous release, including the tenotome, 21-gauge angiocatheter, and specially designed knives. 4,6,7,15 Rajeswaran et al. 10 reported good results of ultrasonography-guided percutaneous release using a 19-gauge needle. However, Ha et al. 7 considered that injection needles can be twisted easily and that a vertical approach from above the A1 pulley may increase the risk of nerve damage. Therefore, they designed the HAKI knife with a hook shape and reported satisfactory results with complete relief of triggering. Nikolaou et al. 13 also reported a success rate of 100% using this knife in ultrasonography-guided percutaneous release. In the present study, the HAKI knife was used and operative satisfaction was 86% in blind percutaneous release, which is similar to that seen in previous studies.
However, percutaneous release has several native problems. For example, inexperience of the surgeon and anatomical variation of the patient can lead to accidental injury to the flexor tendon or adjacent neurovascular bundles, as well as difficulty in determining the completeness of release. 16,17 In addition, close proximity of the digital nerve makes percutaneous release potentially dangerous in the thumb, index finger, and little finger. Furthermore, a longitudinal tear of the flexor tendon has been reported to occur in 90% of the cases. 16,17 Ultrasonography-guided percutaneous A1 pulley release was first introduced by Jou and Chern et al. 9 to overcome the problems with blind percutaneous release. Ultrasonography is used to identify the digital nerve, artery, and vein as well as the thickened annular pulley during percutaneous release. This observation can help to reduce any risk to the neurovascular bundle and the likelihood of incomplete pulley release. In this study, there were no neurovascular injuries in the blind release group. However, our results of ultrasonography-guided release showed better VAS scores at 2 and 4 weeks postoperatively as well as higher patient satisfaction with complete resolution of triggering compared with blind release. Therefore, we cautiously supposed that the ultrasonography-guided percutaneous release technique was a more safe and reliable method for obtaining complete pulley release.
Although percutaneous A1 pulley release can eliminate stenosis induced by the A1 pulley, it can cause persistent pain after surgery because it cannot remove the tenosynovitis of the accompanying flexor tendon. Therefore, Patel and Moradia 14 reported satisfactory results with steroid injection into the tendon sheath after percutaneous release. In the present study, steroid injection into the tendon sheath in cases with pain and tenosynovitis symptoms at 6 weeks postoperatively had satisfactory results. Therefore, if there is no evidence of bacterial infection or relief of triggering after percutaneous release, steroid injection into the sheath should be considered.
Unfortunately, Paulius and Maguina 18 described injury to the flexor tendon in 17% and incomplete release in 83% of cases with ultrasonography-guided percutaneous release in a cadaveric study. They insist that, although ultrasonography may improve safety, the experience of the surgeon remains important. However, in a cadaveric study, it is difficult to identify the vessels and obtain dynamic images. This can lead to potential damage to the surrounding structures and/or incomplete release. To overcome these risks, we marked the anatomical structures using ultrasonography before percutaneous release. During surgery, the blade was always positioned in the middle of the flexor tendon to avoid stinging the tendon. After pulley release, a probe was inserted to confirm complete release. In addition, the patient confirmed disappearance of triggering during an active range of motion.
This study has several limitations. Statistical power is reduced due to the small sample size in the present study (n = 32). This could have played a role in reducing the significance of some of the statistical tests. In addition, the results of open A1 pulley release and ultrasonography-guided percutaneous release cannot be compared because this study did not include open surgical results. Furthermore, pain assessment using the VAS score is prone to subjective error. Finally, there were additional costs associated with performing ultrasonography-guided A1 pulley release (US$30).
Conclusion
Ultrasonography can identify the A1 pulley, flexor tendon, and neurovascular bundle in real time, thereby reducing the risk of injury to the surrounding structures and reducing the likelihood of incomplete release in percutaneous A1 pulley release.
Ultrasonography-guided percutaneous A1 pulley release for treatment of trigger finger reduces postoperative pain and incidence of complications, such as incomplete release, compared with a blind procedure.
However, surgical skill remains important for ultrasonography-guided percutaneous release. Therefore, the surgeon must have good knowledge of the anatomical structures, exhibit excellent handling of the ultrasound equipment, and provide complete resection of the pulley through the use of delicate surgical skills.
Footnotes
Authors’ note
This study is supported by Wonkwang University 2017.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.