
Abstract
Background:
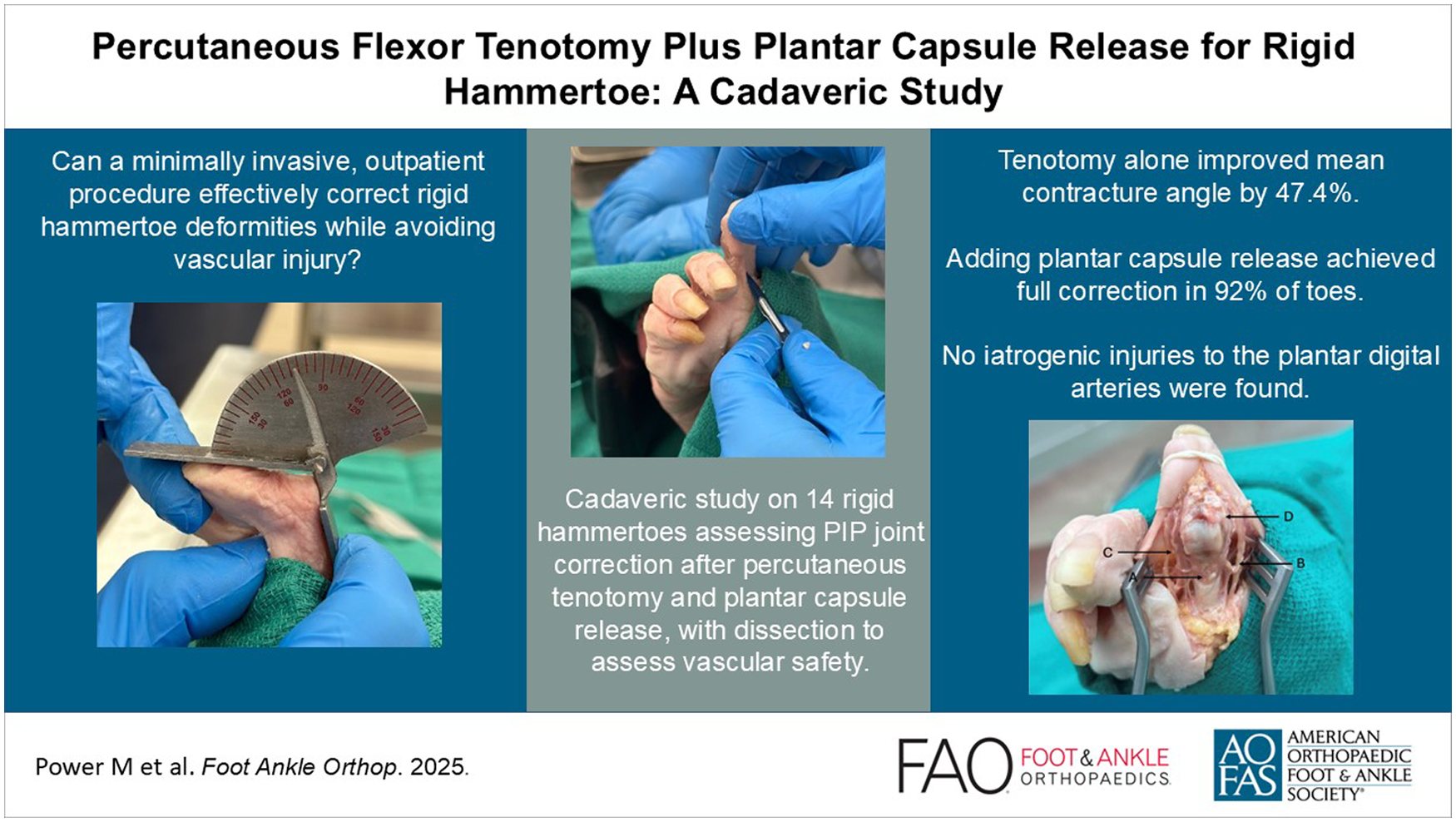
Rigid hammertoe deformities in diabetic patients present a therapeutic challenge: percutaneous tenotomy often fails to address capsular contractures, whereas arthrodesis carries an elevated risk of complications. We hypothesized that combining tenotomy with plantar capsule release would provide effective correction while preserving neurovascular structures. This study evaluates the feasibility correction magnitude and vascular safety of this technique through a cadaveric model.
Methods:
We perfused 10 clinical-grade lower-limb cadaveric specimens, possessing 14 rigid hammertoes (N = 14), with an India ink–latex mixture to highlight vascular structures. Specimens with significant pathology or prior forefoot surgeries were excluded. The angle of the hammertoe deformity was measured using a goniometer preoperatively, after percutaneous flexor tenotomy, and again after releasing the plantar capsule. Standard dissection was then conducted to assess the common plantar digital arteries.
Results:
Mean preoperative contracture of 56.5 (range 15-86) degrees improved to 26.8 (range 0-60) degrees (47.4%) after tenotomy of the flexor digitorum brevis and longus tendons, with 1 toe releasing fully. In cases where full release was not achieved following tenotomy, plantar capsule release was performed. Full release was obtained in 92% of the cases undergoing plantar capsule release. Importantly, no iatrogenic injury occurred to the plantar medial and lateral digital arteries during the procedure.
Conclusion:
In cadaveric specimens, partial release of the rigid hammertoe deformity was seen following flexor tenotomy in all but 1 toe. The addition of a proximal interphalangeal joint plantar capsule release was effective at obtaining full release, without evidence of vascular injury. As such, combining tenotomy with plantar capsule release showed effective correction in this cadaveric model and may represent a less invasive option for correcting rigid hammertoes in an outpatient setting.
Level of Evidence:
Level V, expert opinion includes case reports and technique tips.
Clinical Relevance:
This technique may offer diabetic patients a lower-risk alternative to arthrodesis, potentially reducing ulcer-related amputations through earlier intervention in outpatient settings.
Keywords
Introduction
Foot ulcers disproportionately impact people with diabetes with a 19% to 34% lifetime incidence and 20% risk of progressing to amputation. 1 Toe deformities, particularly hammertoes, are a significant risk factor for ulceration, infection, and amputation. Ulceration is often due to abnormal pressure distribution on the dorsum of the proximal interphalangeal (PIP) joint and toe tip. 2 Although the exact etiology of hammertoes remains debated, intrinsic foot muscle atrophy and flexor-extensor imbalances—due to diabetes-associated motor neuropathy—are generally thought to cause the characteristic metatarsophalangeal joint hyperextension and PIP flexion.1,3
Current management strategies exist on a therapeutic spectrum. Conservative measures against ulcers include patient education, frequent foot examination, regular callus debridement, appropriately fitted footwear, and early detection and treatment of diabetic foot ulcers. 1 However, conservative measures often prove insufficient for established deformities, and ulcers can persist and reoccur, which can lead to osteomyelitis.
Surgical management depends on distinguishing flexible from rigid hammertoes. Flexible deformities are less severe and can be passively corrected by the examiner. 1 For these cases, percutaneous flexor tenotomy has emerged as an effective outpatient option. Studies have shown that tenotomy alone achieves ulcer healing rates of 92% to 100%, expedited healing times, and reduced progression of pre-ulcerative lesions to active ulcers.4 -6 Other minimally invasive techniques, such as selective long or short flexor tenotomy, PIP joint arthrolysis, and phalangeal osteotomies, also exist. 7 However, rigid deformities, characterized by fixed PIP contractures from capsular fibrosis, typically require arthrodesis or resection arthroplasty. These procedures carry significantly higher complication rates in diabetic patients compared with nondiabetic populations, including infections and poor wound healing. 8 A recent technique tip proposed the idea of combining percutaneous flexor tenotomy and plantar capsule release for rigid hammertoes, highlighting growing clinical interest in this minimally invasive approach. 9 However, as a descriptive report, it lacks quantitative data on the degree of correction and anatomical validation of its safety.
This therapeutic gap motivated our investigation into a minimally invasive alternative for rigid hammertoes. Building on the success of percutaneous tenotomy for flexible deformities, we hypothesized that adding a PIP joint plantar capsule release would provide effective correction for rigid hammertoe deformities without compromising neurovascular integrity. Our cadaveric study assessed this novel technique’s feasibility, effectiveness, and risk to adjacent neurovascular structures. Ultimately, we aimed to develop a minimally invasive outpatient procedure that improves rigid hammertoe alignment while avoiding implant-related risks—potentially improving access, shortening wait times, and reducing costs compared with traditional surgical interventions.
Methods
Specimen Selection and Preparation
Ten lower-leg specimens, spanning from mid-tibia to tip of the toes, were used. Selection criteria included a clinically evident rigid hammertoe deformity. Specimens with significant pathology or prior forefoot surgeries were excluded. All cadaveric feet were Caucasian and female with a mean age of 87 (range 72-99) years (Table 1). Fourteen rigid hammertoes were identified (N = 14) through passive reduction maneuvers, 6 from left feet and 8 from right feet. Ten of the toes were second digits, whereas 4 were third digits.
Baseline Characteristics of Cadaver Specimens and Rigid Hammertoes.

The clinical-grade cadavers were prepared with the Sandeski technique and stored at 4 °C. The anterior and posterior tibial arteries of each specimen were cannulated and perfused with an India ink–latex mixture. 10 This perfusion technique was employed to highlight the vascular branches supplying the phalanges, facilitating the identification and assessment of vascular structures during the procedure. This study was approved by the Horizon Health Network Research Ethics Board (RS: 2024-3386).
Operative Technique and Measurements
All procedures were performed by a fellowship-trained orthopaedic foot and ankle surgeon with extensive experience in minimally invasive techniques. The sample consisted of 14 rigid hammertoes of 10 different cadaveric specimens (n = 14). The cadaveric feet were positioned to simulate a supine patient with the foot at the end of the examination table. The angle of the hammertoe deformity (degrees) at the PIP joint was measured using a goniometer: (1) at baseline, (2) after percutaneous flexor tenotomy, and (3) after releasing the plantar capsule (Figure 1).

Preoperative lateral view of a cadaveric rigid hammertoe demonstrating a 74 degrees proximal interphalangeal joint flexion contracture, measured by goniometer.
A No. 11 blade was used for the percutaneous flexor tenotomy, following a technique adapted from Tamir et al. 5 A transverse incision (2-3 mm) was made on the plantar surface of the toe at the base of the middle phalanx, using a midline approach to avoid injury to the plantar medial and lateral digital arteries (Figure 2).

Landmarking for initial percutaneous flexor tenotomy in a cadaveric rigid hammertoe, showing midline approach at the base of the middle phalanx with 90 degrees blade angulation relative to the middle phalanx.
While applying a passive extension force to the toe, the flexor digitorum longus (FDL) and brevis (FDB) tendons were cut. Passive reduction of the toe was carried out and the post-percutaneous flexor tenotomy angle was measured. Release is indicated by further extension of the toe relative to its baseline: complete (release), being an angle of 0 degrees, and partial (release), of more than 0 degrees indicating remaining rigidity. In cases where passive reduction of the toe revealed that a full release was not achieved, plantar capsule release was carried out by advancing the No. 11 blade into the PIP joint capsule at an angle perpendicular to the middle phalanx, allowing entry into the joint. The entry into the joint can be detected through tactile feedback. If entry into the joint is not immediately achieved, the blade is used to palpate the proximal portion of the middle phalanx until it enters the PIP joint. The plantar capsule was fully released by angling the blade medially and laterally, while always maintaining contact with the bone. Successful release was confirmed by improved toe extension relative to baseline (Figure 3).

Measurement with goniometer of the cadaveric hammertoe post tenotomy and plantar capsule release, measuring 0 degrees, restoring full range of motion.
Following the procedure, anatomical dissection was performed to expose the FDL and FDB tendons, the joint capsule, and to visually assess the continuity of the medial and lateral proper plantar digital arteries and nerves for any iatrogenic damage (Figure 4).

Anatomic dissection through a plantar approach to assess the release of the flexor digitorum longus and brevis tendons (A), assess the integrity of the medial (B) and lateral (C) proper plantar digital arteries and nerves, and the release of the plantar capsule (D) post-procedure.
Statistical Analysis
Descriptive statistics were used to analyze the data. Continuous variables were reported as means and SDs, whereas categorical variables were reported as percentages or counts. This descriptive cadaveric study (N = 14) focused on reporting the angle of entry, success rates of plantar capsule release, and incidence of neurovascular damage. Analyses were performed using SPSS Statistics (v29.0.1.1 (244)).
Results
We evaluated the effectiveness of a combined tenotomy and plantar capsule release in 10 cadaveric specimens (mean age, 87 years; range, 72-99) with 14 rigid hammertoes (N = 14; Table 1). Pre-treatment PIP joint flexion angle averaged 56.5 (range 15-86) degrees (Table 2). The selected hammertoes were unable to be manually straightened, reflecting the rigidity of the deformity. Tenotomy alone achieved a mean 47.4% improvement in PIP contracture (mean, pre-tenotomy 56.5 vs post-tenotomy 26.8 degrees; range post-tenotomy, 0-60 degrees), with complete correction (0 degrees) in 1 toe (7%; Table 2). In cases where full release was not achieved (n = 13), subsequent PIP plantar capsule release was successful in completely releasing the plantar capsule in all cases, and it restored full mobility in 92% of them (Tables 2 and 3).
Hammertoe Correction Outcomes by Specimen. a
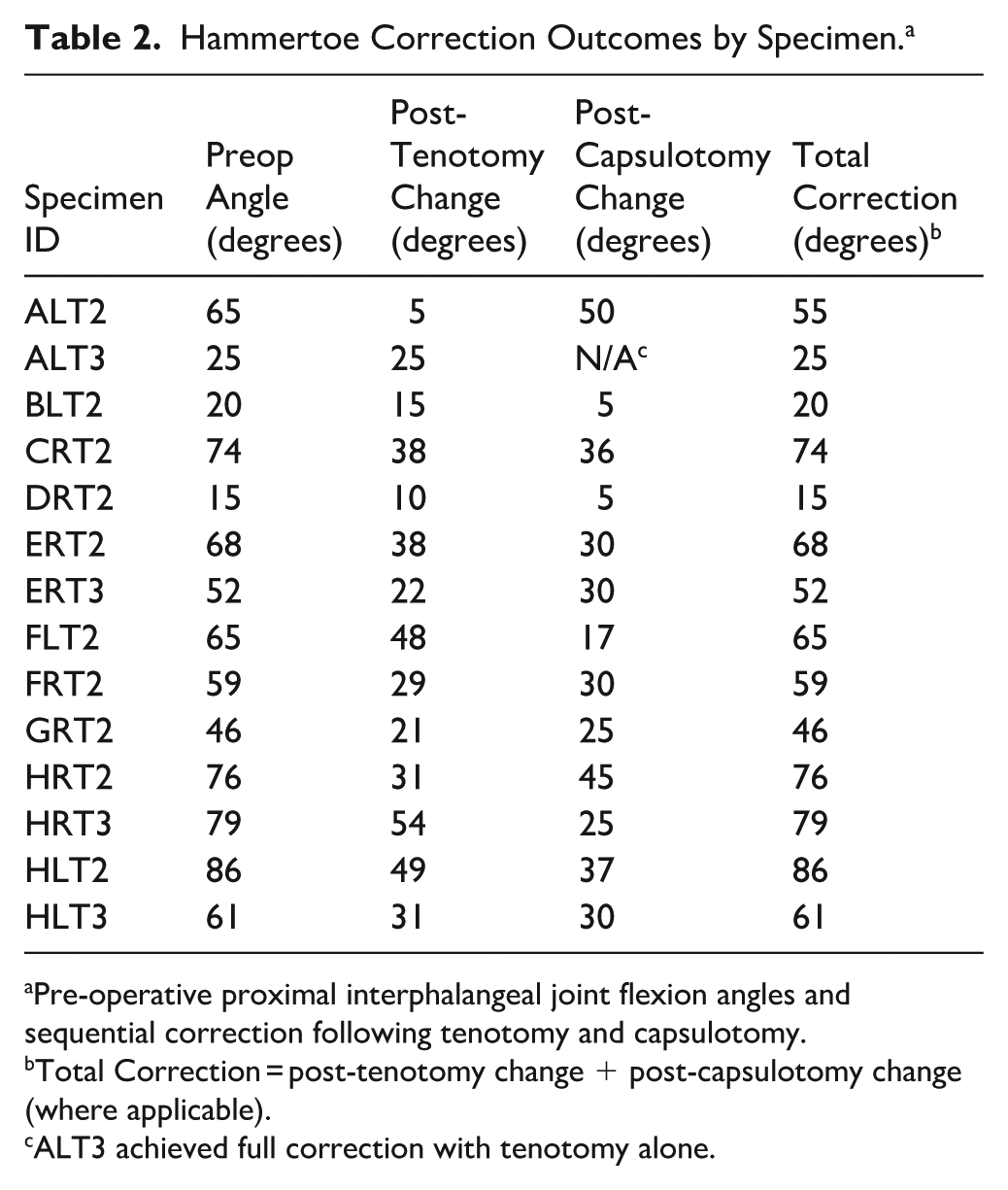
Pre-operative proximal interphalangeal joint flexion angles and sequential correction following tenotomy and capsulotomy.
Total Correction = post-tenotomy change + post-capsulotomy change (where applicable).
ALT3 achieved full correction with tenotomy alone.
Tendon Release Status and Neurovascular Safety Outcomes by Specimen. a

Abbreviations: FDB, flexor digitorum brevis; FDL, flexor digitorum longus; N, no; Y, yes.
Confirmation of FDL and FDB tendon releases and integrity of plantar medial and lateral digital arteries and nerves post-procedure. All specimens maintained intact plantar digital arteries post-procedure.
Anatomical dissection confirmed complete release of both FDL and FDB tendons in all but 1 toe (DRT2, brevis intact with complete restoration of movement; Table 3). Importantly, no iatrogenic damage was observed to the medial or lateral proper plantar digital arteries and nerves in any of the specimens, supporting procedural safety, while achieving complete release of the flexion deformity at the PIP joint (Table 3).
Discussion
Percutaneous flexor tenotomy achieves excellent outcomes for flexible hammertoe deformities, with ulcer healing rates of 92% to 100%,4 -6,11 -13 but fails to address the capsular contractures underlying rigid deformities. 1 For these cases, current options (ie, arthrodesis or resection arthroplasty) carry increased risks in diabetic patients (5%-20% non-union; 2%-5% infection).8,14,15 Given this population’s elevated risk of surgical complications, we developed a combined tenotomy-capsulotomy technique designed to address both tendinous and capsular contractures. Our findings in this cadaveric study demonstrate that this minimally invasive approach reliably corrects rigid hammertoe deformities without compromising adjacent neurovascular structures.
The technique described herein builds on the combined percutaneous flexor tenotomy with plantar capsule release, as recently described by Power et al, 9 by quantitatively validating the degree of correction and anatomical safety, offering a potential advantage over traditional open procedures. 5 Tenotomy alone improved contractures by 47%, whereas subsequent PIP joint plantar capsule release achieved full correction in 92% of toes, reinforcing the pivotal role of PIP joint capsular fibrosis in rigid deformities. 1 The single outlier was a rigid hammertoe that did not correct despite tenotomy and plantar PIP joint capsule release. One possibility for this may be worn or deformed PIP joint articular surfaces that, despite soft tissue release, maintain a rigid flexed position. This was not verified in the present investigation but may be evaluated by anatomical dissection following the procedure in future clinical studies.
FDL tenotomy proved essential in all specimens, consistent with its dominant role in PIP and DIP flexion. 16 Interestingly, in 1 case (DRT2), preserved FDB function did not compromise outcomes. This successful correction despite FDB preservation highlights the critical role of capsule release in addressing fibrotic plantar capsules—overcoming a key limitation of FDL tenotomy alone. Importantly, employing a plantar midline entry at the base of the middle phalanx enables consistent access to the plantar capsule while keeping nearby neurovascular anatomy intact, highlighting the importance of a plantar midline approach. For patients with rigid toe deformities and especially those with comorbid diabetes, this technique offers 3 key advantages: (1) elimination of implant-related complications,14,15 (2) outpatient feasibility reducing costs and wait times,5,17 and (3) minimized risk of wound complications with a smaller incision.
Our technique aligns with a paradigm shift toward curative offloading in management of diabetic foot ulceration. This is evidenced by the Keller gap arthroplasty, which reduces hallux ulcer recurrence via joint resection, 18 and by percutaneous partial bone excision (PPBE), which effectively salvages toes with established osteomyelitis. 19 Minimally invasive interventions, such Achilles tendon lengthening and distal metatarsal osteotomies, have an important role in the reduction and redistribution of forefoot pressure, leading to resolution of impending or existing forefoot ulceration.20,21 With the minimally invasive technique outlined in the present study, by correcting the rigid deformity without bone resection or implants, we aim to intervene earlier in the disease cascade, potentially preventing the ulcers that necessitate more invasive, salvage procedures.
Study limitations include small sample size (N = 14); although this aligns with other cadaveric studies, this may reduce the clinical applicability of our findings. The specimens’ advanced mean age (87 years), exclusive female sex, and Caucasian ethnicity limit generalizability and introduces potential selection bias. 22 Furthermore, the absence of neurovascular injury in our cadaveric model does not preclude wound healing complications in living patients with diabetes and microangiopathy. Additionally, the cadaveric model presents inherent limitations; tissue properties differ from those in living patients, which could bias the tendon release and subsequent measurements. The static conditions also precluded assessment of gait dynamics, and the cadaveric model could not evaluate recurrence rates. In clinical practice, concomitant MTP/DIP deformities may contribute to malalignment and could require adjunctive procedures (eg, extensor tenotomy), which were outside the scope of this PIP-focused model. Future studies should validate functional outcomes and ulcer prevention efficacy in diverse populations.
Conclusion
This cadaveric study demonstrates that combined percutaneous tenotomy and plantar capsule release reliably corrects mild to moderately rigid hammertoe deformities while preserving neurovascular structures. The technique addresses a key limitation of current options—offering a more effective correction than tenotomy alone while avoiding the risks of more invasive techniques. Its outpatient feasibility and minimal tissue disruption make it particularly suitable for high-risk patients. Although these anatomical results are promising, clinical studies are needed to confirm functional outcomes, ulcer prevention and resolution benefit, and recurrence rates. If validated, this approach could provide a practical middle-ground option in the management of rigid hammertoes.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251398766 – Supplemental material for Percutaneous Flexor Tenotomy Plus Plantar Capsule Release for Rigid Hammertoe: A Cadaveric Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114251398766 for Percutaneous Flexor Tenotomy Plus Plantar Capsule Release for Rigid Hammertoe: A Cadaveric Study by Madeline Power, Erin Bigney, William Mayer, Hirbod Abootalebi, Siyum Mohiuddin, Hannah Isaac, Oreoluwa Alugo and Jacob Matz in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
We would like to express our gratitude to the donors and the Dalhousie Body Donation Program for their invaluable contributions to this project. We are deeply thankful to the generous donors of the Saint John Regional Hospital Foundation, whose support funded the resources essential to this study. Finally, we are appreciative of the volunteers at the Canada East Spine Centre for their hard work.
ORCID iDs
Ethical Considerations
Ethical approval was received from the Horizon Health Network Research Ethics Board under RS No. 2024-3386.
Consent to Participate
Individuals in the Human Body Donation Program at Dalhousie University provide premortem informed consent and dedicate their bodies to medical education and research. The Body Donation office retains the informed consent signed by the donor/next of kin, or legal executor.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Saint John Regional Hospital Foundation and Dalhousie Medicine New Brunswick through the 2025 Dalhousie Medicine NB Research Health Award.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
Sharing of the full study data through secure channels may be requested by email correspondence (
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.