
Abstract
Mobile-bearing Oxford medial unicompartmental knee arthroplasty (UKA) has been widely used and has produced good results in the treatment of medial compartmental osteoarthritis. But it is associated with the potential risk of meniscal bearing dislocation. Symptoms caused by most meniscal bearing dislocations include acute pain, knee swelling, and locking. We report two unusual cases of meniscal bearing spinning of 180° without remarkable symptoms, which would have been easily missed if we had not watched carefully. Therefore, if there is sudden locking, pain, swelling, or a slight locking history, the possibility of meniscal bearing spin out as well as meniscal bearing dislocation should be considered and the direction of meniscal bearing markers should be confirmed, especially on lateral radiographs.
Introduction
Mobile-bearing Oxford medial unicompartmental knee arthroplasty (UKA) has been widely used and has produced good results for medial compartmental osteoarthritis. 1,2 It has the advantage of minimizing bone resection, low potential for polyethylene wear, and preserving more normal knee functions by using an unconstrained fully congruent mobile bearing. 3 –5 But it has the potential risk of dislocation of meniscal bearing. 6 –9 Symptoms caused by most meniscal bearing dislocations include acute pain, knee swelling, locking, and radiographs which can confirm the anterior, posterior, or lateral dislocation of the bearing. 10 –13 However, in rare cases, it has been reported that radiologic diagnosis was delayed and confirmed late if symptoms were mild even though the liner had dislocated. 14,15
Here, we report unusual two cases of meniscal bearing spinning of 180° without remarkable symptoms in a mobile-bearing UKA on periodic follow-up examination.
Case 1
A 60-year-old woman with right knee medial compartment osteoarthritis underwent medial UKA (Zimmer Biomet, Bridgend, UK) at our hospital in November 2013. The intraoperative and postoperative periods were uneventful. She had a 7 mm meniscal bearing inserted in the correct direction at the time of surgery. Postoperative radiographs showed well-aligned femoral and tibial component with well-positioned meniscal bearing (Figure 1). The patient was followed up during periodic routine visits. At 3-year follow-up, her condition was good with normal gait and she was free from pain. But, she said that she had intermittent mild knee swelling and discomfort. Clinical examination of the knee showed mild medial laxity, tenseness over the medial joint line, and the range of movement was 0–140°. Radiographs were performed and an anteroposterior radiograph demonstrated no sign of component loosening, osteolysis, or degenerative changes in the other compartments, but a lateral radiograph demonstrated that the position of anterior marker wire and posterior ball marker of the meniscal bearing was reversed, which suggested a 180° spin of the meniscal bearing (Figure 2). We questioned the patient closely and she said that she had experienced sudden locking symptoms 6 months previously, and after massage of the knee by hand, the locking symptoms disappeared. Surgical assessment was performed immediately. Intraoperatively, femoral and tibial components appeared well fixed and positioned with no loosening. The meniscal bearing was easily removed and replaced by a thicker bearing (8 mm) for more secure stability (Figure 3). Postoperatively she made a good recovery and 1-year postoperatively had no further trouble.
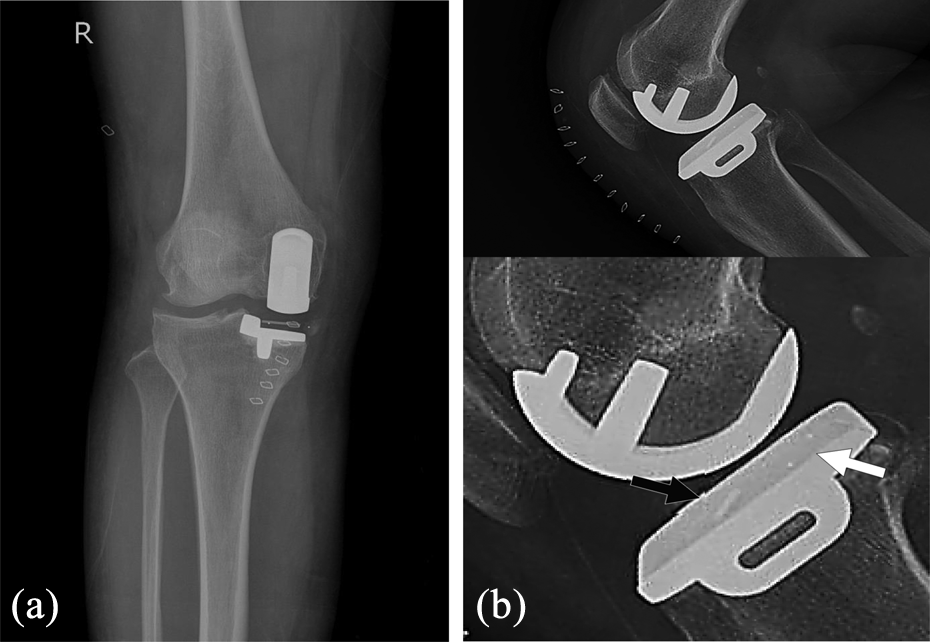
Case 1. (a) Postoperative anteroposterior radiographs showing well-aligned femoral and tibial components with well-positioned meniscal bearing. (b) Lateral radiographs. The black arrow indicates the anterior maker wire and the white arrow indicates the posterior ball marker.

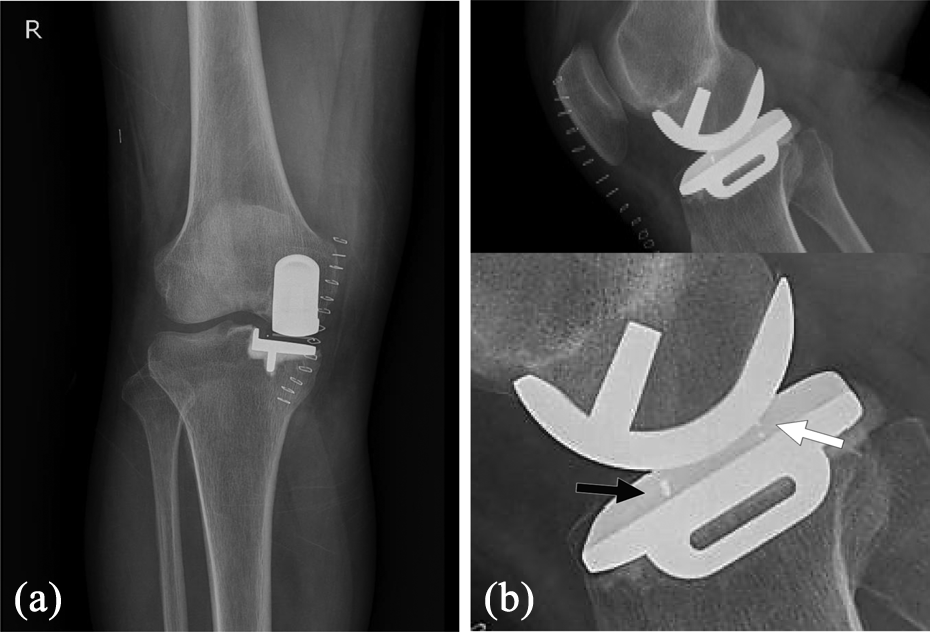
Case 1. (a) Anteroposterior radiographs showing well-aligned femoral and tibial components compared to previous radiograph. (b) Lateral radiographs showing that the position of anterior marker wire and posterior ball marker of the meniscal bearing was reversed, which suggested a 180° spin of the meniscal bearing.

Case 1. Plain radiographs taken after exchanging the meniscal bearing with a thicker (8 mm) bearing. Anteroposterior radiograph showing increased valgus alignment due to thicker meniscal bearing.
Case 2
A 67-year-old woman underwent UKA (Zimmer Biomet, Bridgend, UK) due to medial compartment osteonecrosis of her right knee at our hospital in September 2012.
The intraoperative and postoperative periods were uneventful. Her condition was checked in the clinic periodically. She had a 3-mm meniscal bearing inserted in the correct direction at the time of surgery. Postoperative radiographs showed well-aligned femoral and tibial component with well-positioned meniscal bearing (Figure 4). Five years after the surgery, the patient experienced abrupt right knee locking and pain and after massage of the knee by hand, the locking symptoms disappeared. Postoperative intermittent knee snapping disappeared too. Six months after that event, she sought radiologic examination. Radiographs were performed and the AP radiograph demonstrated no specific findings, but the lateral radiograph demonstrated that the anterior marker wire position and posterior ball marker of the meniscal bearing were reversed, which suggested a 180° spin of the meniscal bearing (Figure 5). On examination, there was mild medial laxity of the right knee during varus stress. Tenderness over the medial joint line was noted during 140° terminal flexion. We promptly recommended revision surgery due to concerns regarding recurrent dislocation and possible damage to the bearing. But, the patient suspended revision surgery since there was no inconvenience in her present daily life. Her condition was checked in the clinic regularly. At 2-year follow-up, she reported only rare episodes of pain and continued to live without great discomfort.
Case 2. (a) Postoperative anteroposterior radiographs showing well-aligned femoral and tibial components with well-positioned meniscal bearing. (b) Lateral radiographs. The black arrow indicates the anterior maker wire and the white arrow indicates the posterior ball marker.
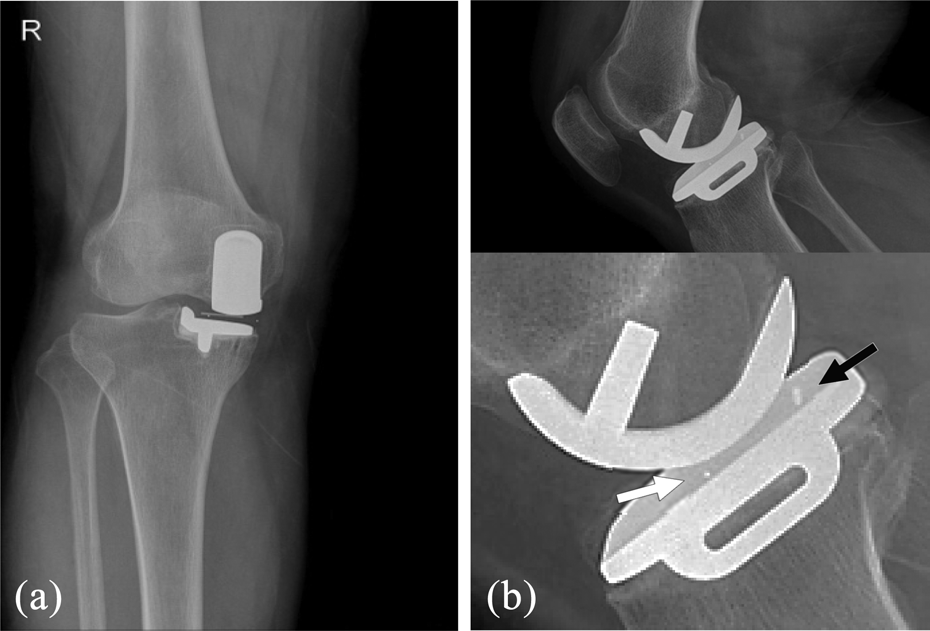
Case 2. (a) Anteroposterior radiographs showing well-aligned femoral and tibial components compared to previous radiograph. (b) Lateral radiographs showing that the position of anterior marker wire and posterior ball marker of the meniscal bearing was reversed, which suggested a 180° spin of the meniscal bearing.
Discussion
In UKA, a common complication in mobile-bearing implants compared with fixed-bearing implants is meniscal dislocation. 1,9,16 The dislocation rate is reported to range from 0.9% to 4%. 8,10,11,16 The bearing dislocation is caused by posterior impingement, ligament laxity, decreased posterior slope, and varus deformity. 6,9,17,18
Meniscal bearing dislocation has been reported in anterior, posterior, and lateral bearing locations. 10 –13 In the anterior and posterior dislocation cases, since meniscal bearing can completely dislocate from the joint space, the main clinical symptoms are sudden locking, limitation of motion, acute knee pain, and swelling. In the case of lateral dislocation, since the bearing remains in the joint space, the symptoms may be faint. 15 In rare cases, it has also been reported that anterior and posterior dislocation may have faint symptoms when the mechanical block symptom does not occur in the joint or the meniscal bearing is missed in extra-articular joint space. 12,14
Our rare case involved the meniscal bearing spinning of 180°. This is the first such report to our knowledge, except for spontaneous relocation in the reduction procedure after bearing dislocation.
In this case, there was no limitation of the patient’s range of motion (ROM) on physical examination. On AP radiograph, the meniscal bearing was well located without dislocation between the femur and tibia implant. However, on the lateral X-ray, we observed that the positions of the anterior marker wire and posterior ball marker in the meniscal bearing had changed by 180°, which could have been easily missed if we had not watched this carefully. Although it is not known exactly how the meniscal bearing spun out 180°, as a possible mechanism, after the liner spun out 90°, it may have been relocated in the opposite direction by the patient self-manipulation. As another possibility, the meniscal bearing may have first dislocated anteriorly or posteriorly and then may have been relocated in the opposite direction during the ROM process.
The morphological features of the Oxford UKA meniscal bearing are fully congruent over a complete range of motion with the round femur and flat tibial component and have a free floating nature that allows gliding on the metal of the tibia throughout the knee’s range of motion. 5,19
The bearing is slightly thicker in the anterior part than the posterior part. There is an anterior marker wire on the front of the liner and two posterior ball markers on the back to identify the anterior and posterior positions of the liner on X-ray. Although there is a difference between the anterior and posterior sides of the meniscal bearing, it is thought that the first patient did not feel any inconvenience because the basic meniscal bearing gliding was possible even if the anterior and posterior was spun out 180°.
In the second case, there was no significant pain caused by the spinning out of the asymmetric anatomical bearing, so it is under continued close observation. However, meniscal bearing change or implant revision should be considered if knee instability due to polyethylene wear or additional meniscal bearing dislocation occurs.
In summary, in mobile-bearing UKA, if there is sudden locking, pain, swelling, or a slight locking history, the possibility of meniscal bearing spin out as well as meniscal bearing dislocation should be considered. This type of meniscal bearing malposition was often overlooked, and recognition may be difficult. Therefore, careful physical examination and confirmation of dislocation of the liner on X-ray are required, and the direction of meniscal bearing markers should be confirmed especially on lateral radiograph.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.