
Abstract
Treatment of massive osteochondral defects of the medial femoral condyle is challenging. A 46-year-old man who had a medial femoral condyle fracture on his left knee underwent osteosynthesis in a hospital, but the pain remained and the patient was referred to our hospital 8 months after the surgery. Radiographs showed a varus alignment of the leg, and magnetic resonance image showed a massive necrotic area in the medial femoral condyle. The patient received high tibial osteotomy (HTO) combined with iliac cancellous bone graft and an osteochondral autograft transplantation. Pain and the knee function markedly improved 2 years after the surgery. A second look arthroscopy showed a well-covered bone graft site with cartilaginous tissue and a well-integrated osteochondral plug. HTO combined with cancellous bone autograft and osteochondral autograft transplantation could be an effective treatment for patients presenting with a varus knee deformity associated with massive osteochondral defects in the medial femoral condyle.
Introduction
Osteonecrosis of the medial femoral condyle is occasionally seen in clinical practice. Osteonecrosis can occur spontaneously and also be induced by steroids, insufficient fracture, or trauma. 1,2 In some cases, osteonecrosis extends to a large area and the collapse of the lesion results in massive osteochondral defects in the condyle. Treatment of massive osteochondral defects of the medial femoral condyle is challenging and the surgical method of treatment has not yet been established. This case report presents a rare case of severe necrotic change and osteochondral defects in the medial femoral condyle that was treated by high tibial osteotomy (HTO) combined with iliac cancellous bone chip and osteochondral autograft transplantation (OAT).
Case reports
A 46-year-old man had a motorcycle accident and sustained an injury to his left knee. He was transferred to an emergency hospital and diagnosed with an open fracture of the medial femoral condyle and osteochondral fracture (Figure 1a). He underwent osteosynthesis with a 6.5-mm cannulated screw in the hospital 3 days after the trauma (Figure 1b). Six weeks after the operation, he was permitted full weight bearing and discharged from the hospital with a crutch. He had moderate pain while walking and the pain gradually increased 8 months after the operation. Thereafter, the screw was removed and arthroscopically inspected. An MRI (magnetic resonance imaging) scan was taken after the operation, and he was diagnosed with osteonecrosis of the medial femoral condyle. As a result, he was referred to our hospital.
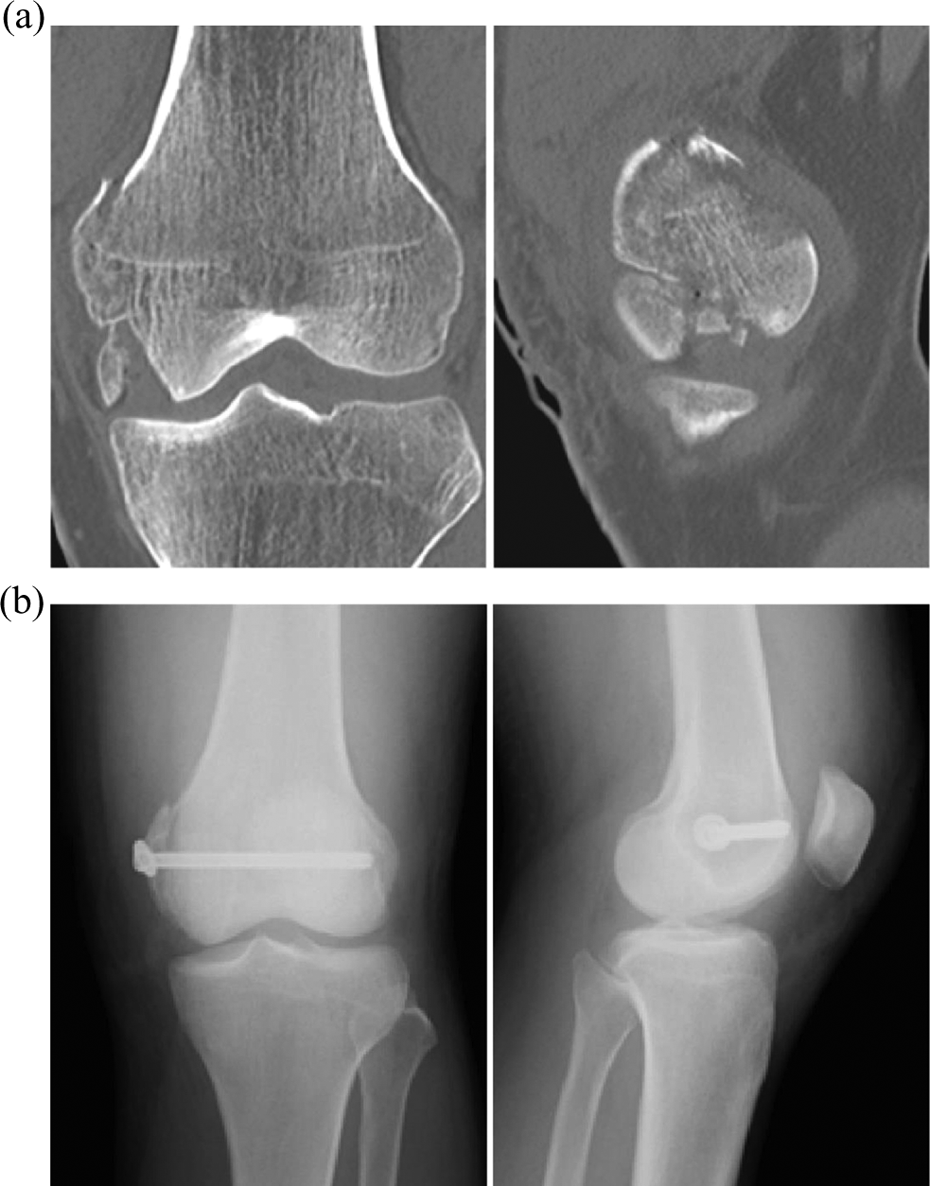
Radiographs at the emergency hospital. (a) Anteroposterior and lateral view radiographs of the knee; (b) computed tomography; (c) postoperative radiographs.
On admission, he was able to walk with a crutch. A physical examination showed an effusion in the left knee. The range of motion (ROM) in the left knee was an extension −5° to flexion 100°. He had a mild tenderness in the medial joint space. An anteroposterior view of the plain radiograph showed a narrowing of the medial joint space and a small bony shadow beside the medial femoral condyle (Figure 2a). A long leg view showed that the weight-bearing line (WBL) passed through 18% of the proximal tibia and the femoral–tibial angle was 183°, while the WBL of the contralateral uninjured side was 37% (Figure 2b). A computed tomography scan showed a destructed medial femoral condyle including the articular surface, despite the bone union that was achieved at the proximal part (Figure 2c). The MRI showed a large necrotic area in approximately one-third of the distal part of the medial condyle (Figure 3a). Thereafter, surgical treatment was performed as follows.
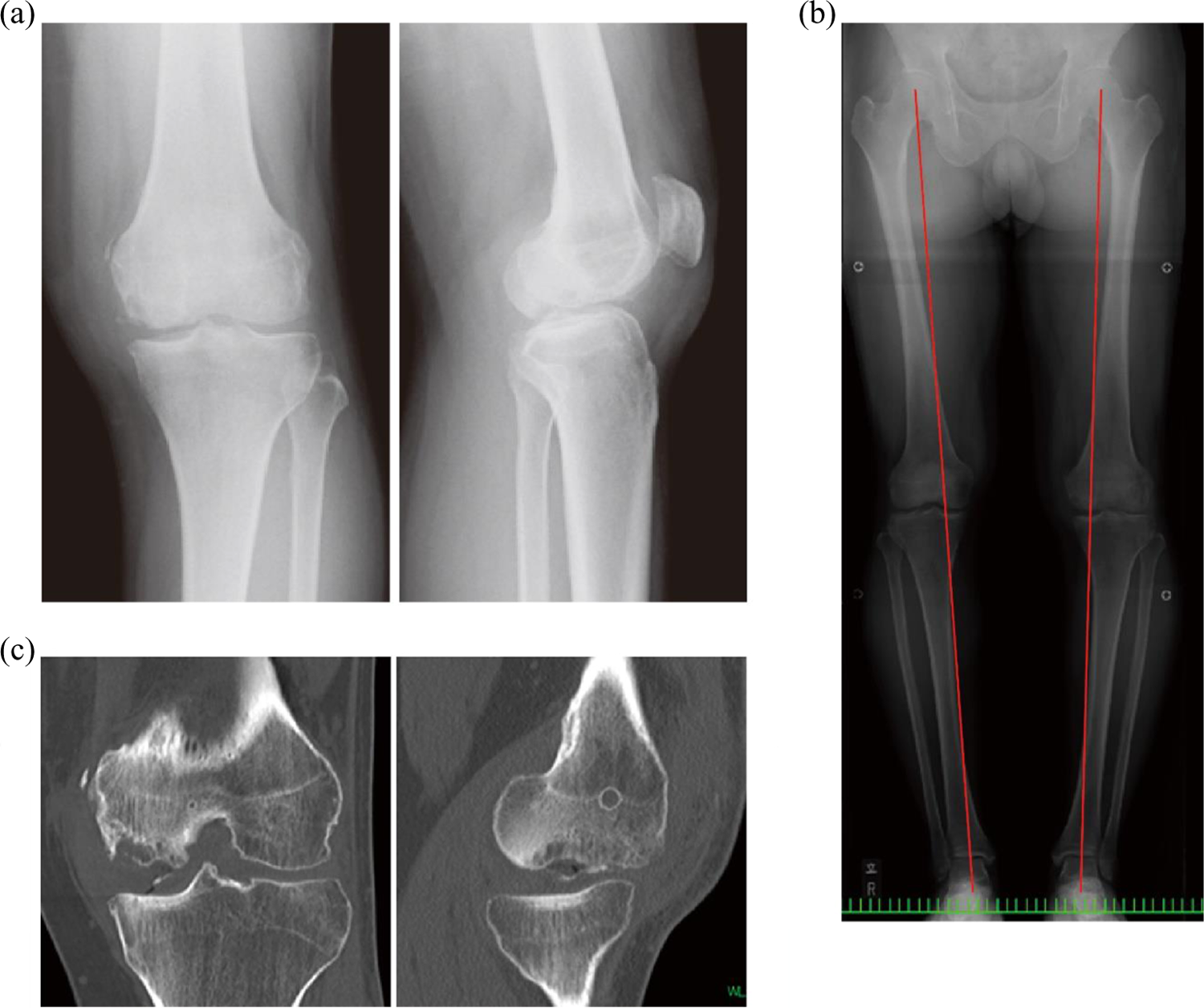
Preoperative radiographs at our hospital. (a) Anteroposterior and lateral view radiographs of the knee; (b) a long leg view radiograph. Red lines show the weight-bearing lines; (c) computed tomography.
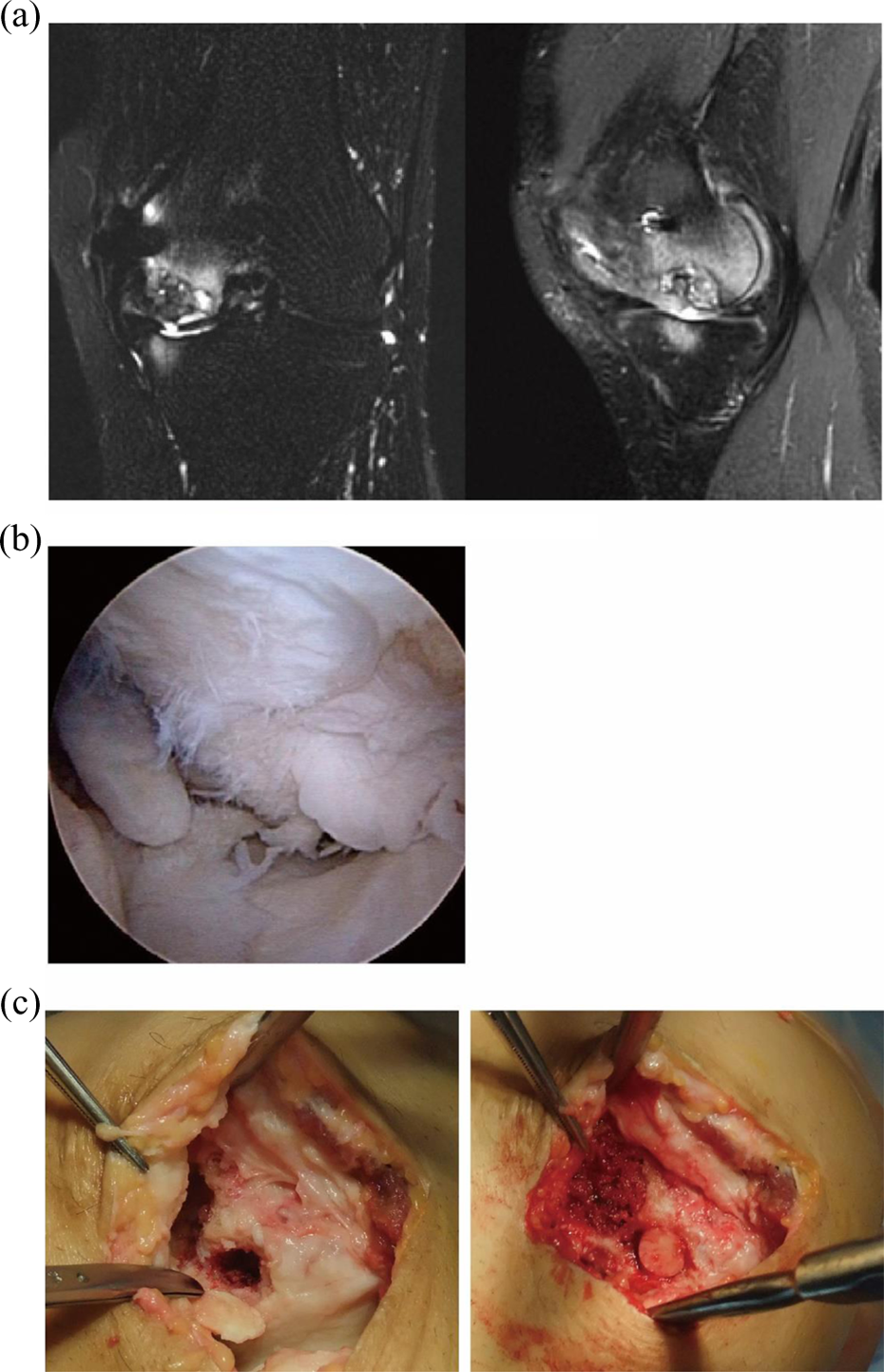
Intraoperative images. (a) An arthroscopic view of the medial compartment of the knee; (b) macroscopic view of the medial femoral condyle through the arthrotomy. After debridement of the damaged cartilage (left). After grafting iliac cancellous bone and osteochondral graft to the osteochondral defects (right).
Surgical procedure
First, arthroscopy was performed using standard medial and lateral para-patellar portal. Then, a large cartilage fragment was partially detached from the surface of the medial femoral condyle (Figure 3b) and a 25 × 15 mm bone fragment was removed. Articular cartilage of the tibia was degenerated but maintained. On examination, the anterior cruciate ligament, posterior cruciate ligament, and menisci looked normal. The patellofemoral joint was also normal.
Second, a 5-cm longitudinal skin incision connecting the medial portal was made. An arthrotomy was performed via the medial para-patellar approach. The unstable cartilage fragment was observed in the weight-bearing area at extension and the fragment was removed. Underneath the cartilage fragment, the bone was soft and necrotic. After removing the necrotic bone, a bone defect measuring 12 mm × 10 mm (diameter × depth) was observed (Figure 3c). Subsequently, a 10 mm-diameter osteochondral plug was harvested from the medial side of the patellofemoral joint (Arthrex OATS system, Naples, FL, USA) after the iliac cancellous bone chip was packed at the bottom of the defect. In the posterior part, the bone defect and necrotic bone was observed over a large area. All the necrotic bone was debrided and a bone defect measuring 30 mm in radial × 15 mm in longitudinal × 20 mm in depth was seen. Thereafter, an iliac bone graft was packed and the surface was sealed with fibrin glue (Figure 3c).
Third, a 5-cm curbed skin incision was made over the tibia. The pes anserinus was incised, and the semitendinosus and gracilis tendons were detached from the insertion site. The medial collateral ligament was detached from the bone at the osteotomy level. HTO was performed using an open-wedge osteotomy system (Arthrex, Naples, FL, USA). During the opening of the osteotomy gap, alignment was checked using a navigation system (Aesculap, Tuttlingen, Germany). An alignment correction was performed until the WBL passed through 55% of the proximal tibia. After checking the osteotomy gap, a Puddu plate with a 12.5-mm wedge was used to fix the tibia. The osteotomy gap was filled with a wedged β-tri-calcium phosphate block and cancellous iliac bone chips.
Partial weight bearing was permitted from 4 weeks postoperatively and full weight bearing was permitted 7 weeks postoperatively. The patient returned to work 4 months after the surgery. At the 2-year follow-up, a complete bone union was achieved and plate removal was performed. A postoperative long leg view radiograph of the left leg showed that the alignment was well maintained (Figure 4a), although the deformity at the most medial side of the condyle remained. At the time of the plate removal, a second look arthroscopy was also performed. Under arthroscopy, complete coverage with regenerated cartilage on the medial femoral condyle was observed, although a part of the cartilage was fibrillated (Figure 4b). In addition, a well-integrated osteochondral plug was observed with no obvious worsening of the cartilage degeneration at the tibial side and the patellofemoral joint. At the 3-year follow-up, the ROM of his left knee was from extension −5° to flexion 120°. He was able to walk and perform manual labors without limitation. Furthermore, the Lysholm score improved from 41 (preoperatively) to 95 (postoperatively).

Radiographs at the final follow-up and an image taken at the second look arthroscopy. (a) Postoperative long leg view radiograph at 2 years; (b) a second look arthroscopic view of the medial compartment of the knee.
Discussion
The most important finding of this case report is that HTO combined with autologous bone graft and osteochondral autograft transplantation could be effective for the treatment of massive osteochondral defects of the medial femoral condyle.
Medial femoral condyle fracture can be caused by high-energy injuries, such as traffic accidents and falls. Among the distal femoral condylar fractures, coronal plane fractures, which are also called as Hoffa fracture or AO-33 B3, are relatively rare and often missed or misdiagnosed by inexperienced orthopedic surgeons. 3 Since this type of fractures includes the articular surface, mistreatment can result in deterioration of the joint. In the presented case, the fracture type was not appropriately diagnosed and the articular part was not fixed stably, which appears to be the major reason for the massive necrotic change that occurred after the fracture. Bel et al. reported the outcomes of surgical treatments of 154 patients with distal femoral unicondylar fractures. According to the report, 15% of the patients had malalignment with coronal-plane or sagittal-plane deformity, and 12% of the patients had step off in the articular surface. In addition, they reported that avascular necrosis of the condyle, similar to our case, was seen in 2% of the patients. 4 Therefore, surgeons need to pay a close attention to the postoperative course after coronal fractures of the distal femoral condyle.
Treatment of massive necrosis and destruction of the femoral condyle are challenging. Unicompartmental knee arthroplasty (UKA) can be indicated for patients with severe osteonecrosis and destructed femoral condyle. Recent reports suggest that UKA can be applied to patients participating in moderate sports activities. 5,6 However, the long-term result of UKA is a concern and does not seem to be an optimal treatment, especially in young active patients. 7,8
HTO has generally been used for treating young patients with medial compartment osteoarthritis by reducing mechanical loads to the medial compartment. Good outcomes of HTO combined with drilling have been reported. 9,10 Koshino reported favorable clinical outcomes of HTO combined with a bone grafting technique that grafts cancellous bone to the osteonecrotic lesion underneath the uncollapsed articular fragment through the window opened at the side of the condyle in patients with osteonecrosis. 11 However, these techniques may not be applicable to a large necrotic area and collapsed lesion.
Some biological treatments for severe necrosis of the medial femoral condyle have been reported such as OAT and bone grafting. Kotani et al. reported good outcomes of OAT in patients with osteonecrosis of the medial femoral condyle. 12 Although OAT is a good treatment for osteochondral injury and osteochondritis dissecans, the size of the lesion may be as long as the length of a plug, which is generally 15–20 mm in size, and the diameter of the graft is 6–10 mm. Therefore, good stability of the plug may not be obtained in deeper and larger defects. The techniques using a fresh allograft to treat massive defect of the femoral condyle have been reported and can be a good treatment option. 13,14 However, such allograft may not be available in some countries like Japan.
Fukui et al. reported a successful outcome of grafting autologous iliac bone block with periosteum for treating 8–10 cm2 steroid-induced osteonecrosis of the femoral condyle based on the concept that the cells in the periosteum could regenerate the articular cartilage. 15 It appears that this surgical treatment is a good option for treating severe bone defect as long as a good stability of the iliac bone block is achieved.
To restore the articular surface underneath the bone, combined autologous chondrocyte implantation (ACI) with bone graft could be a treatment choice for large osteochondral defects. Könst et al. reported that severe osteochondral defects of the medial or lateral femoral condyle were treated with a two-step procedure that combined a gel-type ACI. 16 On the other hand, Ochs et al. reported surgical techniques of one-step ACI with cylindrical iliac bone grafting procedure with a good outcome of cartilage repair based on the MRI evaluation. Despite these surgical methods yielding good outcomes, second- or third-step operations are needed in total including the cartilage harvest for chondrocyte culture. Therefore, those procedures could be more invasive and cost demanding. Initially, we also considered ACI as a second-step surgery if the cartilage regeneration was poor. 17 However, an almost complete coverage with some cartilage over the cancellous bone-grafting site was observed at the time of second look arthroscopy and it seemed that ACI was not necessary, suggesting that bone grafting combined with HTO could be a primary choice of treatment, particularly in patients with a massive bone defect and varus deformity. The results from the previous literature and our case suggest that joint preservation can be achieved by combining the above-mentioned surgical techniques depending on the size of the defect (Figure 5).

Surgical treatment options for osteochondral defects of the medial femoral condyle with varus alignment of the leg. HTO: high tibial osteotomy; OAT: osteochondral autograft, ACI: autologous chondrocyte implantation.
There are certainly some limitations in the present case report. First, the contribution of the osteochondral plug transfer to the outcomes is not clear. It may not be necessary for HTO to be performed with bone grafting. However, we did not expect good cartilage regeneration over the bone-grafting site before surgery, as observed in this case. Therefore, we performed osteochondral plug transfer to restore the articular cartilage in at least some parts of the weight-bearing area. Second, we have not evaluated the histology of the regenerated cartilage. Therefore, the quality may not be durable for the long-term. Third, optimal leg alignment is unclear. Classically, the alignment in which the WBL passes through, 62–65% is recommended to treat patients with varus osteoarthritis. However, based on our experience, young patients whose activity level is high were not comfortable with an overcorrected valgus alignment. Therefore, we limited the correction angle to avoid overcorrection. Fourth, the follow-up period was only 3 years and a longer follow-up period is needed to further evaluate the outcome. Despite all the limitations, the present case provides useful information for the treatment of severe osteochondral defects in the medial femoral condyle.
Conclusion
In conclusion, HTO combined with cancellous bone graft and osteochondral autograft transplantation could be an effective treatment for patients with varus and severe osteochondral defects in the medial femoral condyle.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.