
Abstract
Aims:
This study aims to investigate the long-term results of vascularized iliac bone grafting (VIBG) for osteonecrosis of the femoral head (ONFH). The primary outcome is the long-term survivorship of VIBG, using conversion to total hip arthroplasty as an end-point. Secondly, this study will also analyse the patient or disease factors influencing the long-term survivorship of VIBG.
Methods:
Forty-two patients (50 hips) underwent VIBG for ONFH in our institute between September 1995 and November 2013. Only patients with a follow-up of at least 5 years were included. The risk factors, surgical complications and VIBG survivorship were recorded. The stage of ONFH was classified according to the Ficat staging of the pre-operative radiographs. VIBG was only performed to patients with ONFH of Ficat stage II and stage III. Patients with hip arthritis (Ficat stage IV) did not receive VIBG and thus excluded from the study. Long-term survivorship of VIBG is measured by conversion to total hip arthroplasty.
Results:
Twenty-eight hips (56%) had surviving VIBG for the duration of follow-up. The overall mean graft survival was 12.2 ± 7.8 years (0.4–24.0). Steroid and alcohol-induced osteonecrosis were more predominant in the graft-failure group, which had a hazard ratio of 2.33 and 2.07 respectively for graft failure (p = 0.047). In terms of complication, there was one case of groin wound infection which required surgical debridement.
Conclusion:
At a long-term follow-up of 17 years, our results showed that VIBG is effective in treating patients with pre-collapse (Ficat Stage II) and early post-collapse (Ficat stage III) in ONFH. Alcoholics and patients with steroid are at a higher risk of graft failure, so VIBG should be performed cautiously in these patients. VIBG is an intermediate operation until osteoarthritis sets in, either by the progression of ONFH or natural degenerative change.
Keywords
Introduction
Osteonecrosis of the femoral head (ONFH) is a debilitating medical condition that affects the femoral head by disrupting its blood supply. The estimated yearly prevalence of ONFH per 100,000 population ranged from 20.5 in 2002 to 37.8 in 2006, according to a nationwide epidemiologic analysis in Korea. 1 ONFH occurs earlier than primary osteoarthritis of the hip and typically affects young adults between 20 and 40 years old. 2 It is the third most common indication for total hip replacement in people under 50 years old in the United Kingdom. 3 As the disease advances, the necrotic segments of the femoral head progressively collapse leading to premature degenerative arthritis. 4 The exact pathogenesis of ONFH is unknown, but its risk factors include alcoholism, femoral neck fracture, high dose corticosteroid use and chemotherapy. 5
The treatment strategy depends on the Ficat stage of the disease. 6 Joint preservation is the goal for pre-collapse or early post-collapse lesion. In contrast, the joint replacement is indicated for patients with hip osteoarthritis or those who failed joint-preserving procedures. Vascularized bone grafting aims to provide structural support and restore vascular supply to the femoral head. The two common donor sites include ilium and fibula. 5 Pedicled vascularized iliac bone graft (VIBG) is less technically demanding since microvascular anastomosis is not required. Deep circumflex iliac artery (DCIA) had been described as a nutrient artery in VIBG but the survivorship of it was conflicting. 7 –10 To our knowledge, there is a lack of literature on the long-term outcome of DCIA pedicled iliac bone grafting in treating ONFH.
The study aims to investigate the long-term results of ONFH undergoing decompression and VIBG. The primary outcomes are the long-term survivorship of VIBG and the average time of graft survival. Secondly, we want to identify whether patient or disease factors influencing the long-term survivorship of VIBG.
Patients and method
The study was performed following the ethical standards of our institute’s Clinical Research Ethics Committee (reference number 2020.183). It was a retrospective cohort review of ONFH treated with VIBG in our institute between September 1995 and November 2013, 42 patients (50 hips) underwent VIBG for ONFH. Only patients with a follow-up of at least 5 years were included. Patient demographic was extracted from our institute’s electronic health record. The risk factors, surgical complications and VIBG survivorship were recorded. Failure of the graft was defined as conversion to total hip replacement (THR). All failure of VIBG was converted to cementless total hip arthroplasty. The stage of ONFH was classified according to the Ficat staging of the pre-operative radiographs. VIBG was only performed to patients with ONFH of Ficat stage II and stage III. Patients with hip arthritis (Ficat stage IV) did not receive VIBG and thus excluded from the study.
Surgical procedure
The pedicled iliac crest bone graft is based on the deep circumflex iliac artery (DCIA). Our institute described the surgical technique in 1996. 7 In this study, we modified the original technique to minimize the surgical dissection of the iliopsoas muscle, avoid the soft tissue impingement of the vascular pedicle and reduce the chance of post-operative hip stiffness. The modified surgical technique 11 is described below.
The patient was placed in a supine position with the donor hemipelvis raised with a sandbag under the buttock. A curvilinear skin incision was made along the iliac crest down to the femoral neurovascular bundle and extended distally to the subtrochanteric level (Figure 1(a)). The femoral artery was identified at the femoral triangle and traced proximally above the inguinal ligament, where it became the external iliac artery. After releasing the inguinal ligament, the DCIA was identified as it originated from the lateral aspect of the external iliac artery, opposite to the origin of the inferior epigastric artery.
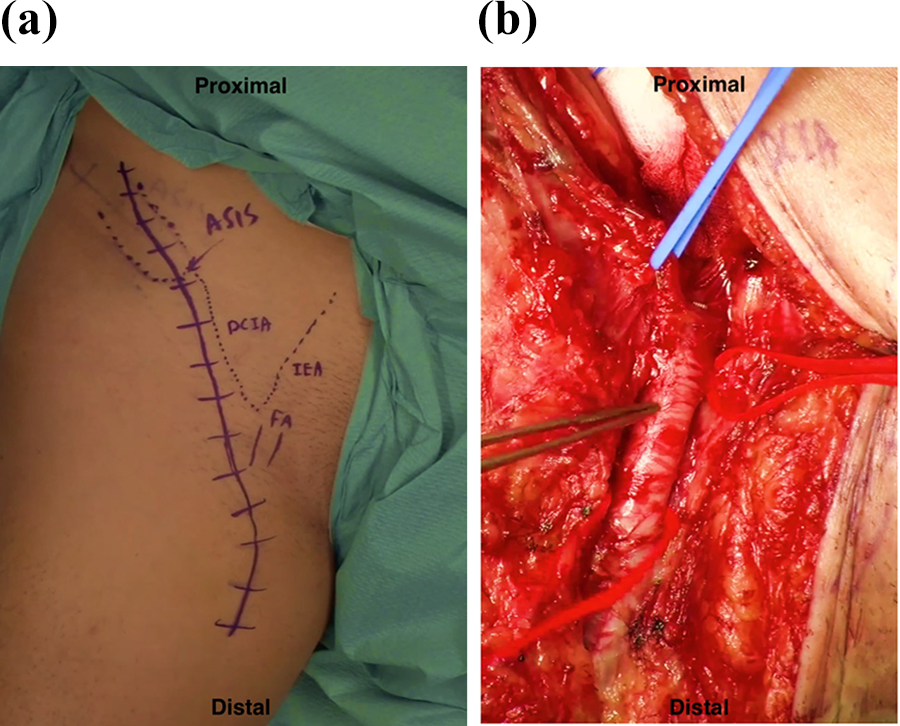
(a) Surgical incision of VIBG was marked. ASIS: anterior superior iliac spine; DCI: deep circumflex iliac artery; IEA: inferior epigastric artery; FA: femoral artery. (b) Deep circumflex iliac artery was raised with blue loop. Femoral artery and inferior epigastric artery were raised with red loop.
The DCIA pedicle was then protected with a silicone loop (Figure 1(b)). The abdominal muscles were incised to free the pedicle from any abdominal muscle attachments. Small vessel branches arising from the medial aspect of the pedicle supplying the abdominal muscle were ligated while it was mobilized and traced proximally and laterally towards the iliac crest. The lateral cutaneous nerve of the thigh was preserved and freed near the anterior superior iliac spine if it did not affect the mobilization of the pedicle. The iliacus muscle, the inner side of iliac crest bone, and its supplying pedicle were protected while the outer table of the iliac crest bone graft was freed subperiosteally.
The hip joint was approached anteriorly via the plane between the femoral artery and the femoral nerve. Ascending branches of the lateral femoral circumflex artery were ligated for better exposure of the femoral neck. The Iliopsoas tendon was released partially thereby allowing it to be elevated and retracted medially. The hip capsule anterior to the femoral neck was excised to yield good exposure of the femoral neck. A rectangular cortical bone window was made at the middle third of the anterior femoral neck after predrilling with a 2 mm drill and completing with fine osteotomes. A bone trough was created at the femoral neck and extended to the femoral head (Figure 2(a)). The necrotic bone was removed, and the bone cavity was further cleared with high-speed burr. Cancellous bone from the iliac crest was impacted into the initial necrotic part and subchondral region of the cavity of the femoral head. A tricortical iliac crest bone graft with its DICA pedicle of approximately 5 cm in length and 1 cm in-depth was harvested (Figure 2(b)). After the bone graft was trimmed to an optimal size, it was inserted and impacted into the bone trough at the femoral head and neck (Figure 2(c)). No screw fixation was needed as the bone graft was tightly fitted into the defect and remained stable. The tension of the pedicle was checked for any soft tissue impingement, especially upon hip extension. Two suction drains with suction were placed, and the wound was closed in layers.

(a) A bone trough was created at the femoral neck and head after necrotic bone was removed. (b) VIBG was harvested with its pedicle DCIA by an oscillating saw. Bleeding of the bone surface demonstrates the viability of VIBG. Cancellous bone graft was also obtained the remaining iliac crest for filling up the bone defect at the femoral head. (c) The VIBG was inserted in an orientation of the distal aspect of the bone graft pointing distally to the thigh. The bone graft was then impacted proximally into the trough while protecting the pedicle. Stability of the bone graft and the soft tissue impingement of the bone graft were checked before wound closure.
Post-operatively the operated leg of the patient was elevated with a pillow for one week to relieve the tension of the DCIA pedicle. Patients were allowed to have a free hip range of movement exercise afterwards. Moreover, they could perform touch down or partial weight-bearing walking after removal of the drains. Most patients could resume full weight-bearing walking in about 4 weeks.
Patients were followed up at 1, 3, and 6 months, every 6 months for 2 years and then annually. At each visit, evaluation of symptom, clinical examination of the hip including the range of motion, and plain radiograph of the operated hips were recorded. We checked for the deterioration of hip symptoms and looked for signs of progressive graft failure including tenderness, leg length discrepancy and limitation in range of motion of affected hip that might warrant joint replacement as a salvage procedure. Post-operative computer tomography (Figure 3) and magnetic resonance imaging of operated hip were also performed in some selected patients.

Forty-two years old man suffered from Ficat stage 2 ONFH. Post-operative computer tomography (CT) were taken 1 year after VIBG. (a) MRI and (b) 3D reconstruction image of the CT scan showed good integration of bone graft with proximal femur.
Statistical analysis
Statistical analysis was performed using SPSS version 24. The time of VIBG survival, as well as patient age, follow-up times and operative time were expressed as the mean and standard deviation with the minimum and maximum. Kaplan–Meier method was used for the overall graft-survival estimate and those according to Ficat stages. The data of graft-survival and graft-failure group were compared by Pearson’s χ2 test, Mann–Whitney U test and t-test. The hazard ratio of graft failure for the various patient factors and disease factors was calculated by univariate cox regression. A p-value of less than 0.05 was considered significant.
Results
Forty-two patients (50 hips) were included in the study (Table 1). Twenty-eight hips (56%) had surviving VIBG for the duration of follow-up. The overall median graft survival was 14.5 ± 7.8 years (0.4–24.0). Among 28 hips with surviving VIBG, the femoral head was still spherical in 16 hips while collapsed femoral head was noted in 12 hips at the latest follow-up. 25% of patients with surviving VIBG were able to perform active events (such as contact sports and labour work), 54% of them participated in moderate activity (such as swimming, jogging and unlimited housework) and 21% of them in mild activities (such as walking, limited shopping and limited housework).
Overall demographics and basic data of patients.

Of the 22 hips (44%) with the failure of VIBG, the median graft survival was 4.8 ± 6.8 years (0.4–22.0). All 22 hips were converted to cementless total hip replacement (THR).
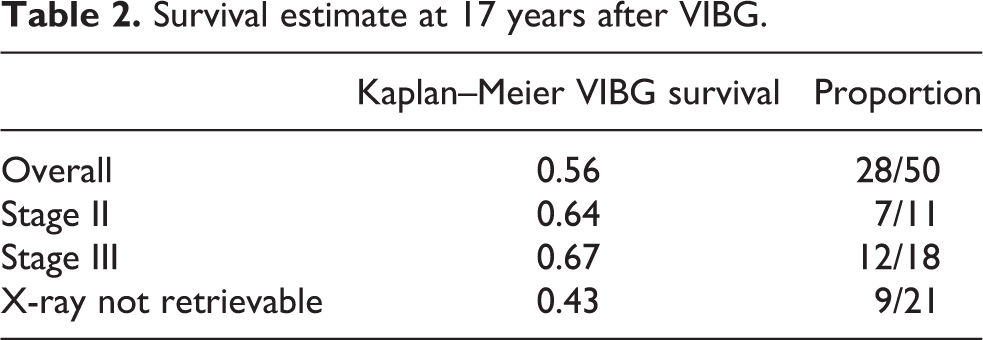
The VIBG survival estimates (Table 2) were analysed by Kaplan–Meier method for all hips (Figure 4) and for hips with retrievable X-ray (Figure 5), respectively. Pre-operative radiograph of 21 hips were not retrievable as the X-ray films were destroyed.

Kaplan–Meier VIBG survival curve for all hips.

Kaplan–Meier VIBG survival curve for hips with X-ray retrieved.
Survival estimate at 17 years after VIBG.
Pre-operative MRI scans were available in 18 hips (36%) only. The locations and sizes of necrotic area in these 18 hips were measured based on the MRI scan. The necrotic area of all 18 hips were located in the weight-bearing area, in other words, in the superolateral aspect of the femoral head. The necrotic area involved 30% of articular surface in three hips, 40% of articular surface in two hips, 60% of articular surface in one hip, 70% of articular surface in six hips, 80% of articular surface in three hips and 90% of articular surface in three hips.
In 18 hips with pre-operative MRI scans, half of the VIBG survived. The greater the necrotic area of femoral head, the higher the risk of subsequent VIBG failure (p = 0.004). In the nine hips with failed VIBG, the median necrotic area of the articular surface on the femoral head was 80% while that on surviving VIBG was 40%.
The etiology of ONFH was different between graft-survival and graft-failure group (p = 0.047). Alcohol and steroid-induced osteonecrosis were more predominant in the graft-failure group (Table 3). Other factors, including patient age and gender, Ficat staging and follow-up time were of no difference between the two groups. Steroid and alcoholism had a hazard ratio of 2.33 and 2.07 respectively for graft failure, leading to subsequent THR conversion (p = 0.047) (Table 4).
Comparison of VIBG survival versus VIBG failure group.

Bold values p-value < 0.05, i.e. statistically significant.
Hazard ratios of various patient and disease factors to VIBG failure.

In term of complication, there was one case of groin wound infection which required surgical debridement. Otherwise no other complication was observed.
Discussion
Vascularized bone grafting (VBG) has been described to treat the pre-collapse and early post-collapse cases of osteonecrosis of the femoral head, which aims to joint and to defer the timing for joint replacement. DCIA pedicled bone grafting has been reported in several case series. 7 –10,12 –14 This is the first study on the long-term outcome of DCIA pedicle iliac bone grafting for ONFH beyond ten years. In this study, with an average follow-up of 17 years, we analyze the survivorship and the mean survival time of VIBG. Hazard ratios of various disease factors and patient factors are also investigated.
The overall survival of VIBG was satisfactory; 72% of hips survived more than 5 years and 52% of hips survived more than 10 years in this study. This study has the longest follow-up time compared to other studies 7 –10,12 –14 using DCIA pedicle bone grafting (Table 5). Only patients with minimum 5-year follow-up were included in our series, which would make the results more meaningful.
Comparison of our study to other studies in the literature with DICA pedicled bone graft.

The etiologies of ONFH do influence the VIBG survivorship. Patients with steroid or alcohol-induced ONFH had a higher hazard ratio of VIBG failure (p = 0.047), compared to idiopathic and post-traumatic causes. Other factors, including patient age, gender and Ficat staging, were not found to affect graft survival. However, ARCO staging was reported as a significant factor that influenced graft survival by others. Chen et al. 9 reported that the survivorship of ARCO stage IIIA was better than stage IIIB (p = 0.016), and Nagoya et al. 13 revealed ARCO stage II survived better than ARCO stage III (p = 0.001). In our study, 42% of pre-operative radiograph were not retrievable as the X-ray films were destroyed. This limitation could account for the insignificant VIBG survivorship difference in Ficat stage II and stage III in our study. In our opinion, VIBG should be cautiously performed in steroid or alcohol-induced ONFH with segmental collapse, as bone graft-failure rate was higher. Furthermore, the size and location of ONFH are important prognostic factors for disease progression. 15 It was noted that satisfactory results were more commonly found in the medial lesion (85%) than in lateral lesion (39%). 10
Satisfactory long-term outcome of free vascularized fibular grafting (FVFG) was reported in the literature. Eward et al. 16 showed 60% (39/65) of hips survived with the mean follow-up of 14.4 years, while Yoo et al. 17 revealed survivorship of hips reaching 90% (111/124) with a mean follow-up of 13.9 years. Nevertheless we considered VIBG more favourable than FVFG because no microsurgical repair is required. The mean operative time of VIBG in our series was 3 h only. Furthermore, there is a higher concern of donor site morbidity in FVFG, compared to VIBG. In one series, out of 1270 FVFG procedures, the complication rate was reported reaching 16.9% at an average of 8.3 years. 18 Donor site complications (11.5%) were more common than that of the recipient site (5.4%). Common donor site morbidities included great toe flexion contracture, ankle pain and sensory deficits.
All 22 patients with bone graft failure were converted to cementless total hip replacement in our study. Only one patient (4.5%) required revision of acetabular cup with the mean follow-up of 9.7 years. Issa et al. 19 reported THR survivorship was 95% and 97% following prior core decompression and non-vascularized bone grafting, respectively, with a mean follow-up of 6.3 years. On the other hand, patient with prior FVFG who underwent THR had greater operative time and blood loss. 20 Further studies are warranted on the outcome of THR following VIBG.
Primary total hip replacement was reported to have excellent results in ONFH. THR performed after 1990 reported a survival rate of 97% at a mean follow-up of 6 years, while THR performed before 1990 reported a survival rate of only 83% with a mean follow-up of 9 years. 21 The improvement in THR survival could be accounted by highly cross-link polyethylene, improved polyethylene sterilization and improvement of implant design. The 10-year THR survival rate in ONFH and hip osteoarthritis was 92.5% and 95.3%, respectively, which was not significant (p = 0.136). 22 Our institute also described excellent long-term survival of cementless THR in ONFH in 2015. 23 The 19-year survival was 97.1%, using revision for aseptic loosening as an end-point. Therefore, VIBG should only be performed in selective manner. THR is a good treatment option to patients with older age or lower activity level.
There are several limitations. Firstly, like all retrospective studies, there was a selection bias, a concern of inaccuracy of retrieved data and loss to follow-up in some patients. Fortunately, in our study, only one patient did not return to clinic after follow-up for 12 years. Secondly, revision surgery was used as an end-point. However, some patients might have a significant progression of osteoarthritis without converting to THR. The assessment of the overall function and quality of life were beyond the scope of this study but this is of importance. Thirdly, a pre-operative radiograph of 42% (21/50) of patients studied were not retrievable. The electronic imaging system was only available since year 2003 in our institute.
Conclusion
At a long-term follow-up of 17 years, our results showed that VIBG is effective in treating patients with pre-collapse (Ficat Stage II) and early post-collapse (Ficat stage III) in ONFH. Alcoholics and patients with steroid are at a higher risk of graft failure, so VIBG should be performed cautiously in these patients. VIBG is an intermediate operation until osteoarthritis sets in, either by progression of ONFH or natural degenerative change.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.