
Abstract
Introduction:
Volumetric measurements of benign tumors enable surgeons to trace volume changes during follow-up periods. For a volumetric measurement technique to be applicable, it should be easy, rapid, and inexpensive and should carry a high interobserver reliability. We aimed to assess the interobserver reliability of a volumetric measurement technique using the Cavalier’s principle of stereological methods.
Materials and methods:
The computerized tomography (CT) of 15 patients with a histopathologically confirmed diagnosis of enchondroma with variant tumor sizes and localizations was retrospectively reviewed for interobserver reliability evaluation of the volumetric stereological measurement with the Cavalier’s principle, V = t × [((SU) × d)/SL]2 × ΣP.
Results:
The volumes of the 15 tumors collected by the observers are demonstrated in Table 1. There was no statistical significance between the first and second observers (p = 0.000 and intraclass correlation coefficient = 0.970) and between the first and third observers (p = 0.000 and intraclass correlation coefficient = 0.981). No statistical significance was detected between the second and third observers (p = 0.000 and intraclass correlation coefficient = 0.976).
Conclusion:
The Cavalier’s principle with the stereological technique using the CT scans is an easy, rapid, and inexpensive technique in volumetric evaluation of enchondromas with a trustable interobserver reliability.
Introduction
All benign intramedullary bone tumors have variant volumes with a distinctive different clinical presentation, and most of the time, each tumor requires a unique array of follow-up protocol. 1 Intralesional curettage usually creates intramedullary defects with different volumes, and many surgeons still propose the use of autogenous bone grafts, polymethylmethacrylate cement, hydroxyapatite, and tricalcium phosphate to fill the defect and to prevent pathological fractures, while other surgeons don’t support using grafts and reported good results without filling the resultant postoperative defects. 2 –7 Enchondroma composes 2.6% of benign bone tumors, and they can be presented at any age. Fifty-nine percent enchondromas occur between 10 years and 39 years of age, and usually, they are asymptomatic in nature. 8 They are mostly presented in long tubular bones and composed of masses of hyaline cartilage in a lobular pattern. Classically, they are solitary in nature; however, they may present themselves as a multiple enchondromatosis to form Ollier’s disease. Small enchondromas carry the risk of 1% of malignant transformation, whereas large ones are prone to a more malignant transformation of 25%. 8 –10
Volumetric measurements of an enchondroma enable surgeons to trace volume changes during follow-up periods, estimate the resultant postoperative defect volumes for variant graft preparation for those who support defect filling, and permit following up of the defect volume changes for the other group of authors who doesn’t support defect fillings.
For a volumetric measurement technique to be applicable, it should be easy, rapid, and inexpensive and should carry a high interobserver reliability.
In this study, we aimed to assess the interobserver reliability of a volumetric measurement technique utilizing the Cavalier’s principle of stereological methods of variant sizes of enchondromas using the computerized tomography (CT) tools.
Materials and methods
Fifteen patients with a histopathologically confirmed diagnosis of enchondroma, had been followed up in our clinic since 2002, and were randomly chosen with variant tumor sizes and localizations for interobserver reliability evaluation of the volumetric stereological measurement with the Cavalier’s principle. Although any standard CT plan sections can be used in this method, however, to avoid the volume calculating bias during the study, the coronal plan sections of the CT of all patients were determined to apply the volumetric stereological measurements in all patients. Nine females and six males with an average age of 25 ± 7.58, range (16–41) years, were included in this study. The localizations of lesions were six in the proximal humerous, three in the distal femur, two in the proximal femur, three in the hand phalanges, and one in the metacarpal bone (Table 1).
Demographic data related to patients involved in the study and the volumes of variant tumors calculated by different observers.a

CI: confidence interval.
aCI = 95%.
Morphometric and stereological analyses
Enchondroma margins of each image were evaluated by two orthopedic surgeons and a radiologist in an interobserver manner. The area was calculated three times manually using stereological point grid system for each of the CT images (Figure 1). All measurements were performed blinded to subject details and data of any other results. An optimal plan was taken as the smallest size of anisotropic structures that may be measured in a stereological volumetric analysis of any plan; axial, sagittal, or coronal CT sections. Original images were exported as tiff image files, which were further subjected to stereological analysis. A uniform point grid with a point-associated area of 0.625 cm2 was randomly superimposed on each CT images using the “grid” plug-in installed with films. Points hitting the tumor were manually counted for volume estimation. The volumes were also estimated using the Cavalier’s principle of stereological methods as described in the previous studies 11,12 using the formula, V = t × [((SU) × d)/SL]2 × ΣP, where t is the section thickness, SU is the scale unit (the real length of the scale marked on the CTs), d is the distance between two points in the point grid, SL is the scale length (the actual measure of the scale on CTs), and P is the number of points counted. All data have been entered into a previously prepared Microsoft excel spreadsheet for automatic calculation of the outcomes of the above formula and the statistical evaluation parameters, including the nugget variance and the coefficient of error. In order to evaluate volumetrical analysis of the lesions, sections were identified by clear visualization of the tumour area. The point counts belonging to the sections were calculated, and the results were added to total point counts for each area separately, and thus, a volume value for each tumour slice was estimated. The stereological point counting method is demonstrated in Figure 2.
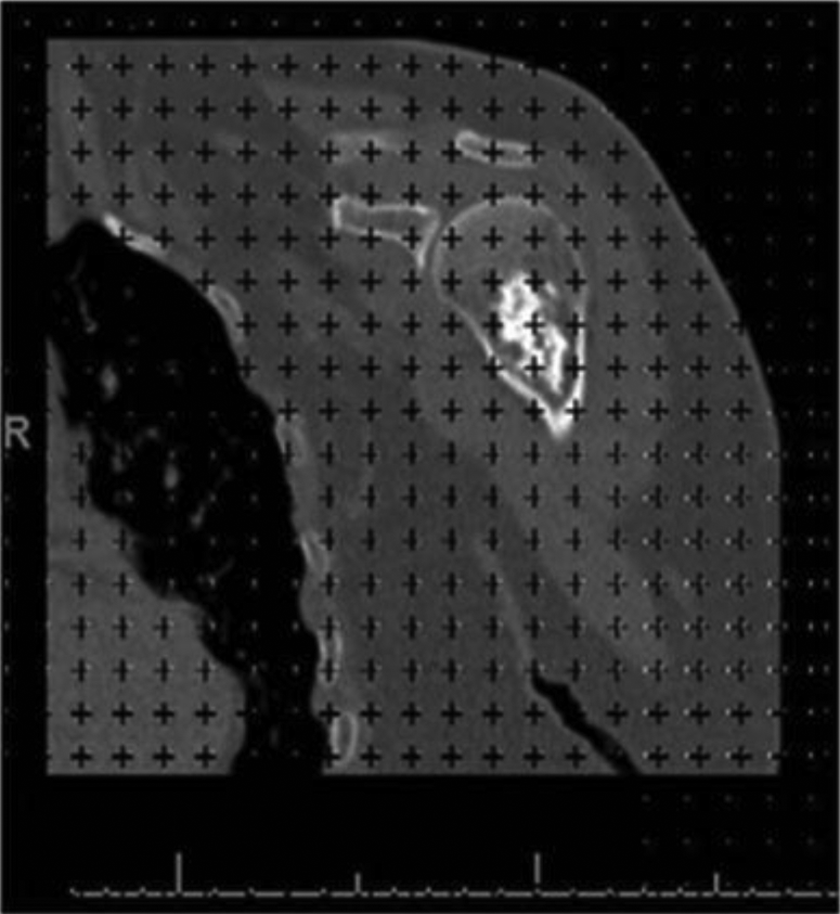
A coronal section of a CT of proximal homeruns enchondroma. Original images were exported as tiff image files, which were further subjected to stereological analysis. A uniform point grid with a point-associated area of 0.625 cm2 was randomly superimposed on each CT images using the “grid” plug-in installed with films. Points hitting the tumor were manually counted for volume estimation. CT: computerized tomography.

The volumes were estimated using the Cavalier’s principle of stereological method using the formula, V = t × [((SU) × d)/SL]2 × ΣP, where t is the section thickness, SU is the scale unit (the real length of the scale marked on the CTs), d is the distance between two points in the point grid, SL is the scale length (the actual measure of the scale on CTs), and P is the number of points counted. CT: computerized tomography.
The SPSS software (version 15.0 for Windows, IBM Corp., NY, USA) was used for data processing to determine the intraclass correlation coefficient for statistical evaluation of the collected data between the observers. The level of significance was set up as p < 0.05.
Results
Two orthopedic surgeons and one radiologist have revised the coronal CTs in a blinded manner, with each area calculated three times manually using stereological point grid system for each of the CT images. The volume of each tumor was calculated three times using the Cavalier’s principle of stereological methods. The volumes of the 15 tumors collected by the observers are demonstrated in Table 1. There was no statistical significance between the first and second observers (p = 0.000 and intraclass correlation coefficient = 0.970) and between the first and third observers (p = 0.000 and intraclass correlation coefficient = 0.981). No statistical significance was detected between the second and third observers (p = 0.000 and intraclass correlation coefficient = 0.976).
Discussion
Most enchondromas follow a benign course throughout lifetime; however, they carry the risk of malignant transformation of 1% when they are solitary and about 30% in multiple enchondromatosis; Ollier’s disease. 13,14
The behavior of these tumors is very hard to be predicted from the conventional evaluation techniques, such as size follow-up and histological appearance. Many studies had been conducted in a trial to predict their potential for malignant transformation but most of which have failed. 15
Hirna et al. 16 had described a volume determination method of bony defects where they depended on preoperative radiographs to examine and measure the size of benign tumors. They described two formulas: one for cylindrical and another for spherical lesions. The volume calculations were done as follows: cylinder defect = ABC × 0.785, that is, (π × A/2 × B/2 × C); and spherical defect = ABC × 0.52, that is, (4/3 × π × A/2 × B/2 × C/2), where A is width, B is depth, and C is height.
The most appropriate of the two formulas was used, depending on the perceived shape of the defect. However, it lacks the blinded interobserver sensitivity and the three-dimensional evaluation pattern.
Cavalier’s principle had been employed by several researchers to calculate the volumetric changes of cerebellum and cerebrum in many diseases. 16,17 There is no agreement between researchers on the volumetric changes of benign tumors during follow-up. Quantitative analysis of CT imaging may improve its diagnostic yield. However, there is still an ambiguity and debate related to the definitions of volumetric measurement methods of benign tumoral structures in the literature, frequently used measures are known as planimetry, automatic, and three-dimensional. Many researchers had documented that the automatic method is an efficient quick, and unbiased, and it is not subjected to issues like rater drift and will not be constrained to poor interobserver reliability. However, other authors reported that the planimetry measurement method is to be the “gold standard” when compared to the automatic method. 18,19 Differing from previous studies, we adopted the stereological measurement technique, which was first used in evaluation of cerebellar asymmetry by Gocmen-Mas. 20
The Cavalier’s principle using the stereological technique is an easy, trustable, unbiased, and inexpensive, and the adopted point counting approach takes less time as well. It is an efficient method for estimating volumes in MRs: Magnetic resonance imagings and CTs: Computerized tomographies. 20,21
In this study, the volumes of enchondromas in variant localization of the body were measured by three observers using the CT method to determine the interobserver reliability of such a method in determining the volumes of benign tumorous lesions like enchondromas. Volumetric measurement is crucial through follow-up periods to detect early malignant transformation, to estimate the defect that may result after surgical intervention, and to preoperatively evaluate the volume of defect that may result for the grafting material preparation.
Obviously, resampling to many studies, our study also has some limitations, the sample size of our study is small, and we only evaluated enchondroma patients. Further studies should be conducted involving greater numbers of patients involving other cystic benign lesions, which would be helpful to support and extend our findings in this study.
Conclusion
The Cavalier’s principle with the stereological technique using the CT scans is an easy, rapid, and inexpensive technique in volumetric evaluation of enchondromas with a trustable interobserver reliability.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.