
Abstract
The growing spine differs from the adult spine in several ways. Although tumors and infections cause only a small percentage of pediatric back pain incidences, delayed proper diagnosis and treatment may be disastrous. Benign lesions, such as osteoid osteoma, osteoblastoma, and aneurysmal bone cyst in the spine, are predominant during the first two decades of life, whereas malignant bony spinal tumors are rare. In the pediatric population, malignant spine tumors include osteosarcoma, Ewing’s sarcoma, lymphoma, and metastatic neuroblastoma. Infections of the growing spine are rare, with the incidence of discitis peaking in patients under the age of 5 years and that of vertebral osteomyelitis peaking in older children. Spondylodiscitis is often a benign, self-limiting condition with low potential for bone destruction. Conservative treatments, including bedrest, immobilization, and antibiotics, are usually sufficient. Spinal tuberculosis is a frequently observed form of skeletal tuberculosis, especially in developing countries. Indications for surgical treatment include neurologic deficit, spinal instability, progressive kyphosis, late-onset paraplegia, and advanced disease unresponsive to nonoperative treatment. Spinal tumors and infections should be considered potential diagnoses in cases with spinal pain unrelated to the child’s activity, accompanied by fever, malaise, and weight loss. In spinal tumors, early diagnosis, fast and adequate multidisciplinary management, appropriate en bloc resection, and reconstruction improve local control, survival, and quality of life. Pyogenic, hematogenous spondylodiscitis is the most common spinal infection; however, tuberculosis-induced spondylodiscitis should also be considered.
Introduction
The growing spine has characteristics that differ from those of the adult spine. In young children, the vertebral metaphyseal area has a rich vascular ring, crossing the vertebral cartilaginous end plate and connecting branches of the disk periphery. These vessels disappear at the age of 8 years. 1 Epidural space is a valveless venous plexus (Batson’s venous plexus). These vascular characteristics of the growing spine provide a route for the invasion and dissemination of infections and tumors, and the courses differ from those observed in adults. 2
Structural pathology is a more common cause of back pain in children (especially before the age of 10 years) than in adults. The differential diagnosis of back pain in children is broad; therefore, clinical awareness, meticulous examination, and imaging (plain radiography and computed topography or magnetic resonance imaging (CT/MRI) when necessary) are important. 3 The diagnostic work-up should consider patient’s age, type of pain, dynamics of symptoms, possible neurological deficits, and, of course, imaging results.
Although tumors and infections cause only a small percentage of pediatric back pain incidences, a delay of proper diagnosis and treatment may be disastrous. Back pain in a growing child should always be seriously considered before pathologies that require early treatment are ruled out.
Tumors
Metastases are the most common tumors in the spine in the general population but not in children. In contrast, benign lesions are predominant in the first two decades of life (Table 1). 4 The main symptom of the tumors is nonspecific back pain. Benign tumors pose a problem, as their locally aggressive growth may compress surrounding structures, especially neural elements (spinal cord and nerve roots), thereby leading to neurological deficits. In addition, tumors can result in deformities, such secondary scoliosis, kyphosis, and dynamic torticollis (Figures 1–3). Although most tumors and tumor-like conditions of the pediatric spine are benign, many of them may require interventional or surgical treatment. 3
Spinal tumors.
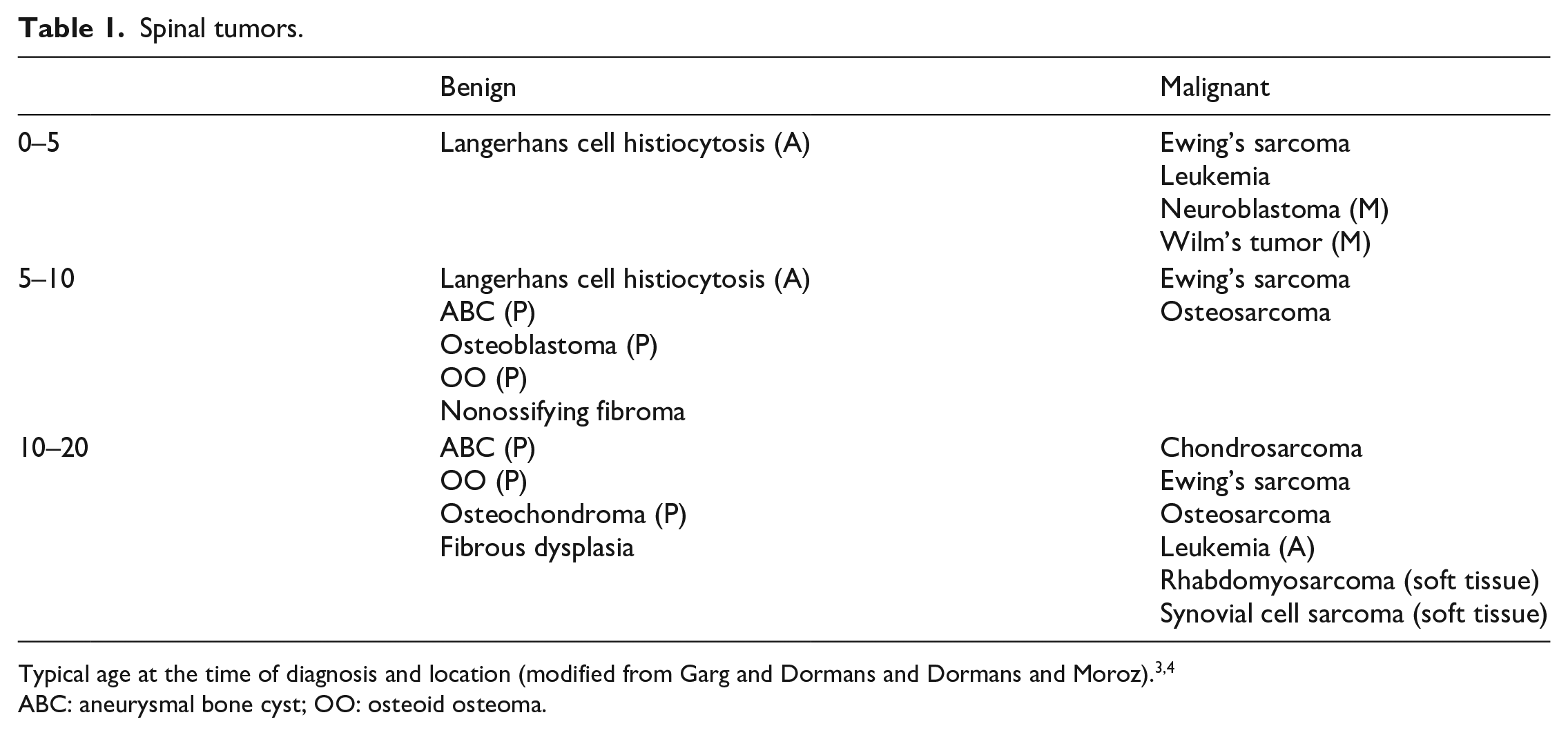
Typical age at the time of diagnosis and location (modified from Garg and Dormans and Dormans and Moroz).3,4
ABC: aneurysmal bone cyst; OO: osteoid osteoma.
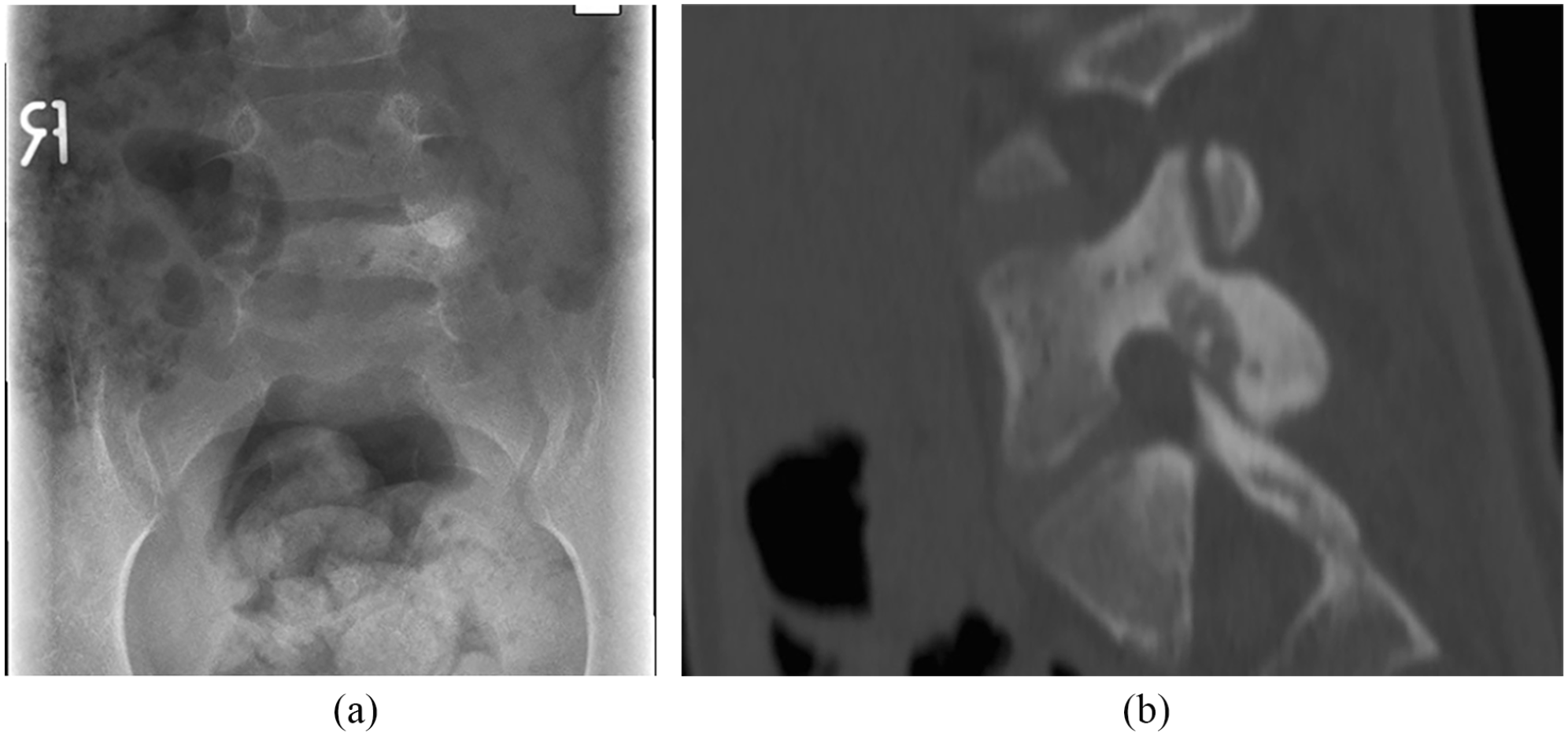
A 6-year-old girl with low back pain and positive “Aspirin effect”: (a) standing posteroanterior lumbar radiograph showing sclerosis of the left L5 pedicle and (b) sagittal computed topography reformat showing typical osteoid osteoma of the L5 pars interarticularis. Patient was treated with en bloc excision.
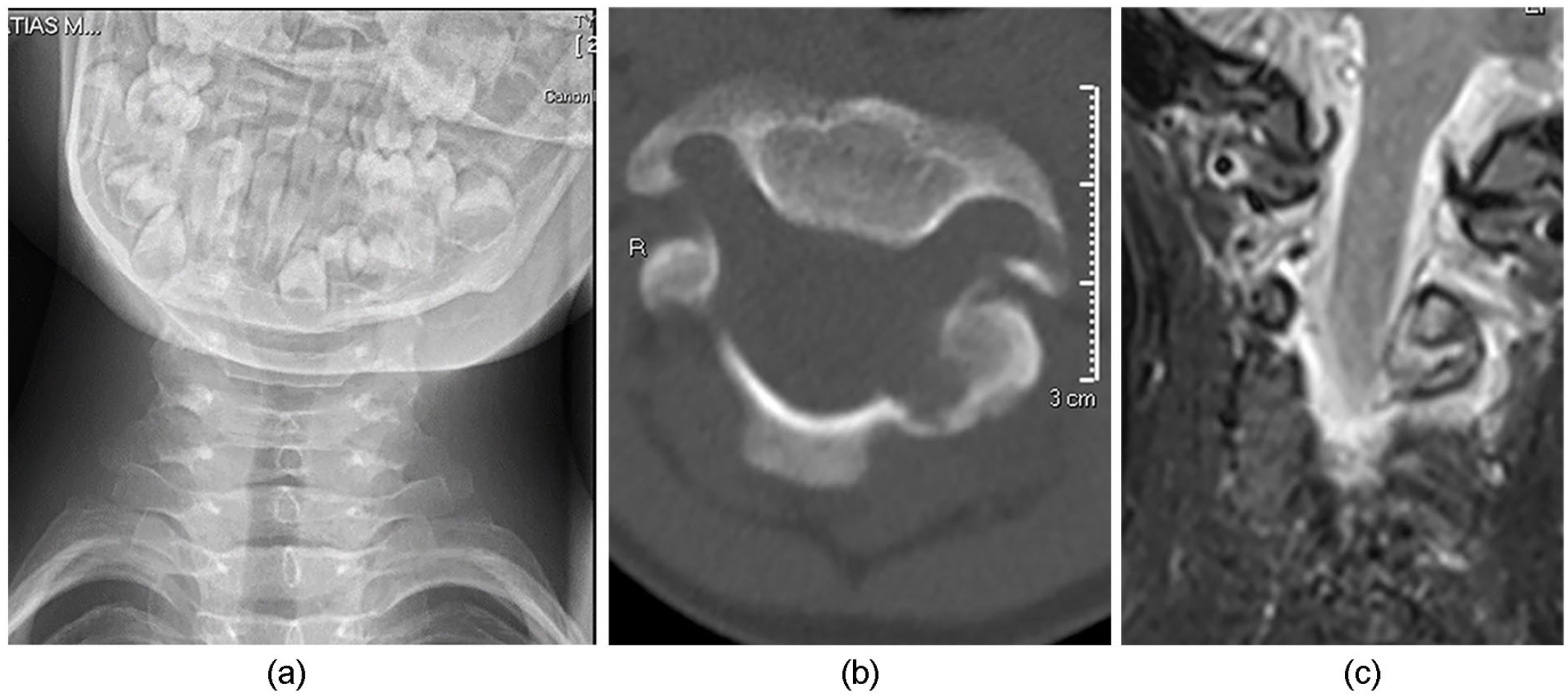
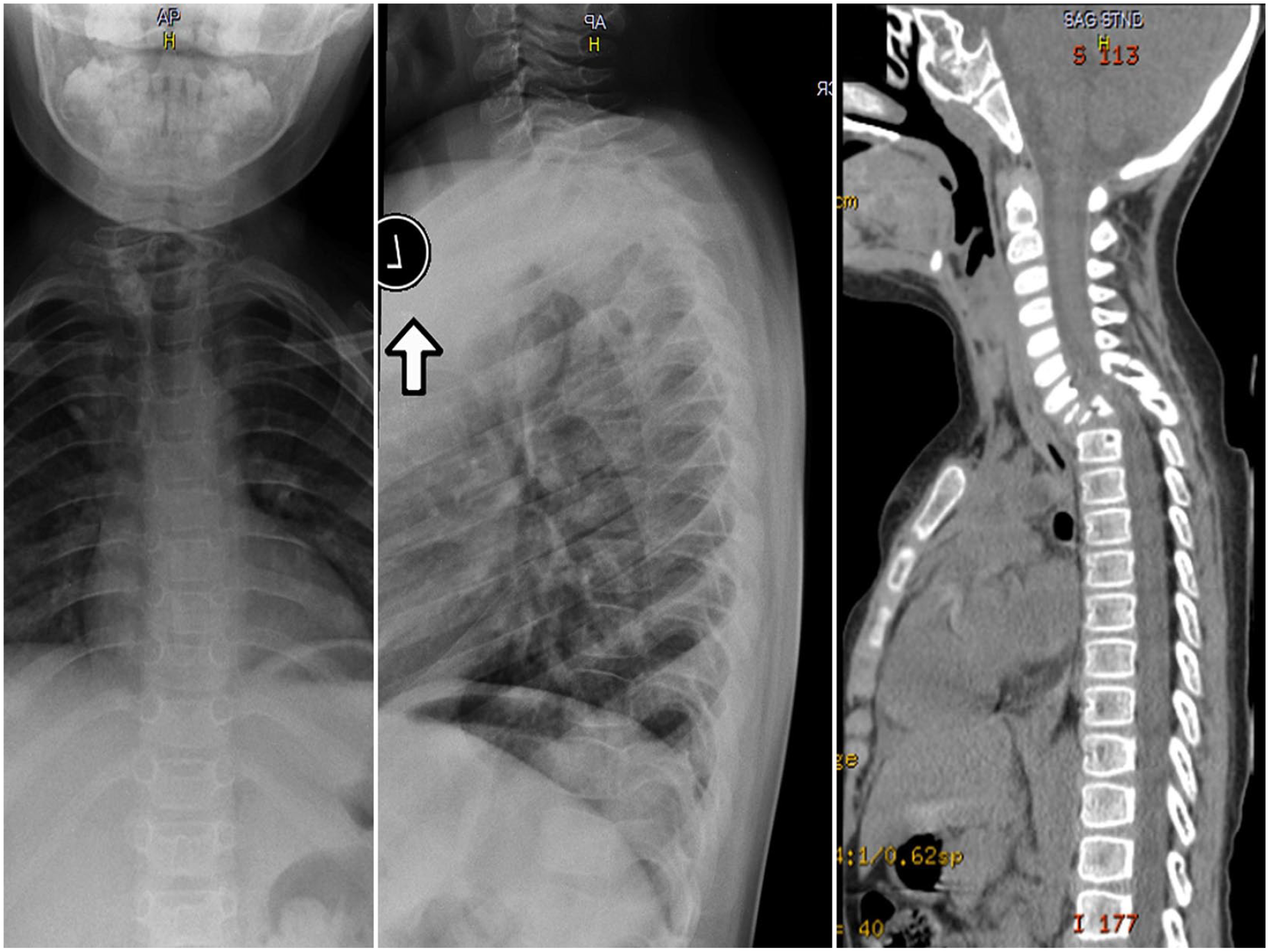
A 5-year-old boy presenting with unresolving torticollis: (a) anteroposterior cervical radiograph showing unresolving torticollis after 3 days in Glisson traction; (b) axial cervical computed topography showing C3 posterior element osteoblastoma in contact with vertebral artery channel; (c) coronal T2 magnetic resonance image of the cervical posterior elements showing enlargement of C3 pedicle and tumor. Treated with en bloc excision and short instrumentation.
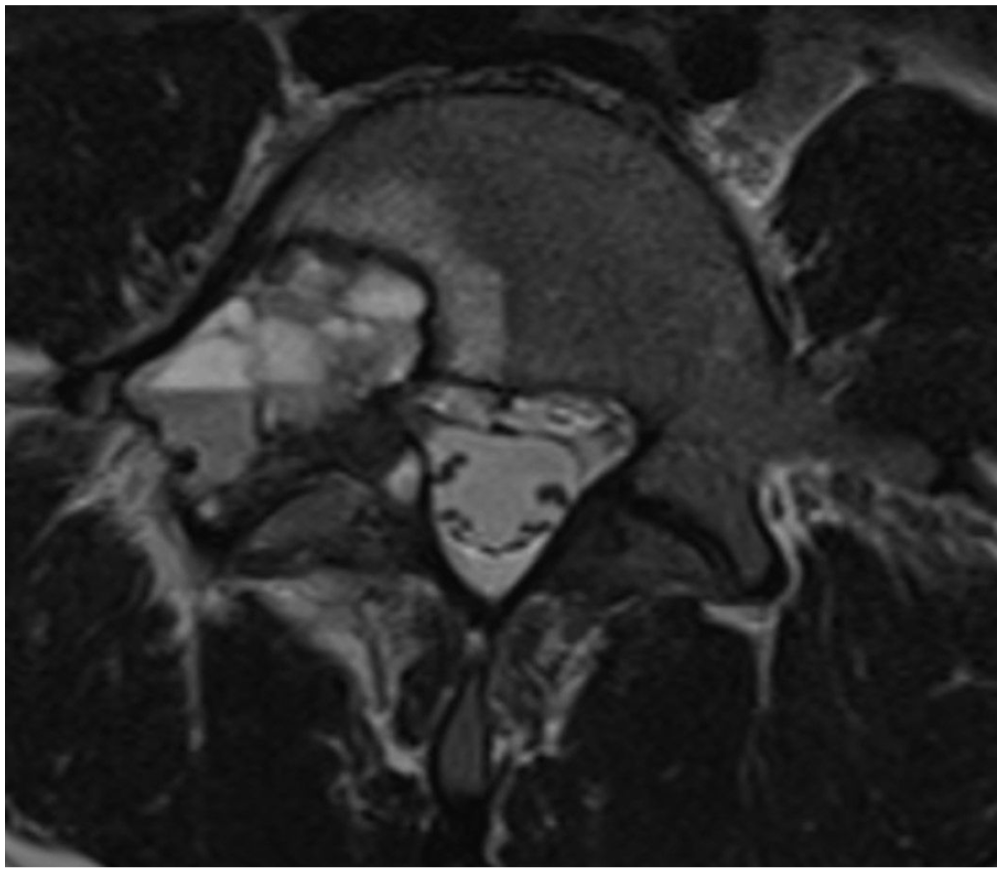
A 14-year-old boy with low back, but no neurologic symptoms. Axial T2-weighted magnetic resonance image showing typical aneurysmal bone cyst on the right posterior elements of L5.
Malignant bone tumors of the spine
Malignant bony spinal tumors are infrequent in children and adolescents.4 –6 Malignant osseous spinal tumors such as osteosarcoma, Ewing’s sarcoma, lymphoma, and metastatic neuroblastoma are typical for the pediatric population.4,6,7 Almost 50% of bony Ewing’s sarcomas occur in the axial skeleton (spine, pelvis, and ribs), and this axial location is a poor prognostic sign (Figure 4). The overall incidence of bone sarcomas among children and adolescents (below 18 years of age) is 5.1 per 1 million people: 3.6 for osteosarcoma, 1.2 for Ewing’s sarcoma, and 0.3 for chondrosarcoma. 5 The axial skeleton is involved in approximately one-fourth of these cases.7–9 Serlo et al. 9 reported 24% pediatric bone sarcomas in the axial skeleton in Finland, with a 10-year overall survival rate of 82% if the disease was localized at diagnosis.
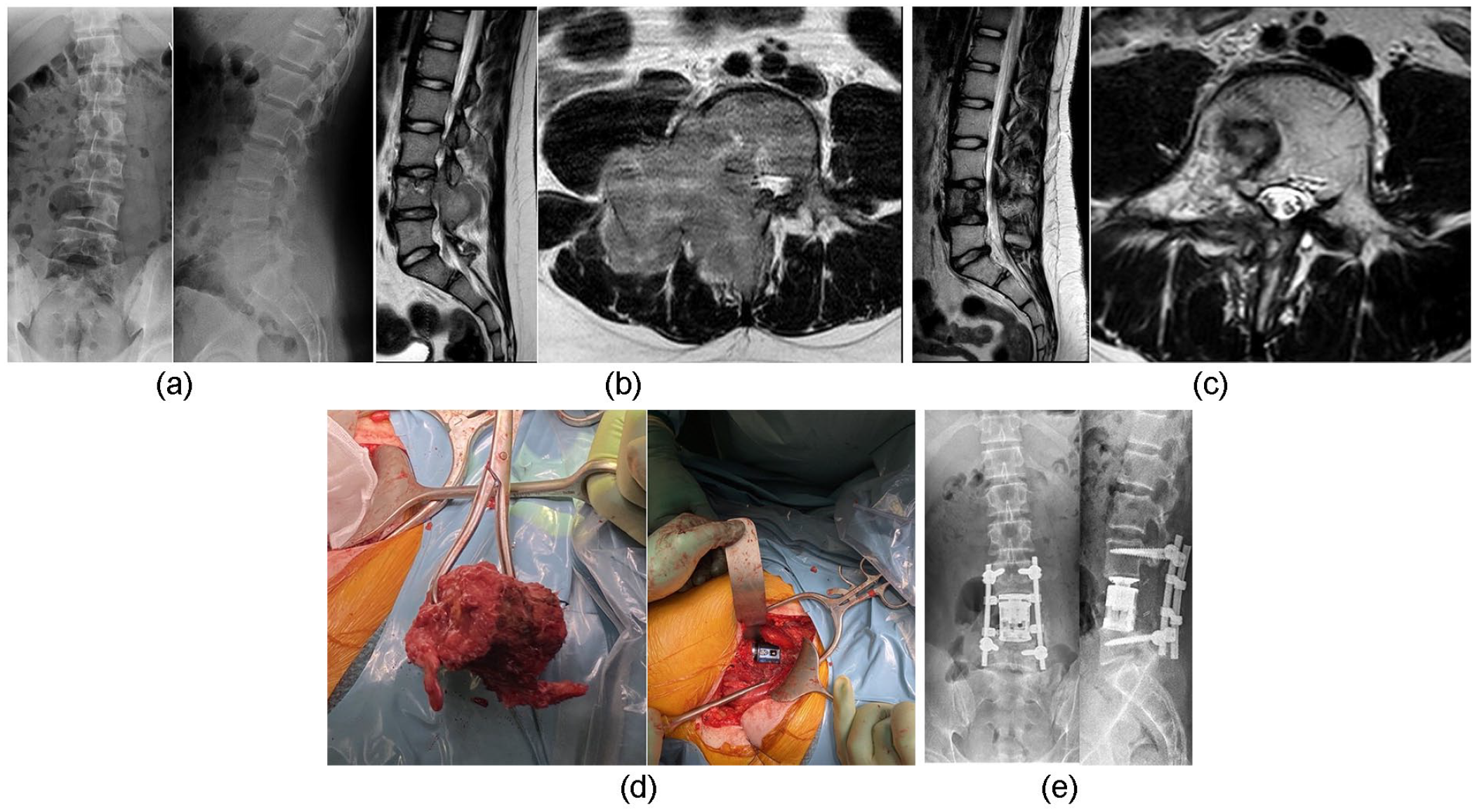
A 15-year-old boy with low back pain and right-sided radicular pain (L4 dermatome): (a) standing posteroanterior and lateral lumbar radiographs showing missing L4 pedicle; (b) sagittal and axial T2-weighted lumbar MR image demonstrating L4 posterior element, pedicle and vertebral body tumor extending to surrounding paraspinal muscles, epidural space, and L4 nerve channel. Transpedicular computed topography-guided biopsy confirmed Ewing’s sarcoma; (c) sagittal and axial T2-weighted MR images showing complete resolution of soft tissue tumor after 12 weeks preoperative chemotherapy and proton therapy; (d) combined approach and en bloc excision of posterior elements and intraoperative images of en bloc spondylectomy specimen and reconstruction using an expandable cage. Right L4 nerve root was sacrificed; (e) postoperative standing lumbar posteroanterior and lateral radiographs 7 months after index procedure.
Besides bony tumors, there are also spinal cord tumors, which grow inside the spinal canal. The most common intramedullary lesions are astrocytomas and ependymomas.2,10
Symptoms
The symptoms of axial bone tumors include back pain or inguinal pain, which is typically a dull night pain that is unrelated to physical activities.4,6,11 –14 Spinal deformity, regional stiffness, and neurologic deficits may occur; however, these symptoms are less common. Neurologic deficits are less prevalent in the pediatric population; however, large soft tissue mass may cause spinal cord or nerve root compression, which is followed by various neurologic symptoms (Figure 4). 6 Walking difficulties are typical neurologic deficits. Intramedullary tumors can present more acutely with progressive loss of neurological function, especially in severe cases of spinal canal stenosis. 2 Constitutional symptoms such as fever, weight loss, and night sweating are observable in some patients, especially in those with Ewing’s sarcoma. 7
The time interval between the onset of symptoms and diagnosis of spinal or pelvic tumors is usually significantly extended (average: 7 months) because the growth of the tumor may be unnoticeable to a certain degree.7,12,13 Typical symptoms and physical examination findings include buttock pain, lower back pain, limited spinal movement, hip and groin pain, bladder dysfunction, and sciatic nerve symptoms.12,13 Early symptoms can be minimal, subjective, and noncharacteristic.
Diagnostics
A complete clinical investigation of the child is indicated when there is a clinical suspicion of axial bone tumor.4,6 Palpation of the tumor area may evoke the pain; however, this is hardly possible in most cases of intrathoracic and retroperitoneal growth. Neurological examination may reveal some neurologic findings, including positive Babinski reflex, brisk patella, and Achilles (due to cord compression) or attenuated reflexes (nerve root compression), depending on the location of the tumor. The straight leg raising test is a sensitive tool; it shows positive results quite early, following nerve root or spinal cord compression (Figure 4). Screening tests such as heel and toe walking tests are sensitive to the neurological function of the lower extremities, including general strength and ataxia (spinal cord compression and myelopathy), supplemented by active motion in the hip, knee, and ankles. 7 Furthermore, rectal tone is valuable for the diagnosis of cauda equina lesions.6,7
When the patient is presenting with the abovementioned symptoms or with obvious palpable paraspinal mass or deformity, standing radiographs of the whole spine are indicated.4 –6,11 –14 Radiological diagnosis of spinal tumors using plain radiographs only is difficult; therefore, patients should be evaluated via MRI (with intravenous contrast if necessary). Primary malignant bone tumors rarely occur before school age, whereas infections and other pediatric cancers (leukemia and neuroblastoma) are more common. 4 Typical imaging findings in malignant bone tumors are soft tissue mass and various bone destructions (Figure 4).
The diagnosis of malignant tumors should be confirmed by a well-planned biopsy performed according to the principles of oncologic orthopedics.4,6,7 Percutaneous biopsy should be preferred since the associated 0.37% risk of tumor cell seeding is significantly lower than the 32% risk associated with open biopsy.15,16 Advanced imaging techniques allow percutaneous biopsy; preferably, CT guidance is used after interdisciplinary planning. At the spine, percutaneous biopsy should be performed via the pedicle, as a relatively easy access to the vertebral body. Transthoracic biopsies should be avoided, as they can contaminate the whole chest cavity. A malignant bone tumor can often be diagnosed not only from bony material but also from the soft tissue component of the tumor. 7
Before planning treatment, proper staging is crucial. There are two well-known staging systems for spinal tumor classification and treatment planning. 17 The first was published by Enneking in 1986. 18 The author divided all lesions into inactive (observation), active, and locally aggressive (malignant bone tumors), staging tumor according to biologic aggressiveness, anatomic extent, and presence of metastases. 17 The second classification, described by Weinstein, Boriani, and Biagini, is known as the WBB system (Weinstein-Boriani-Biagini anatomic classification system) and considers the anatomical complexity of the spine. The basic concept of this staging system is sparing of spinal cord without compromising the surgical margins. 19 The WBB system divides the vertebra into zone and layers. Twelve radiating zones divide the spine in an axial plane, while five concentric layers are centered around the dura sac.17,19
Treatment
Advances in chemotherapy and surgical treatment have changed the current treatment modality. The management of the most common malignant axial tumors (Ewing’s sarcoma and high-grade osteosarcoma) in children starts with a neoadjuvant therapy and ends with postoperative chemotherapy regardless of neurologic compromise. Prompt initiation of neoadjuvant chemotherapy, including corticosteroids, has been shown to improve neurologic deficits; in the cases sensitive to chemotherapy, it should be the primary management (Figure 4).7,20
Typically, the surgical window opens after 10–12 weeks of oncologic management. The anatomy of spine and neural elements does not allow radical tumor resection; therefore, resections of tumors in the spine are typically marginal or wide. 19 Notably, there is often only one good chance to perform curative en bloc resection for malignant spine tumors and surgery should be performed only by the most experienced orthopedic spine surgeons. Although there is no possibility of radical excision, surgery is still considered beneficial, at least when marginal resections within anatomical barriers are achievable.11,14,19,21 –23 In radiation-sensitive bone tumors like Ewing’s sarcoma or in high-grade osteosarcomas, proton radiation therapy could be an alternative or additional adjuvant treatment option. 7
Additional procedures such as preoperative embolization of large tumors, aortic balloon occlusion, or application of a temporary stoma in case of sacrum tumors can be helpful in reducing the risk of intraoperative or postoperative complications like massive blood loss or infection.7,24
Surgical procedures employed in en bloc resection can be divided into three groups: spondylectomy (removal of full vertebral body en bloc with or without posterior elements) (Figure 4), sagittal resection through the spine, and posterior arch resection. 19 Surgical staging systems help in choosing the most suitable technique. In addition to the previously mentioned WBB and Enneking systems, the Tomita system also can be useful. 25 This system was developed particularly for spinal metastases, considering three prognostic factors: grade of malignancy, visceral metastases, and bone metastases.25,26
Resection of the whole vertebra (en bloc spondylectomy) can be performed via a posterior-only approach or a combined anterior and posterior approach, depending on the extent of the lesion, part of spine, and surgical staging of the tumor.27,28
One pedicle free of the tumor is a requirement for marginal en bloc tumor resections; otherwise, the operation will be intralesional.19,25,27 A combined approach is usually necessary in cases of a large tumor extension outside the vertebral body, as this will allow full excision of the tumor with adequate margins (Figure 4). Anterior approach can include cervical, transthoracic, lumbotomy, or laparotomy. Nerve root sacrifice may be needed to obtain surgical margins.
The Tomita procedure (en bloc spondylectomy from posterior approach only) encompasses a wide bilateral posterolateral approach. 25 To perform this approach, two or three pairs of ribs around the malignant tumor must be cutoff from the vertebral body 5 cm laterally. Pleura and large vessels are dissected away from the spine using blunt dissection. A space is created around the spine and the anterior longitudinal ligament, disks, as well as the posterior longitudinal ligament above and below the vertebral body are cut to allow removal of the body en bloc. 7 During surgery, the spine is stabilized using pedicle screw instrumentation typically one (lumbar) or three pairs above and below.
The defect between the remaining adjacent vertebral bodies is reconstructed using an allograft or expandable titanium cage (Figure 4). Afterward, the spine becomes stable, allowing for early mobilization, postoperative radiotherapy, and continuation of the neoadjuvant therapy. Laminectomy, with excision of the posterior elements of the spine, requires instrumentation and spinal fusion to avoid postlaminectomy kyphosis. 29
Successful en bloc resection has been shown to improve survival in chondrosarcoma and osteosarcoma.30 –32 In Ewing’s sarcoma, en bloc spondylectomy combined with radiotherapy seems to be beneficial for local control. 33 Neoadjuvant chemotherapy is highly recommended in spinal Ewing’s sarcoma even if the patient presents with neurological deficits because the soft tissue mass will typically disappear after chemotherapy, which makes the excision possible and more effective (Figure 4). 20
En bloc spondylectomy is an extensive surgery, with common minor and major complications such as deep surgical site infection, cerebrospinal fluid leakage, and neurologic deficits; therefore, the decision to perform total en bloc spondylectomy should be made by an experienced multidisciplinary team. 34
Prognosis
There are very limited data on the prognosis of primary malignant bony spine tumors in children. Usually, the results of treatment are presented for both children and adults. According to SEER (the Surveillance, Epidemiology, and End Results database, USA), the 5-year survival rate is approximately 18% in all patient age groups with primary spine osteosarcoma and 41% in those with spine Ewing’s sarcoma.21,35 In a Finnish nationwide retrospective study, children with axial Ewing’s sarcoma had a significantly lower 10-year survival (56%) than children with a peripheral tumor location (100%). 9 The majority of patients with Ewing’s sarcoma experienced a favorable outcome, with respect to independence status, following surgery and adjunctive treatment; however, the 5-year survival rate was 57%, with the increased risk of recurrence and death between 14 and 20 years of age. 36 Full chemotherapy response (100% necrosis rate) was a predictor of local recurrence in Ewing’s sarcoma, with the lowest recurrence rate for patients with good chemotherapy response who underwent radiotherapy and surgery.
In children with osteosarcoma, chemotherapy response and surgical margin affected local control. Advances in chemotherapy and surgery transformed osteosarcoma from an almost universally fatal disease to a disease that most patients can survive. Although the treatment outcome has improved in recent years, patients with lung metastasis and chemotherapy resistance await an effective treatment. 37
Luzzati et al. 38 described the results of en bloc spondylectomy in spine tumors with 79.5% survival rate at 5 years; however, his group was heterogeneous including other tumors besides high-grade tumors. Reconstruction in the growing spine may be challenging, as 40% of patients had at least one late complication, which was most often hardware failure or nonunion. 38 If en bloc osteosarcoma excision is not primarily performed, aggressive use of revision tumor surgery and multimodal adjuvant therapy may improve outcomes. 39
Benign tumors and tumor-like conditions
Primary benign spine tumors are uncommon in the general population but are more prevalent in children and adolescents. They may be incidental findings and may cause local pain with or without radicular symptoms. Neurologic deficits and spinal instability are also possible symptoms; however, they are rarer than they are in malignant tumors. 40 Benign spine tumors classified as stage 2 (active) and 3 (locally aggressive) the Enneking staging system require treatment. 40
Osteoid osteoma
An osteoid osteoma (OO) is a relatively common benign tumor that occur in long bones (femur and tibia) and the spine (10% of cases). The tumor occurs more in males than in females, typically presenting the first and second decades of life. OO is a small, bone-forming tumor, with osteoblasts that produce osteoid and woven bone. 41 The tumor is usually located in the posterior spinal elements (spinous processes, transverse processes, lamina, pedicles, and facets), with occurrence in vertebral body a rarity (Figure 1).40 –42 The most common localization is in the lumbar spine, followed by cervical and thoracic localizations. The main symptom is pain, which increases over time and may occur at night. The pain subsides after nonsteroidal anti-inflammatory drugs (NSAIDs), an effect known as the aspirin effect. Diagnosis is often delayed, occurring after weeks or months of back pain. OO is regarded as the most common cause of painful scoliosis due to muscle spasm, and lesion is usually on the concavity of the curve. Typically, there are no associated neurologic deficits. Imaging should begin with plain radiography; however, the lesion may be not visible at all in the early stages and may only be visible in the subtle area of sclerosis in the later stages. A typical OO image shows sclerosis surrounding a radiolucent nidus, with a diameter of 15–20 mm. CT typically provides diagnosis. OO can be treated conservatively (pain management), as some tumors regress spontaneously within 2–6 years. 42 NSAID therapy-refractory pain and activity limitations are indications for surgery. Treatment options include open en bloc excision, intralesional curettage, or minimally invasive radiofrequency (or laser) ablation. 42 Radiofrequency ablation is becoming more popular as a minimally invasive and highly effective technique; however, its use in the spine remains controversial because proximity of spinal canal and spinal cord is important while high-frequency currency creates a small heated region with coagulation necrosis around electrode. 42 This thermal effect can be reduced, for example, by the application of saline into the epidural space.
Osteoblastoma
Osteoblastoma is a benign primary bone tumor, with a peak incidence during the second and third decades of life, mostly in children aged 10–15 years (Figure 2). The most common localization is the spine (up to one-third of cases), with strong predilection to posterior elements (lamina and pedicles). 43 Osteoblastoma is a benign bone-forming tumor histologically similar to OO; both tumors are variants of the same basic lesional process of osteoblastic derivation. 43 Osteoblastoma is clinically and radiologically more aggressive than OO, although it is benign; it can cause more bone destruction, soft tissue infiltration, and epidural extension (“mass effect”).43,44 These tumors behave more aggressively, with extensive local recurrence and even malignant-type transformation (rare), followed by metastatic disease. 45 Typically, the main symptom is regional back pain (nocturnal pain), sometimes with atypical scoliosis. Neurologic deficits can result from bone destruction and spinal canal stenosis (mass effect), in the form of nerve root symptoms, and spinal cord compression with various degrees of sensory and motor deficits. 43 Because of nonspecific symptoms, the diagnosis of this tumor is often delayed. Thus, more severe neurologic deficits (paraparesis or paraplegia) occur in approximately one-third of patients, whereas minor radicular symptoms can occur in up to 50% of patients. Imaging modalities include plain radiographs, CT scans, and MRI, followed by needle or open biopsy. Plain radiography can show a dense shell of bone surrounding the lesion, somehow resembling OO. Bony shell can be very thin, with tumor expansion into adjacent soft tissues. Approximately 50% of patients’ radiographs can be normal.
CT scan is important for detailed diagnosis, including the extent of bone destruction and degree of sclerosis. MRI, although nonspecific, is a very sensitive tool in the assessment of spinal cord compression and paradural and epidural extensions.
Surgery, with en bloc resection, followed by reconstructive surgery to regain spine stability is the gold standard treatment strategy.43,46
Aneurysmal bone cyst
Aneurysmal bone cyst (ABC) is a rare, benign but expansile lesion composed of varying sizes of blood-filled spaces in a bone. Sometimes, it can be expansive and destructive. It occurs in young adults and children, with a peak incidence in patients between 10 and 20 years of age. The condition is most commonly localized in the femur and tibia but one-third can be found in spine. 47 The main symptom is focal pain or back pain, with neurologic manifestations common, especially when pathologic fracture occurs. 48 Located in the vertebral column, it undermines the structural integrity of the spine and neurologic complications can occur. 49 Plain radiographs show expansile, eccentric, and lytic lesions with bony septae (“bubbly appearance” or “blood-soaked sponge), classically with a thin rim of periosteal new bone-surrounding lesion (Figure 3).47,48 The typical image looks like “ballooning” of the vertebra with thin bony rim. 47 Further imaging includes MRI or CT scans showing multiseptated, well-defined cystic lesions with fluid levels, possibly expanding into soft tissues.
However, the cause of ABCs remains unknown; recently, primary ABCs have been associated with a translocation resulting into the activation of the ubiquitin-specific peptidase 6 (USP6) gene on chromosome 17.40,50,51
ABCs may have an unpredictable behavior, with a high recurrence rate after intralesional treatment.48,52 The treatment of ABC is controversial, with surgical and nonsurgical options described in the literature.47,48,52 Intervention under fluoroscopy with arterial embolization injection of sclerosing agent (polidocanol) or autologous bone marrow concentrate (BMC) may be considered, whereas surgery represents a standard treatment for spinal ABC. 52 When considering the high recurrence rate (10%–44% of cases) of ABC, the best option is en bloc resection with adequate spinal stabilization; however, the procedure can be difficult, especially in the cervical spine.47,48 Another option is intralesional excision: curettage and bone grafting, but is associated with local recurrence. In case of recurrence, en bloc excision is advocated. The clinical course of ABC is unpredictable but healing of the lesions is often achieved especially after en bloc excision.
The newest research shows another solution. Denosumab is an inhibitor of receptor activator of nuclear factor kappa-Β ligand (RANKL), which works by decreasing the development of osteoclasts. 53 Denosumab may be a new option for the treatment of ABC.54 –56 It allows bone formation and tumor regression. It can be especially useful in the cases of ABC when surgical location is difficult such as upper cervical spine or as an additional adjunct to surgical management decreasing the size of the lesion or in recurring lesions.53,54,56
Langerhans cell histiocytosis
Langerhans cell histiocytosis (LCH) is a rare disease associated with the proliferation of Langerhans cells causing local or systemic effects. Although it can appear at any age, the peak incidence of LCH is in patients below 10–15 years of age, with males slightly more affected than females.57,58 The disease may be focal or systemic. LCH (former name: histiocytosis X) encompasses three syndromes that are considered to be clinical variations of the same disease: eosinophilic granuloma (EG; benign, isolated to bone), Hand–Schuller–Christian disease, and Letterer–Siwe disease.57,58 The etiology is unknown, but the abovementioned syndromes are histologically related. LCH lesions in children are mostly of the EG type, and approximately 90% are mono-ostotic bone lesions, with the spine involved in 6.5%–25% cases (Figure 5).57,58 Furthermore, these lesions are associated with the destruction of bone, replaced by Langerhans cells, eosinophils, and some neutrophils as well as macrophages. 57 EG of the spine is usually located in the vertebral body, with osteolytic appearance, leading to classic vertebra plana. Rarely, an adjacent paravertebral soft tissue mass may occur, and it can expand toward the posterior elements with a soft tissue mass. Azouz et al. 57 claimed that the thoracic spine is mostly involved, followed by the lumbar and cervical spine. Symptoms include local and radicular pain and, usually, mild neurologic deficits (e.g. difficulty in walking); however, in some cases, EG bone lesions can be asymptomatic. Imaging should begin with plain radiography (vertebra plana and anterior wedging); then, MRI and/or CT scans can reveal epidural soft-tissue extension.
Langerhans cell histiocytosis of cervico-thoracic junction in 4-year old boy. First symptoms: pain in whole spine and torticollis.
The main management of a single lesion (unifocal) vertebral EG is conservative treatment with biopsy, chemotherapy, and bracing, if necessary. Chemotherapy is indicated for polyostotic diseases. Mono-ostotic EG often shows spontaneous resolution, and recurrence is more rare in children than in adults. 59 Partial or almost complete height reconstitution of the vertebra is the usual healing pattern. 58 Surgery is rarely indicated for secondary deformities. 60
Spinal cord tumors
Spinal cord tumors are rare in children, accounting for less than 10% of pediatric central nervous system tumors, with a decreasing incidence over recent years. 61 The most common spinal cord tumors are intramedullary, although they can be found in the extradural compartment or as intradural extramedullary masses. 62 Neuronal or glial intradural intramedullary tumors can be derived from neuroepithelial tissues, including astrocytomas (60%), ependymomas, and developmental tumors. 62 Intradural extramedullary tumors mostly tend to be benign, although they can be meningeal or begin from distant sites, and include meningiomas and schwannomas. Spinal cord tumors most often present with pain followed by neurologic and spine deformities such as torticollis and kyphoscoliosis. Children with spinal cord tumors, in contrast to adults, frequently develop scoliosis before the onset of pain. 3
Spinal cord tumors require a multidisciplinary approach, and the treatment depends on tumor type; however, surgical resection by a pediatric neurosurgeon is usually indicated. A large percentage of emergent operations suggests poor early recognition of these tumors and highlights the need for more awareness of early symptoms to clinicians. 61 Typically, predictors of outcome include histological grading, extent of resection, and neurological status at the time of surgery.
Neurofibromatosis
Neurofibromatosis 1 (NF1) is the most frequent single-gene multisystem disorder with autosomal dominant inheritance.63 –65 It is caused by the mutation of Neurofibromin 1, a gene on chromosome 17 which is responsible for production of a neurofibromin.66,67 This is a disorder of neural crest cells, defined as “a spectrum of multifaceted diseases, probably of hamartomatous in origin, involving neuroectoderm, mesoderm, and endoderm.”65,68
Typical orthopedic manifestations include vertebral dysplasia, dystrophic and nondystrophic scoliosis, dural ectasia, tibial pseudoarthrosis, and increased risk of paraspinal tumors. Up to 70%–80% of dural ectasia is found in NF1 patients, and surrounding bones are “eroded by the expanding dura.” 69
NF1 causes tumors along the nervous system which can present as intraspinal or paraspinal tumors or in combination; they are noted in more than one-third of patients with NF1.68,70,71 They are isolated neurofibromas or plexiform neurofibromas (with the incidence of 25%–50%). 69 Plexiform neurofibromas may be followed by pain, neurologic deficits, and deformity of adjacent structures. 63 Initially benign paraspinal tumors may show a malignant transformation into malignant nerve sheet tumor and often require early detection based on surveillance to allow curative en bloc excision (Figures 6–8). 63 Therefore, regular MRI is obligatory; hence, it is the method of choice for measuring the neurofibromas and monitoring their growth. 66 Medical management using mitogen-activated protein kinases (MEK) inhibitors (selumetinib) is an option for the treatment of plexiform neurofibromas in children with NF1. 72
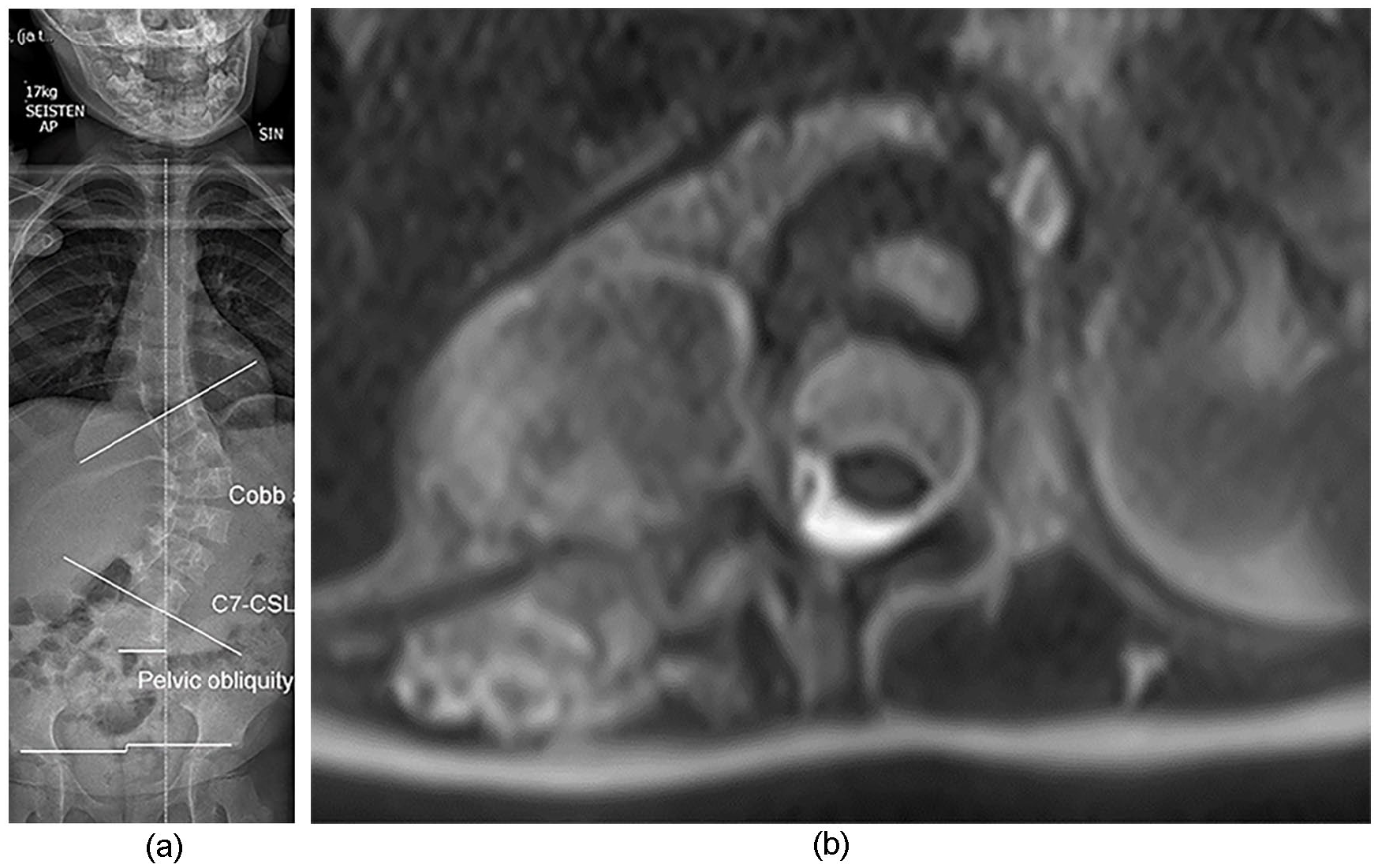
A 4-year-old girl with neurofibromatosis 1 associated early onset scoliosis. Preoperative spinal magnetic resonance image (T2 axial) shows a paraspinal tumor without features of malignancy according to biopsy.
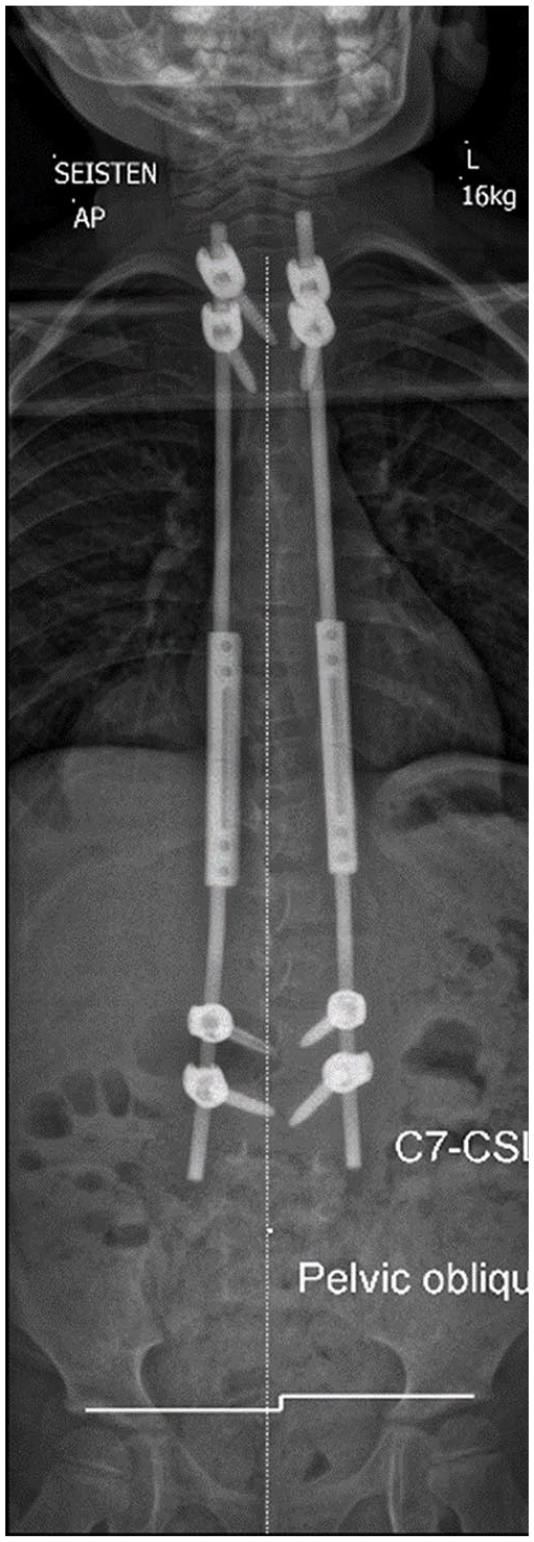
Postoperative standing radiograph after index surgery for Early Onset Scoliosis (EOS), which was carried using with traditional growing rods to allow tumor imaging and follow-up.
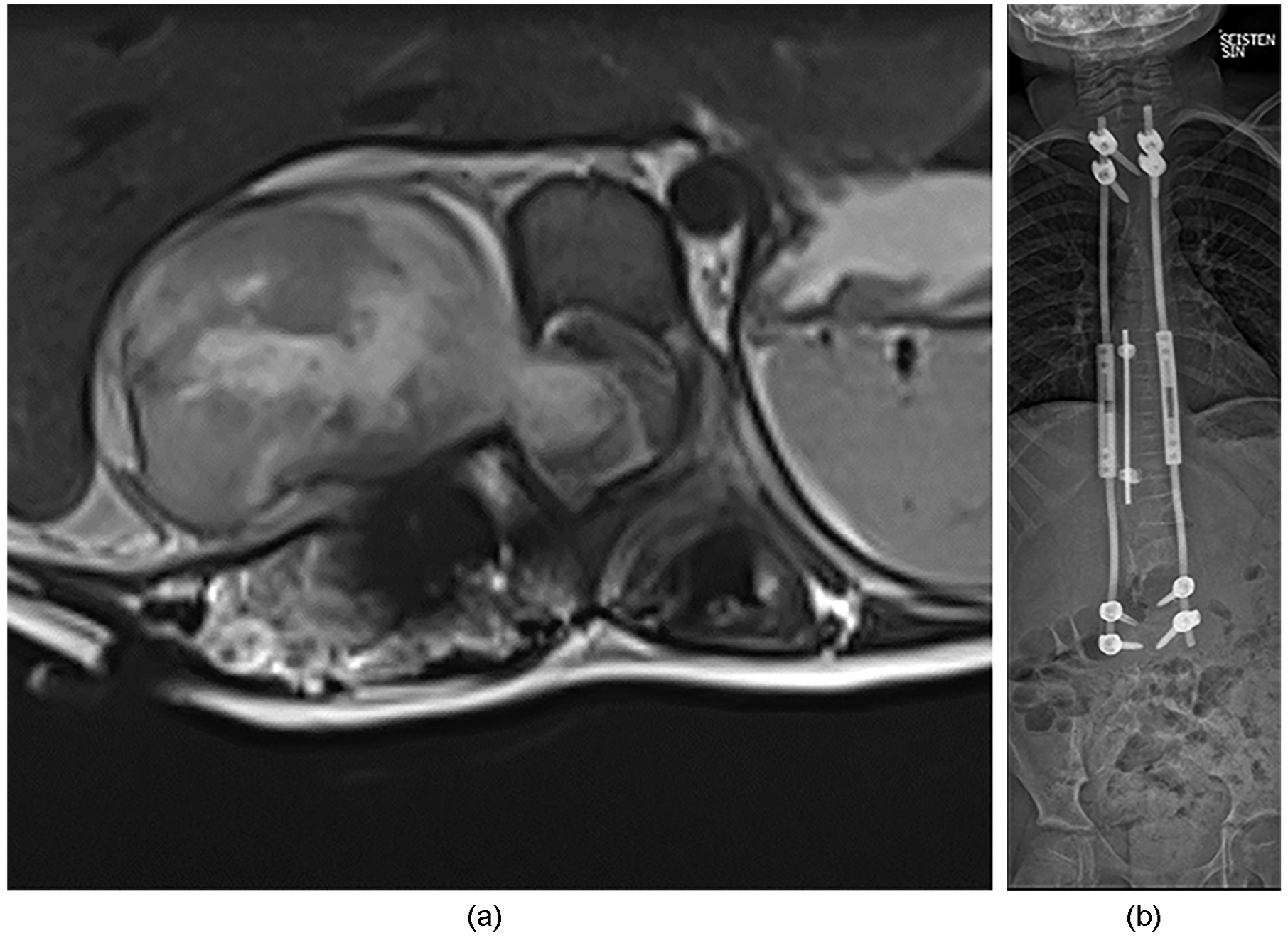
Transformation of an initially benign tumor into malignant nerve sheet tumor with intraspinal involvement (T2 axial). Tumor was excised with posterior laminectomy (nerve sheet excision and intradural tumor component removal) and a staged anterior tumor en bloc excision. Laminectomy area was instrumented with hook construct to prevent postlaminectomy kyphosis (3B).
Dystrophic scoliosis (short, stiff curve with increased kyphosis) with rib penciling, spindling of the transverse processes, vertebral scalloping, severe apical vertebral rotation, and adjacent neurofibromas usually does not respond to conservative treatment, and orthopedic surgery is usually necessary. 73 NF1 children with early onset scoliosis represent a special group as magnetically controlled growing rods may prevent tumor surveillance, and therefore, traditional growing rods are an option. 74
Infections of the spine
Infections of the growing spine are rare. Even if children are the second age group after elderly patients, only 2%–4% of musculoskeletal infections are in the spine area. 75 The peak of incidence of discitis is in patients below 5 years of age, whereas older children develop more vertebral osteomyelitis.76,77 There are several associated risk factors, including immunocompromised states, direct trauma with hematoma, hematogenous spread (skin, genitourinary tract, oral cavity, respiratory tract, and middle ear), and spine surgery (not included in the review). 78 Infections of the spine can be divided into pyogenic, granulomatous (specific and unspecific), fungal (Aspergillus spp. and Candida spp.), or parasitic (taenia solium and schistosoma).78,79
Pyogenic infections
The most common spinal infection is pyogenic, especially in industrialized countries. Pediatric spine infection can be described as infectious discitis or spondylodiscitis (SD), depending on the extent of the infection. Discitis (D) refers to an inflammation restricted to the disk, and the term SD is used when both disk and vertebral bodies are affected. 80
Bacterial infections spread to spine via three main routes: hematogenous, local extension, and direct inoculation. The most common is the hematogenous route (urinary tract infection, dental caries, and infected catheters). Local extension refers to the spread of the inflammatory process from adjacent soft tissue infection or paravertebral abscess (Figure 9). Direct inoculation occurs especially following spine surgery. Exceptionally, in infants, discitis and SD can be associated unwitnessed button battery ingestion.81 –84
A 17-year-old boy with pyogenic infection of L4 vertebra.
Owing to specific blood supply in childhood, an isolated disk infection may occur. Blood vessels and lymphatics can be detected in the annulus even up to 20 years of age, and cartilage end-plate blood vessels appeared up to 7 years of age (cartilage canals). These findings in addition to the occurrence of blood and lymphatic vessels in growing intervertebral disks help us to understand childhood discitis without a simultaneous effect on the vertebral body.85,86 Discitis and vertebral osteomyelitis seem to be two ends of the same disease spectrum. 77 In common practice, SD is often used to describe a continuum of spinal infections, from discitis to vertebral osteomyelitis. 87 Specific differentiation may be necessary for the selection of an appropriate therapy.
The age distribution is described as triphasic, with the first peak in the neonate period, second during preschool time, and the third in the second decade of life. 87 Another study divided childhood into two period with higher incidence of spinal infection: children below the age of 4 years and teenagers. 76 Children with discitis have an earlier disease onset than those with vertebral osteomyelitis. 77 Common risk factors for spinal infections are diabetes, renal failure, spinal surgery, immune compromise, and chronic steroid therapy. Regarding sex prevalence, males are more often involved than females. 82
Two pathogenesis underlie the spread of bacteria from a distant focus to the spine. In the first pathogenesis, the disk is primarily involved, followed by adjacent vertebral end plates and bodies. This mechanism is possible in younger children due to specific vascularization of the disk space. In the second pathogenesis, the bacteria settle in vertebral bodies first and then produce osteomyelitis, involving the disk in the next phase.85 –87 This pathogenesis occurs usually in older children and adolescents, when the subchondral bone is supplied by end arteries. A small bacterial embolus may stop there and begin to proliferate, with subsequent vertebral osteomyelitis. From here, the infection may spread through the end plate into the disk. 87
Pyogenic bacterial infections almost always involve the disk; nowadays, most authors state that pure discitis does not exist due to vascular anatomy. All bacterial infections are probably primarily located in the metaphyseal region of the vertebral body. According to this theory, bacteria go through the cartilaginous vertebral plate via adjacent vertebral metaphysis and finally reach the disk space. 87 Wenger claimed that bacterial spinal infections in children begin in the form of microabscesses in the vertebral body near the end plate. 88 Afterward, the infection spreads from the end plate to the disk through the perforating vascular channels and extends to the paravertebral area and epidural space.78,89,90
Etiology
Identifying the causative pathogen of SD in the pediatric population is difficult (Table 2). Moreover, cultures from blood and vertebral aspiration can show false-negative results.
Infections of the pediatric spine and etiologic agents (modified from Principi and Esposito). 87
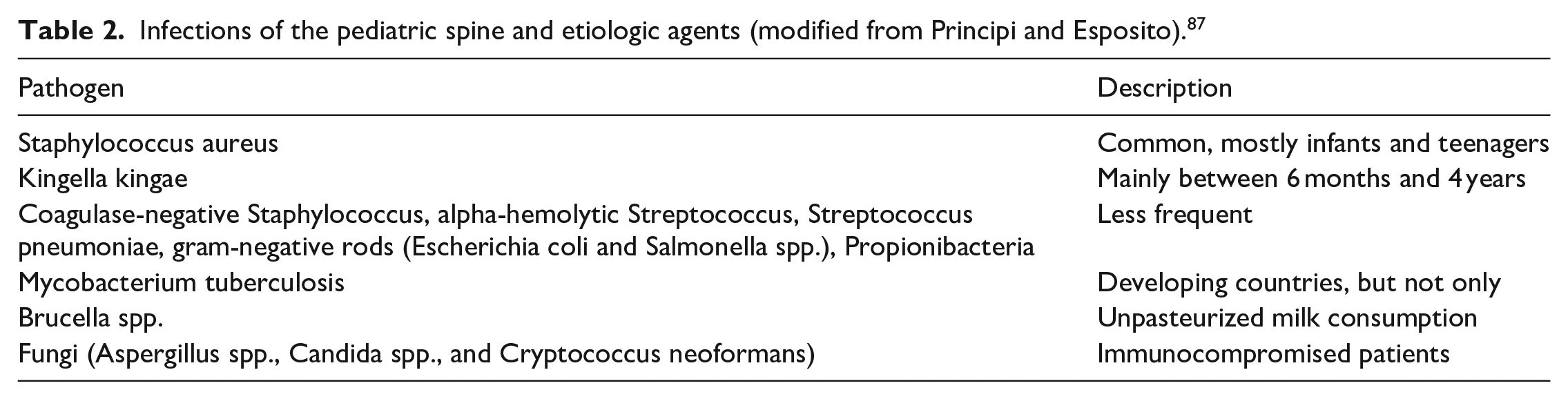
Staphylococcus aureus is the most common pathogen; it has been identified in more than 50% of cases. Some studies suggest an incidence of approximately 80%, especially in the juvenile and adolescent groups.82,87 Other pathogens detected in SD cases are various gram-positive and gram-negative bacteria (rods such as Escherichia coli and Salmonella).75,77 Kingella kingae is the main pathogen of the condition in children below 4 years of age.75,82,87 It is a gram-negative organism, and it is difficult to detect in different samples of bodily fluids.87,91 In this age group, the traditional culture is frequently negative, but some studies found throat swabs positive with Kingella kingae.87,92
Symptoms and diagnosis
Discitis is most common in children aged 1–5 years. The symptoms may occur gradually over a few weeks, thereby delaying diagnosis. The typical symptoms include mild fever, irritability, local tenderness, chronic back and leg pain, abdominal pain, back pain and inability or failure to walk, limping, and Gower’s sign.77,78,80,93 –95 Back pain is present in almost all cases of SD, usually localized near the infected segment, although it may radiate. 79 Back pain worsens at more than weeks to months; however, acute and chronic forma are also possible. The pain increases overnight and during physical activity. 79
During clinical examination, typical findings included stiffness and restricted movement of the affected spinal segments and need for support when standing up or bending over. Local pain during percussion occurs in some cases. 80
Although discitis may resolve spontaneously, the theory of avoiding antibiotic therapy remains controversial. The most severe form of SD occurs in young children below 6 months of age, and it is associated with multiple foci of infection and septicemia. Severe local vertebral damage and destruction occurs, followed by pathologic kyphosis in the thoracic spine. 78
SD may be accompanied by neurologic symptoms, ranging from subtle to radicular or intraspinal pressure, depending on the extent of the inflammatory process. Epidural abscess is one of the most common cause of significant neurologic deficits (4%–38% of SD cases).82,96 Typical symptoms include the triad of fever, excruciating pain, and rapid progression of neurological symptoms. 78
Typically, in SD, the primary site of involvement is the L3–L4 and L4–L5 interspaces. Primarily, radiographs may be normal, with disk space narrowing occurs first, although after 2–4 weeks. Typical radiographic findings are disk space narrowing and erosion of adjacent vertebral end plates. 77
Estimation of white blood cell (WBC) count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) yields only nonspecific information, with normal WBC counts and elevated inflammatory marker usually.96 –99 Although nonspecific, ESR and CRP with their sensitivity from 94% to 100% are very important tests.78,100,101
Bone scans are useful in localizing the pathology; however, the results should be confirmed by additional imaging. MRI is a good diagnostic tool in early and late sequelae. First, we can observe the narrowing of the intervertebral space and swelling of the annulus (hyperintense in T2, contrast enhancement), which progresses up to irregularity of end plates and brightness of whole vertebra (T2 image). In addition, epidural abscesses are easily visible in MRI, with high sensitivity (up to 90%). In these cases, the epidural space of intermediate intensity (in T1 and T2—images) is observable with homogeneous enhancement using the gadolinium. Pus filling the center of the lesion is nonenhancing in magnetic resonance (MR) images. 78 Such abscess may extend along two to four vertebral bodies.
Invasive diagnostic procedures such as needle aspiration and biopsy can reveal bacteriological etiology.34,49 However, bacterial growth can be determined in 40% of the cases using biopsy.102,103 Therefore, CT-guided biopsy is recommended only when initial blood cultures are negative. 96
Treatment
Childhood SD is often a benign, self-limiting condition with antibiotics and the likelihood for bone destruction is low. 80 Therefore, conservative treatment is usually sufficient. Nonoperative treatment includes bedrest, immobilization, and antibiotics typically for 4–6 weeks.79,80,97 Recommendations regarding the duration of treatment vary. However, the most common schedule consists of 7–10 days of parenteral antibiotics followed by oral antibiotic for 2–3 weeks. 80 The extent and duration of immobilization are another consideration: bed rest, plaster cast, and brace of duration from weeks to months. Treatment can be stopped when pain ceases, passive spinal mobility is unrestricted, and CRP and ESR are normalized. 80
Indications for surgery include paraspinal abscess in the presence or progression of neurological deficits and limited responsiveness to nonoperative treatment. Basic operative treatment consists of surgical debridement followed by antibiotic treatment. Epidural abscess are located behind the vertebral body; therefore, posterior approach, laminectomy, evacuation of the pus, and spinal instrumentation are sufficient for decompression and prevention of postlaminectomy deformities. 78
The typical outcome is favorable, with the child asymptomatic child and free of pain. Late radiographic changes include fibrous or bony ankylosis of the affected spinal segments. Kaiser observed such changes in 65% of cases; however, only 16% presented with restricted movement of the spine. 80
Tuberculosis
Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis. Skeletal involvement can be observed in approximately 10% of patients with extra pulmonary tuberculosis. Spinal tuberculosis (ST) is a frequently observed form, occurring in up to 50% of skeletal tuberculosis cases, especially in developing countries.
Pediatric ST is characterized by rapid bone destruction and associated with the risk of rapid-onset neurological deficits and severe deformity of the spine. The behavior of the spinal deformities over time is affected by the growth of spine. 104 As a child grows, pathologic kyphosis may increase leading to spinal canal stenosis and myelopathy.
Symptoms and diagnosis
The main, but noncharacteristic, ST symptoms include pain and signs of chronic infection (but also malaise, loss of weight and appetite, and night sweats).89,105 Torticollis, neck guarding, respiratory distress, and difficulty in swallowing suggest involvement of the cervical spine. 106
Severe neurologic deficits are rare among children, whereas the disease may be more aggressive in adults, with developing large abscesses. The thoracolumbar region is often the most affected; however, there are rare cases of ST in the cervical spine or multifocal noncontiguous spinal lesions. 106
Garg clearly described the mechanisms of neurological deficits in ST, categorizing them into early onset and late-onset paraplegia. Early onset paraplegia may have several causes, as presented in Table 1, whereas late-onset paraplegia is caused by either transection of the spinal cord by bony bridge (severe kyphosis) or fibrosis of the dura (pachymeningitis). 105
ST creates three main problems: cold abscesses (collection of purulence from infected vertebra), neurological deficits, and kyphotic deformity of the spine due to bone destruction. 107 In the pediatric population, up to 50% of patients presented neurological deficit and 62% with paraspinal abscesses.78,108
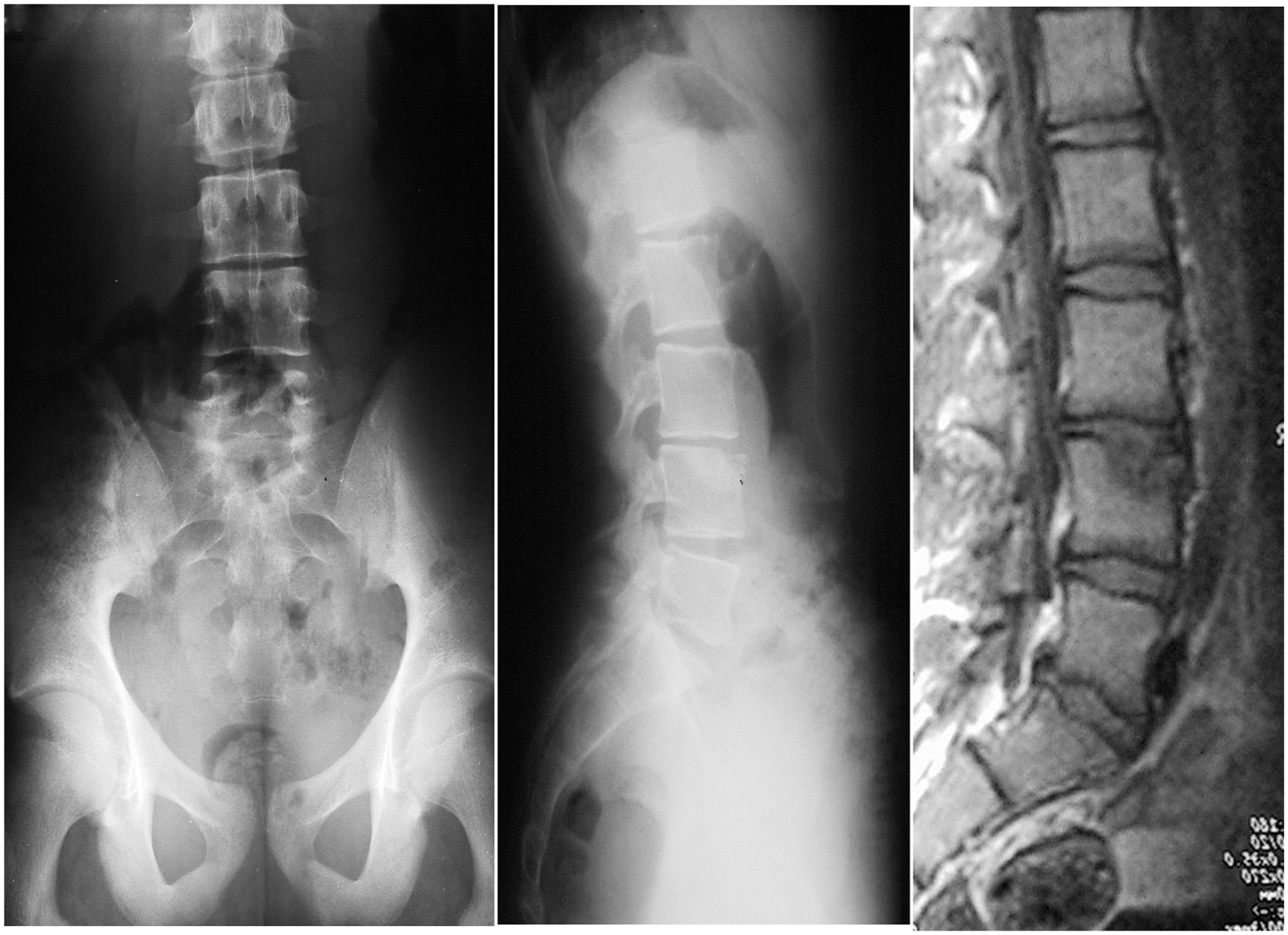
Imaging should begin with plain antero-posterior (AP) and lateral spine radiography (Figure 10). In the active phase of disease, a characteristic loss of bone density in the anterior spine with lytic lesions of vertebral body and soft tissue shadows in the paraspinal region can be observed, suggesting cold abscesses. 89 However, radiographs may show normal results in the very early stages of the disease.

Tuberculosis of thoracic spine in a 5-year-old girl (spondylodiscitis 11th/12th).
Further imaging modalities should include MRI and CT. Both tools can detect bony destruction earlier than plain radiography. MRI is more sensitive than radiography and more specific than CT; it can reveal involvement of the vertebral bodies, disk destruction, cold abscess, and spinal deformities. 105
Tissue diagnosis is the gold standard diagnostic test for ST. Tissue samples could be obtained by CT-guided needle biopsy or surgical biopsy. 107 All samples should be routinely sent for culturing and histopathology. In addition, polymerase chain reaction is a useful tool for bacteriological diagnosis of tuberculosis. 105
Treatment
Appropriate pharmacological treatment is obligatory. Nonoperative treatment may include various spinal orthoses for pain control and prevention of deformity.
Indications for surgery include neurologic deficit (worsening and acute severe paraplegia), spinal instability with or without subluxation or dislocation, kyphosis (progressive, >60°, more than three vertebral bodies affected), late-onset paraplegia, and advanced disease unresponsive to nonoperative treatment. Early operative treatment in ST with neurologic deficits in currently being discussed; recommendation for surgery varies from surgery only for complete paraplegia to surgery in all neurologic deficits.105,107,109 Regarding kyphotic deformity, the orthopedists are more unanimous; this problem is very important as a late sequela of ST and a crucial component of the natural history of ST, especially in the growing spine.107,110 Neurologic deficits associated with kyphotic deformity can be slowly increasing (due to gradual spinal cord compression) or rapidly occurring (deformity leading to an instability episode). A special group of patients are children with “spine-at-risk” signs, with risk of deformity progression and neurologic failure during the growth period.
Surgery can be performed in either the active or healed phase. Nowadays, surgical indications are restricted to cases with unconfirmed diagnosis requiring open surgical biopsy, gross motor deficits (less than two out of five muscle strength), or rapidly evolving neurologic deficits at presentation. Other indications include deformity progression or instability, deficits refractory to 3 to 4 weeks of appropriate chemotherapy. 107
Generally, there are two main groups of surgical procedures: (1) debridement with the release of neural structures, and (2) debridement and spinal stabilization (with bone grafts and implants).109,111 –113 A third kind of surgery concerns progressive kyphotic deformities in the healed phase. 114 These procedures are difficult to perform, with high risk of complications. With the development of different spinal osteotomies, a three-column osteotomy from the posterior-only approach was sufficient in the correction of post-tuberculosis kyphosis.109,115
Conclusion
Spinal tumors and infections should both be considered as potential diagnoses in patients with spinal pain unrelated to activity, accompanied by fever, malaise, and weight loss. In spinal tumors, early diagnosis, timely adequate multidisciplinary management, appropriate en bloc resection, and reconstruction improve local control, survival, and quality of life. Pyogenic, hematogenous SD represents the most common spinal infection; however, tuberculosis-induced SD should also be considered. Importantly, the unique features of the growing spine make diagnosis and treatment of infections and tumors challenging.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231215857 – Supplemental material for Tumors and infections of the growing spine
Supplemental material, sj-pdf-1-cho-10.1177_18632521231215857 for Tumors and infections of the growing spine by Barbara Jasiewicz and Ilkka Helenius in Journal of Children’s Orthopaedics
Footnotes
Authors’ contribution
BJ and IH contributed equally to the writing and reviewing of the article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I.H. reports grants from State funding via Helsinki University Hospital, grants from State funding via Turku University Hospital, during the conduct of the study, grants from Medtronic, grants from Nuvasive, grants from University of Helsinki, Research Funding for Injuries, personal fees from Globus, outside the submitted work. B.J. has nothing to disclose.
Ethical statement
Institutions of both authors do not require ethical approval for article being an expert opinion.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I.H. has received funding from Finnish government (Helsinki and Turku University Hospitals), Medtronic (ERP-2022-13237).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.