
Abstract
Background
We employed a novel curettage tool, a bent needle tip, during irrigation for enchondroma of the distal phalanx. This study aimed to evaluate our new curettage tool for treating enchondroma of the distal phalanx.
Methods
Seven distal phalanx enchondromas were pathologically diagnosed at our institute. We evaluated age, gender, tumor location, affected side, clinical symptoms, Takigawa classification, size, recurrence, complications, residual pain, Tordai score, and follow-up period. We bent an 18G needle tip connected to an extension tube and syringe. The bent needle was inserted through the small hole, and the cavity for bone grafting was adequately filled with injectable calcium phosphate cement through the small hole.
Results
There were five centric-type and two giant-type tumors, with a mean size of 52.7%. All patients had clinical symptoms at the initial presentation. All patients showed complete bone healing within 3 months on post-radiological examinations and were Grade 1 according to the Tordai score.
Conclusions
This tool is extremely simple, and both the incision and the cortical window can be small. We recommend a bent needle tip, easily devised in any hospital, as a curettage tool for treating enchondroma in small bones, especially of the distal phalanx.
Keywords
Background
Enchondroma is a benign bone tumor that frequently arises in the tubular bones of the hands as well as in the proximal phalanx, and less commonly in the middle phalanx and metacarpals. 1 However, enchondromas of the distal phalanx in the hands and feet are rare.2,3 Surgical treatment of enchondromas is recommended mainly to alleviate pain or pathological fractures, including impending fractures. The standard surgical method is complete tumor removal, which is achieved by firmly opening a cortical window followed by full curettage of the cavity using a curette, and finally irrigating the cavity. 1 However, the distal phalanx is a very small bone and has attachments to the flexor and extensor tendons (Figure 1). Enchondroma of the distal phalanx usually occupies the majority of the distal phalanx and arises from the proximal side of the distal phalanx. The conventional method of curettage of the distal phalanx through a cortical window has a risk of iatrogenic postoperative fractures and avulsion of the flexor digitorum profundus (FDP). 4 However, it is necessary that enchondroma of the distal phalanx should be treated not only through a small cortical window but also with full curettage.

Anatomy of the distal phalanx. The distal phalanx is a very small bone, and the proximal site of the distal phalanx has flexor and extensor tendon attachments.
There are various curette sizes for small bones depending on the tumor size, and the size of the cortical window depends on the size of the curette or working space needed to achieve full curettage. The curettes are usually made of solid metal and lack flexibility. Moreover, every type of small curette is not always available. Hence, we were looking for a new tool with fewer procedure-related complications that is easy to use. E.O. designed a new tool using a needle tip to be bent as a curettage tool (Figure 2). This tool is simple to devise, easy to use, flexible, and can be made in virtually any hospital. Besides, curettage can be achieved while performing irrigation via the needle connected to a syringe. The aim of this study was to evaluate the effectiveness of the bent needle tip as a curettage tool for treating enchondroma of the distal phalanx.

A new curettage tool. Needle tip views; (a) frontal view, (b) lateral view, (c) oblique view, (d) overview of the curettage tool. An 18G needle tip was bent and then connected to an extension tube and a 50-mL syringe filled with saline, (e) saline in the tube is used for washing the cavity.
Materials and methods
Patients population
We performed a retrospective review using prospectively collected data from 37 consecutive patients who underwent surgical treatment of enchondromas in the hands at our institute between January 2014 to December 2016. Avulsion of the flexor digitorum superficialis, non-operative, and recurrent cases treated with another method were all excluded. We obtained informed consent to participate in this study from all patients and the study protocol was approved by the Nihon University Hospital’s Joint Institutional Review Board (RK-180612-12). We evaluated age at diagnosis, gender, tumor location, affected side, clinical symptoms, Takigawa classification, 5 tumor size, perioperative complications, residual pain, Tordai score, tumor recurrence, and follow-up period. Takigawa et al. reported the radiographic classification of enchondroma as encompassing central, eccentric, combined, polycentric, and giant types. 5 The size of an enchondroma was calculated from the frontal view of a plain radiograph as the percentage of the longitudinal axis of the distal phalanx that occupied the lytic area of the enchondroma (Figure 3). Residual pain was evaluated by visual analog scale (VAS). Patients were radiographically evaluated and recurrences were assessed according to the classification system employing the Tordai score. 6 Grade 1 indicates bones with a normal cortex and spongiosa or a bone defect smaller than 3 mm in diameter. Grade 2 indicates bone defects 4 to 10 mm in diameter but with no clear recurrence. Grade 3 represents bone defects larger than 10 mm with the characteristics of an enchondroma. 6 We also evaluated bone union rate. We radiographically defined bone union as no gap between cancellous bone and calcium phosphate cement for bone graft. Nonunion was diagnosed on plain radiographs when the bone graft was absorbed 3 months after surgery. Postoperative follow-up was performed at 1, 2, 3, 4, and 6 weeks, and every 3 months thereafter.

The size of an enchondroma was calculated from the frontal view of a plain radiograph as the percentage of the longitudinal axis of the distal phalanx that occupied the lytic area of the enchondroma.
Surgical technique
Surgery was performed under general anesthesia with a tourniquet. Fluoroscopic imaging was used to confirm the curettage area during the operation. An 18G (outside diameter: 1.25±0.02 mm) needle tip (TERUMO NEEDLE, TERUMO Corporation, Japan) was bent (Figure 2a–c), and then connected to an extension tube and a 50-mL syringe filled with saline (Figure 2d). An incision was made on either the radial or the ulnar side, selected based on the thinnest side of the distal phalanx. A small hole was made in the cortex using a 2.0 K-wire (Figure 4). The bent needle was inserted through the small hole, and the tumor area was fully curettaged while saline washing was performed via the connected syringe (Figure 2e). The needle tip is flexible and can be bent at any angle while performing irrigation and pressuring saline into the tumor cavity, so we could easily remove the entire lesion of the tumor with this tool. After curettage, residual saline and fragmented tumor tissues were aspirated through the end of the extension tube connected to the bent needle. We confirmed whether the tumor was fully curettaged by using a contrast agent. Finally, the cavity for bone grafting was adequately filled with injectable calcium phosphate cement (BIOPEX®-R, HOYA Technosurgical Corporation, Japan) through the small hole (Figure 5). The finger was immobilized with a splint for 1 to 2 weeks depending on the patient’s VAS pain level. The patient was encouraged to gently mobilize the finger postoperatively.
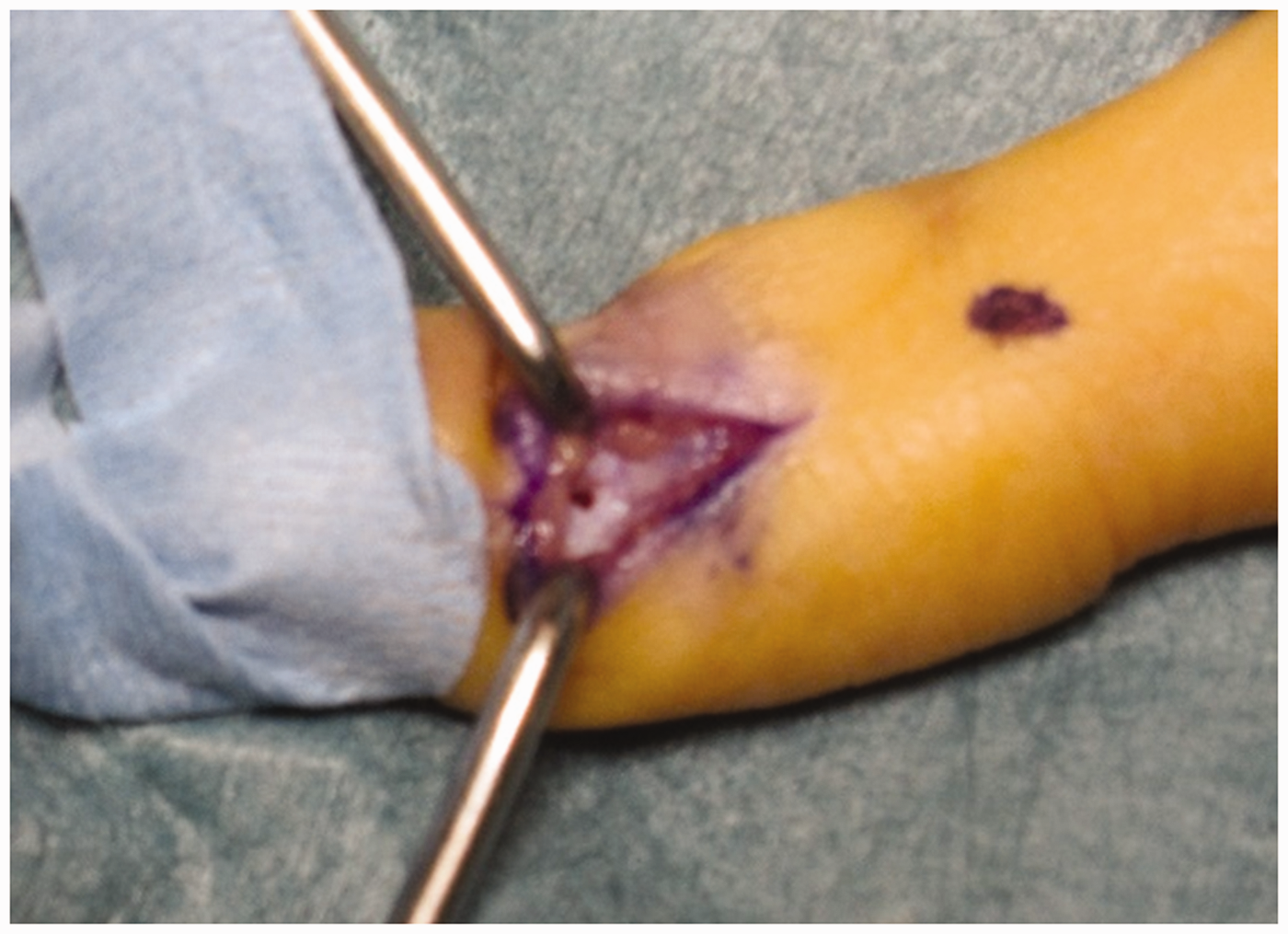
Intraoperative findings. A small hole is made in the cortex with 2.0 K-wire. A bent needle is then inserted through the small hole.

(a) Pre-operative radiographic images. (b) Post-operative radiographic images. After full curettage, the cavity is adequately filled with injectable calcium phosphate cement for bone grafting.
Results
Of the 37 patients reviewed, seven enchondromas of the distal phalanx were pathologically diagnosed and included in this study. There were five women and two men with a mean age of 41 (range, 32–51) years (Table 1). The average follow-up was 18.0 (range, 6–30) months. There were two index, one middle, two ring, and two little finger tumors, with locations in the left hand in four cases, and the right hand in three cases. All tumors were located at the proximal side of the distal phalanx. There were five centric-type and two giant-type enchondromas according to the Takigawa classification, with a mean size of 52.7% (range, 34.5–72.3). All patients had clinical symptoms at the initial presentation, such as swelling, pain with/without pathological fracture, and/or nail deformity. Three patients with pathological fractures were treated after bone healing. All patients showed complete bone healing on plain radiographs within 3 months after surgery. There were no perioperative complications such as infection or range of motion limitations. There were no recurrences, and all cases were regarded as Grade 1 according to the Tordai score system at the final follow-up. Although two patients complained of residual pain, it did not affect their daily living.
Demographic data.

*Percentage of the longitudinal axis of the phalanx that was occupied by enchondroma.
Discussion
Enchondroma is a common benign hyaline cartilage lesion of bone that frequently arises in the tubular bones of the hands. They are the most common tumor of the small bones of both hands. However, enchondromas of the distal phalanx are rare, accounting for 4% to 18% of those in the hand.2,3,5,7–9 These tumors are usually found incidentally with not only pain, swelling, and pathological fracture but also clubbing of the affected finger and nail deformity. 10 Surgical treatment of enchondromas in the distal phalanx is considered to be indicated mainly in the presence of pain or pathological fracture or impending fracture. 9
The standard surgical treatment is complete tumor removal. However, surgical treatment of enchondroma in the distal phalanx is controversial in terms of the surgical approach, curettage tools, and the necessity for post-curettage void augmentations. Because the distal phalanx is a very small bone and the medullary cavity is also small, there might be attachments to the flexor and extensor tendons despite the minimal size of the affected bone (Figure 1).
Enchondromas of the distal phalanx have been surgically treated through dorsal, palmar, fish mouth, and mid-lateral approaches.1,11 The dorsal approach is not currently recommended because of injury primarily to the terminal extensor tendon and the nail apparatus. The palmar incision entails full exposure, but has the drawback of often leading to a persistent painful scar. The fish mouth incision allows incomplete curettage based on the long distance to the tumor location, such as with the eccentric type. Making a smaller mid-lateral incision has gained popularity owing to the low risk of damaging the tendon and nail. However, care must be taken to avoid disrupting fingertip sensation. For these reasons, we recommend treating the distal phalanx using a mid-lateral incision, which can be made small by creating a small cortical window, and a mid-lateral incision on either the radial or ulnar side was selected for our cases based on the thinnest side of the distal phalanx.
Curettage for enchondroma of the distal phalanx needs to be treated through a small cortical window. However, there has been no tool with an appropriate size and flexibility for curettage of the distal phalanx. To overcome this problem, we used a bent needle tip as a curettage tool (Figure 2a–c). This tool is simple to devise, easy to use regardless of the tumor size, is flexible at any angle, and can be made in virtually any hospital. In addition, curettage can be achieved more easily while performing irrigation via the needle connected to a syringe and pressuring saline into the tumor cavity (Figure 2d,e). Furthermore, if necessary, we can add surgical adjuncts, such as phenol, dehydrated alcohol, and polymethyl methacrylate cement, via the small cortical window.
Optimal management of the post-curettage cavity including the distal phalanx remains uncertain. 1 Some authors reported that post-curettage bone grafting was not always necessary.12,13 However, the others recommended a bone graft for enchondroma in the distal phalanx.10,14,15 They insisted that bone grafting facilitated early exercises and functional recovery for cases with large osseous defects or pathological fractures. Our result showed that tumors had a mean size of 52.7% and were located at proximal sites in the distal phalanx with attachments to the flexor and extensor tendons. Thus, we also recommend that bone grafting for enchondroma in the distal phalanx should be added, allowing early exercises and avoidance of post-operative fractures. Moreover, injectable calcium phosphate cement should be used because the cortical window is small.
There were several limitations of this study. First, the number of surgical procedures was small because enchondromas of the distal phalanx of the hands are rare. However, our results showed not only complete bone healing and no perioperative complications but also the strong possibility of the usefulness of this surgical method. Second, the study design was retrospective without a control group, such as a conventional surgical group or a group treated with other curettage tools. Although there were no recurrences among our cases, it is possible that curettage might be incomplete because we could not directly check whether or not complete curettage was performed. However, we confirmed complete curettage by using a contrast agent. For this reason, prospective studies with a cohort or clinical trial design are needed. Third, our follow-up period was short. Some patients experience enchondroma recurrence more than 10 years after the operation. 16 This risk and the possibility of local recurrence necessitates meticulous follow-up observation.
Conclusion
We evaluated the effectiveness of the bent needle tip as a curettage tool for treating enchondroma of the distal phalanx. All patients showed complete bone healing on plain radiographs within 3 months after surgery. There were no perioperative complications including infection or range of motion limitations. This surgical method is extremely simple, and both the incision and the cortical window can be small. The bent needle tip as a curettage tool is simple to devise, easy to use without depending on the tumor size, flexible at any angle, and can be made in virtually any hospital. Additionally, curettage can be achieved more easily while performing irrigation via the needle connected to a syringe and pressuring saline into the tumor cavity. We recommend this curettage tool for treatment of enchondromas in small bones, especially of the distal phalanx.
List of abbreviations
FDP: flexor digitorum profundus; VAS: visual analog scale
Footnotes
Acknowledgements
We acknowledge our staff of the Orthopaedic department in our University Hospital.
Availability of data and materials
All data used and analyzed during this study are available from the corresponding author on reasonable request.
Authors’ contributions
EO performed study design, data collection, analysis, and preparation of the manuscript. HU performed study design, decision to publish, and preparation of the manuscript. TK performed data collection and preparation of the manuscript. YY performed data collection, analysis, and preparation of the manuscript.
Ethics approval
IRB approval in Nihon University Itabashi Hospital: RK-180612-12.
Consent for publication
All individual persons consented to publish their data.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.