
Abstract
Colonic lipomas are the second most common benign tumor of the colon. During a systematic literature search, a lack of review is observed. This study reports two cases of colonic lipomas and also tries to review the clinical and pathologic features of the reported symptomatic lipomas.
Keywords
Introduction
Lipomas are benign tumors arising from deposits of adipose connective tissue being detected from skin, adrenal glands, parapharyngeal space, breast, mediastinum and pleura, heart and vessels, brain, and intraspinal areas to gastrointestinal tract (GIS). Lipomas of the GIS are rare conditions and were first described by Bauer in 1757. 1 The colon is the most frequently involved segment of the GIS, accounting for 65%–75% of lipomas. 1 In fact, lipomas are the second most common benign tumor of the colon, after the adenomatous polyp. 2 In most cases, colonic lipomas (CLs) are mildly symptomatic. The aim of this study is to present two new cases of CLs and also to review the literature in order to determine the clinical features, pathological findings, and management of these lesions.
Case series
Case 1
A 29-year-old woman complained for alternative changes of diarrhea and constipation as well as abdominal pain and hematochezia. Coloscopy and computed tomography (CT) revealed a 5.0 × 2.5 × 5.0 cm tumor located in the sigmoid colon. Sigmoidectomy was performed and a submucosal pedunculated lipoma was excised. The patient is well 2.5 years after surgery (Figure 1(a)–(c)).
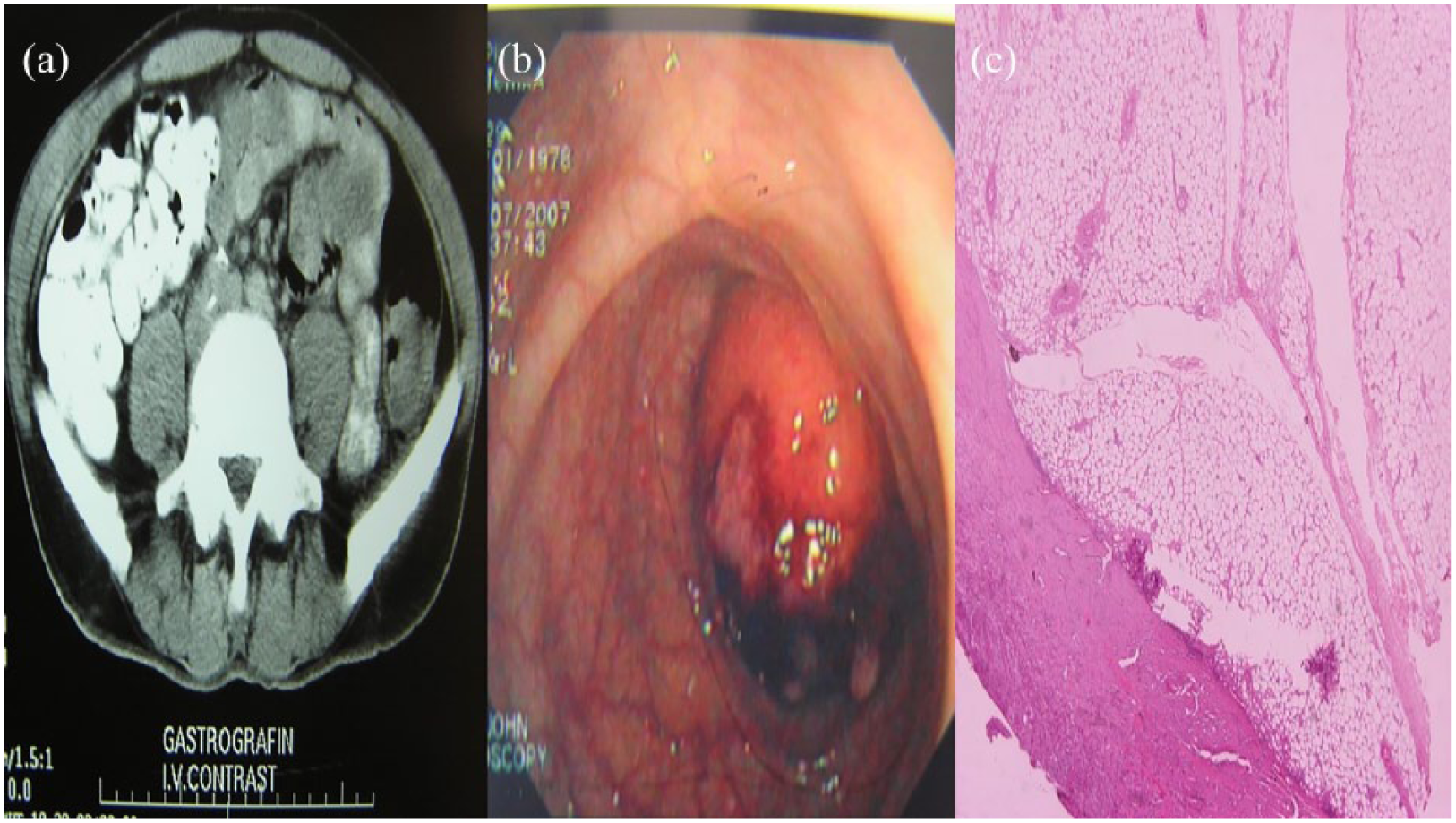
(a) CT of the abdomen, (b) image from the lipoma during endoscopy, and (c) pathology image from the lipoma.
Case 2
A 61-year-old male patient was admitted to our clinic with abnormal bowel disorders, bleeding per rectum, and abdominal pain. Physical examination was unremarkable. However, the performed diagnostic modalities revealed the presence of multiple lesions of sigmoid colon. Endoscopic removal was performed. Two submucosal pedunculated lipomas were excised, one of 3.3 × 3.2 × 2.5 cm and the other of 4.5 × 3 × 2.6 cm; 6 months upon follow-up, the patient is free of symptoms (Figure 2(a)–(c)).
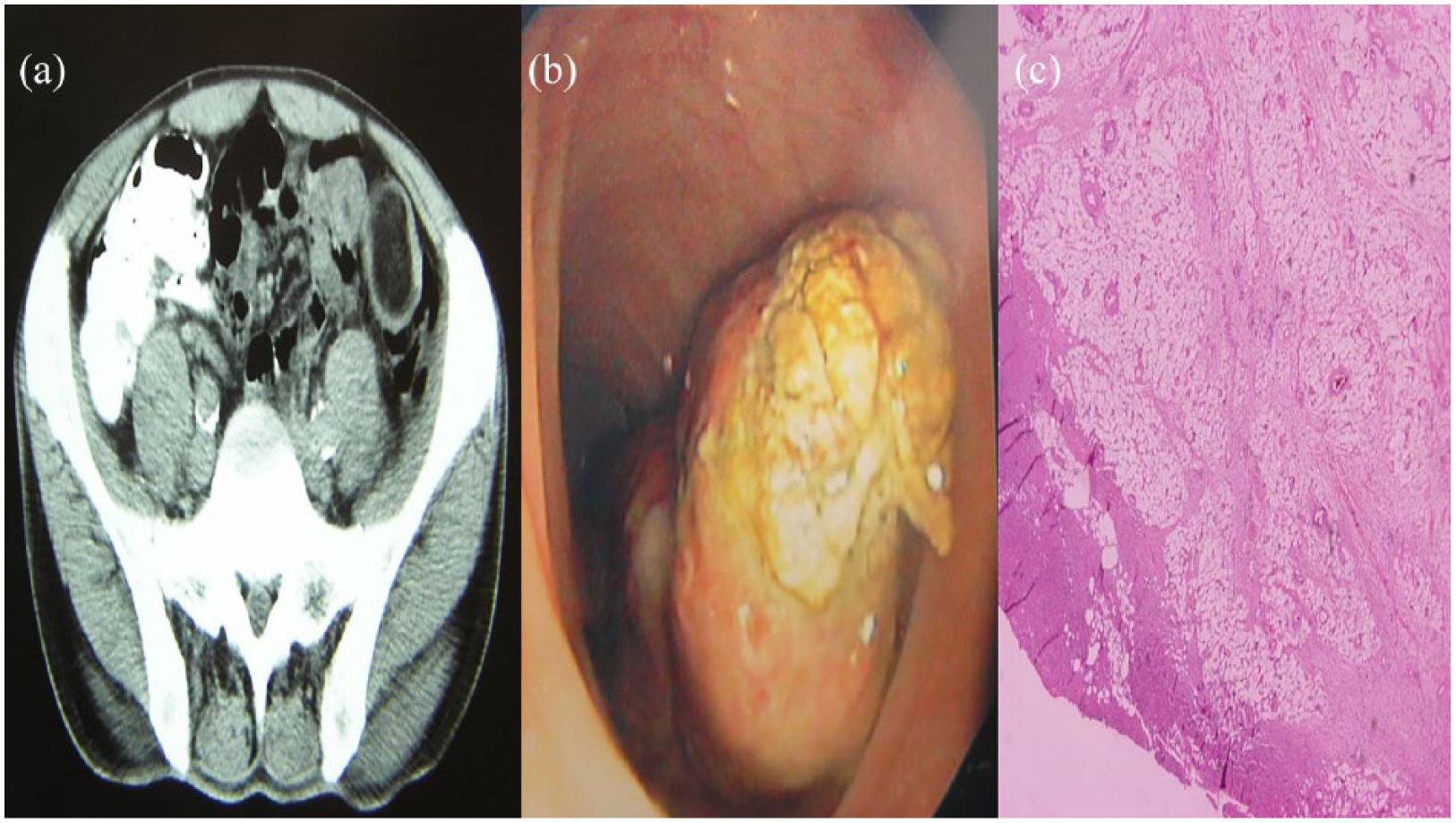
(a) CT of the abdomen, (b) image from the lipoma during endoscopy, and (c) pathology image from the lipoma.
Discussion
Searching the international literature from 1757 when Bauer reported one of the first known symptomatic colonic lipoma (SCL) to 2014, 115 articles describing 210 cases of SCLs were found. We decided to limit our report from 2000 to 2014, since more data were available and recently updated. A further exclusion was necessary due to the inability to obtain full text for some articles. This led to the review finally of seven cases (Table 1).
PRISMA flowchart.


CLs are rare, benign, non-epithelial neoplasms with an incidence ranging from 0.035% to 4.4% in relation to all polypoid lesions of large intestine. However, they are the most common tumors of mesenchymal origin of the GIS. Based on our review, SCLs usually occur in patients from 27 to 84 years old with the mean age of 59.3 years. Men (51.2%) and women (48.8%) are affected equally, with a male:female ratio of 1.04.
Clinical manifestations are associated with the size of tumor and not with the involved segment of the bowel. 1 Mean size of the reported SCLs was 5.09 cm with a range from 0.35 to 10 cm. As widely accepted, lipomas larger than 2 cm in diameter are likely to be symptomatic. 1 However, Goasguen and Zhang describe SCLs in ascending colon measuring 0.35 and 0.45 cm, respectively, in patients complaining for abdominal pain. SCLs are more commonly observed in transverse colon (25%). Sigmoid colon and cecum are the second location to be found (20.2% each).
Symptoms are generally nonspecific and have long duration. 3 The majority of the patients present with abdominal pain, which is described as diffuse, intermittent, crampy, or acute. There are some cases referring to nausea and vomiting and others to anemia due to chronic bleeding. Emergency due to the complications of colon lipoma can also occur. 4 Rectal bleeding accounts for the most cases of emergency followed by obstruction, which includes intussusception as well. Since SCLs have no specific symptoms and physical signs, accurate preoperative diagnosis cannot be achieved. Various imaging modalities can imply the diagnosis. Barium enema may reveal an ovoid filling defect with well-defined margins. The squeeze sign is frequently noted. This indicates a change in size and shape of a radiolucent lesion in response to bowels’ peristalsis. Endoscopically, lipomas are seen as smooth, round, yellowish polyps with a thick stalk or broad-based attachment. Typical colonoscopic features are the “cushion sign” or “pillow sign” (pressing forceps against the lesion results in depression or pillowing of the mass) and the naked fat sign (extrusion of yellowish fat at biopsy site). 5 Although the mucosa overlying a CL is usually not involved, in rare cases, colonoscopy may reveal ulcerations and stiffness on palpation that may lead to a mistaken impression of carcinoma. However, biopsy is not usually recommended in patients with suspected lipoma. Since the lesion is beneath the normal mucosa, biopsy cannot often promote diagnosis, whereas it increases the risks of bleeding and perforation. 1 Endoscopic ultasonography (EUS) can be used to discriminate the origin of the mass. CLs are mainly submucosal. So, they can be distinguished from smooth muscle tumors, lymphangiomata, and invasive or metastatic malignancies. EUS is also useful in the determination of a possible extension of the SCLs into the muscularis propria before endoscopic resection. For definite diagnosis, computerized tomography (CT) scans are used. On CT, CLs present characteristic fatty densitometric values of 40 to 120 HU 6 and have a uniform appearance with smooth border. For small lipoma though, the diagnostic value of CT is low due to artifacts and partial volume averaging. 1 Recently, reports describe the usefulness of magnetic resonance imaging (MRI) in the diagnosis of CLs. 6 The signal intensity is characteristic of adipose tissue on T1-weighted and fat suppressing images.
The decision whether to remove lipomas and which method is the best option either endoscopically or surgically remains controversial. 7 The general agreement is that colon lipomas <2.0 cm in diameter are more accessible for endoscopic treatment. 3 Endoscopic removal is not suggested for lesions >2.0 cm due to the high risk of complications, such as bleeding and perforation. 7
Traditionally, surgical treatment has been the choice for large SCLs.5,8 It is generally accepted that the difficulty of obtaining preoperative diagnosis influenced the type of surgical treatment undertaken. Colectomy with lipomectomy and limited colon resection are considered an adequate treatment modality for certain colon lipomas diagnosed preoperatively.5,8,9 However, a segmental resection, hemicolectomy, or subtotal colectomy may be necessary in isolated cases when diagnosis is questionable or when a complication occurs.3,5,10 Recently, laparoscopic procedures and minimal laparotomy approach were reported as an alternative to conventional laparotomy used in removal of large CLs.7,9 Both approaches involve shorter operation times, less postoperative pain, shorter duration of ileus, and quicker recovery.9,11
A definitive diagnosis of CLs is often obtained from histopathological examination of the resected specimen. 12 Macroscopically, they are yellowish, well-circumscribed, soft, and compressible lesions. Lipomas consist of well-differentiated adipocytes, while fibrous diaphragms among organize them in lobules. 3 Malignant transformation has never been reported; although when examined histologically, some lipomas have atypical “pseudosarcomatous” features.13,14 In general, recurrence of colon lipoma after surgical treatment has not been documented. 3
Conclusion
Consequently, although rare, CLs should be considered in the differential diagnosis of symptomatic bowel tumors. Preoperative diagnosis is difficult to be set, so lipomas are often mistaken for adenomatous polyps or carcinoma. 3 Surgical approach is still the treatment of choice, while the type of procedure depends on correct preoperative diagnosis, size, and location of lipomas, as well as the presence of complications.
Footnotes
Acknowledgements
All authors contributed equally to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article and it is available for the editor and editorial office if requested.