
Abstract
Introduction
Approximately 1 in 300 Canadians identify as transgender and non-binary (TNB). 1 Based on individual needs, gender affirmation can encompass social, legal, medical, and surgical components. Gender-affirming surgeries (GAS) align an individual's anatomy with their gender identity. They have been associated with positive health outcomes including improved quality of life and reduced psychological distress.2,3 Surgeries can be divided into those that ‘feminize’ or, masculinize, the body, although these terms may not align with TNB individuals’ gender affirmation goals. Individuals of varying gender identities, including trans men, trans women, and non-binary identities may require GAS.
The number of GAS performed annually is increasing across Canada. In 2018, over 1600 procedures were approved as medically necessary in Ontario alone, 4 equivalent to approximately 1 approval per 9000 residents. Despite increasing prevalence, the basic demand for GAS within the TNB community in Canada, including patient preference for GAS procedures and subsequent completion rates, remains unclear. The objective of this study is to describe the desired surgeries among participants, the procedures they were able to access and categorize these findings by surgery type (feminizing vs masculinizing) as well as gender identity.
Methods
A national, community-based cross-sectional survey was conducted by Trans PULSE Canada from July 26–Oct 1, 2019. More detailed methodology is available in Scheim et al. 5 The Trans PULSE Canada 2019 survey was approved by research ethics boards at Western University, Unity Health Toronto, and Wilfrid Laurier University. This specific sub analysis underwent review by the Trans PULSE Steering Committee and was approved by Women's College Hospital. For all age groups, informed consent was implied upon voluntary completion and return of the survey. No additional consents were required for those under the age of 18.
Data Collection
TNB individuals aged 14 + were recruited via convenience sampling to participate in the English- or French-language survey online, on paper, by phone (with a language interpreter), or in-person in 10 major urban centres across Canada (Vancouver, Calgary, Edmonton, Saskatoon, Winnipeg, Southwestern Ontario, the Greater Toronto Area, downtown Toronto, Ottawa and Montreal). The survey was distributed through multiple venues including online (eg, mailing lists and social media), in person (eg, pride festivals), and through outreach by peer research associates.
The survey was available in full-length (approximately 60 min to complete) and short-form (approximately 10 min) versions. Surgery questions were only received by participants who chose to complete the full-length survey (86.4% of 2873 total respondents). For the 2019 survey, the research team adapted core survey items on surgeries from Trans PULSE Ontario (2009–2010), 1 with review by nine priority population teams (eg, immigrant, youth, non-binary) for community language and clarity.
Study Variables
Participants were asked their sex assigned at birth (male/female), and their gender identity (man or boy, woman or girl, indigenous or other cultural gender identity (eg two-spirit), and non-binary, genderqueer, a gender or a similar identity). For this study non-binary individual includes genderqueer, agender, or similar identity and Indigenous or other cultural gender minority (eg, two spirit). Self-reported demographic variables including age (years old), highest level of formal education (categories ranging from some high school to graduate/professional degree), household income level (categories ranging from <$15,000 to $100,000 or more), race (person of colour - yes/no), disability (yes/no), citizenship (Canada or other country/countries only), province/territory of residence, and current or past hormone use (yes/no) were collected via the survey.
Participants were asked about their history of gender-affirming surgical procedures that included breast augmentation or mastectomy, feminizing or masculinizing facial procedures, body contouring, voice surgeries, orchidectomy, hysterectomy (+/- oophorectomy), vaginoplasty, phalloplasty, and metoidioplasty. The surgical terms were simplified by community knowledge users so it would be understandable for all people completing the surgery. Trans women and non-binary individuals who were assigned male at birth (AMAB) were asked about feminizing surgeries and trans men and non-binary individuals who were assigned female at birth (AFAB) were asked about masculinizing surgeries. For each type of feminizing or masculinizing surgery, participants selected 1) do not want; 2) want; or 3) have had.
Data Analysis
SAS version 9.4 (SAS Institute Inc., Cary, North Carolina, USA) was used for data analyses. Those who indicated that they ‘want’ surgery type or ‘have had’ surgery type comprise the total number of individuals that ‘desired’ each surgery type (‘want’ + ‘have had’ = ‘desired’). Raw percentages are reported. Weighted t-test for means and Rao-Scott chi-square tests for proportions were done to compare TW and NB AMAB and TM and NB AFAB and generate p-values to show there was no major difference in demographic data from those populations and demonstrate that the surgical desire rates are coming from comparable patient populations (Tables 1 and 2).
Sociodemographics of the Survey Sample Wanting Feminizing Surgeries.
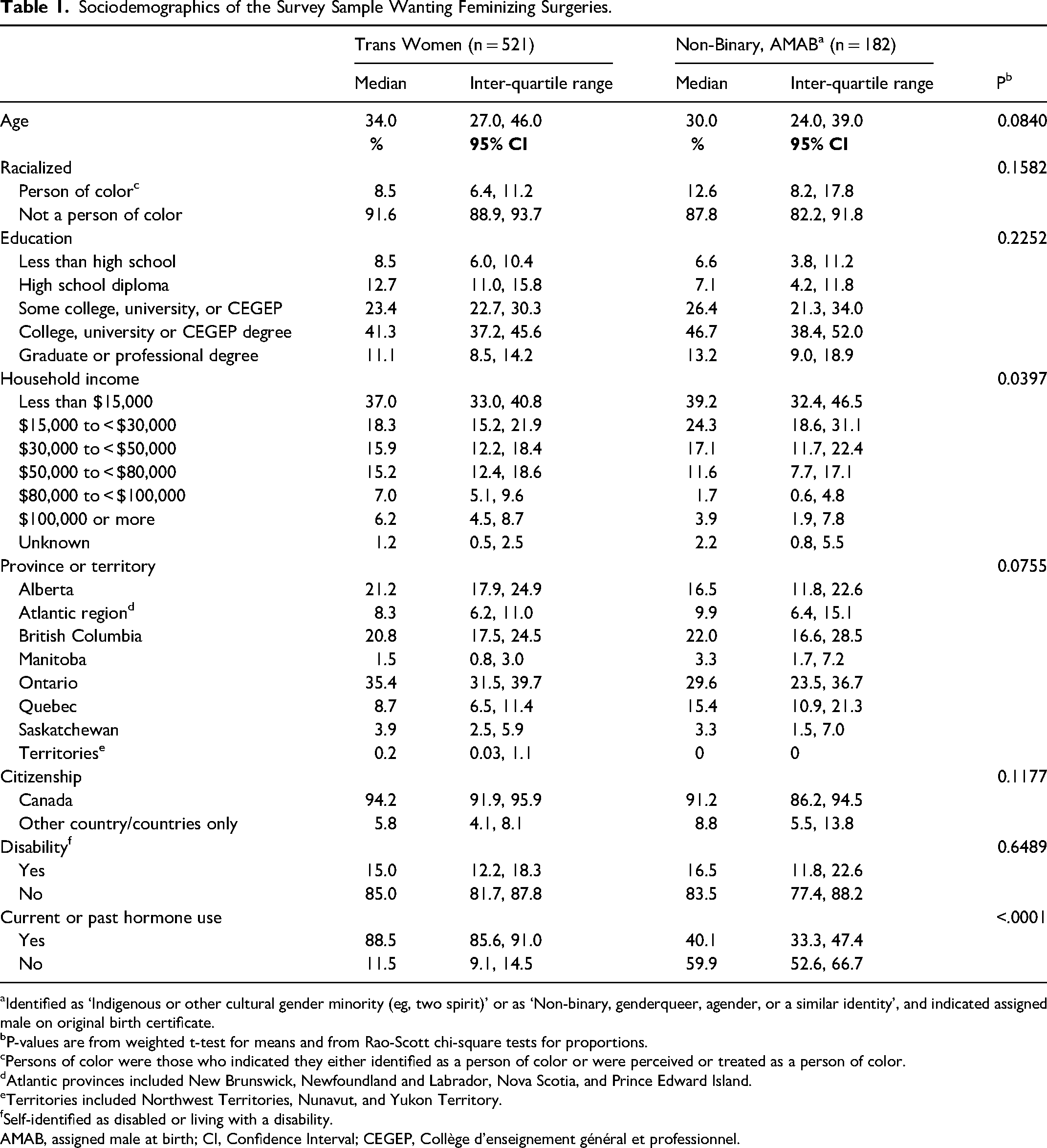
Identified as ‘Indigenous or other cultural gender minority (eg, two spirit)’ or as ‘Non-binary, genderqueer, agender, or a similar identity’, and indicated assigned male on original birth certificate.
P-values are from weighted t-test for means and from Rao-Scott chi-square tests for proportions.
Persons of color were those who indicated they either identified as a person of color or were perceived or treated as a person of color.
Atlantic provinces included New Brunswick, Newfoundland and Labrador, Nova Scotia, and Prince Edward Island.
Territories included Northwest Territories, Nunavut, and Yukon Territory.
Self-identified as disabled or living with a disability.
AMAB, assigned male at birth; CI, Confidence Interval; CEGEP, Collège d'enseignement général et professionnel.
Sociodemographics of the Survey Sample Wanting Masculinizing Surgeries.
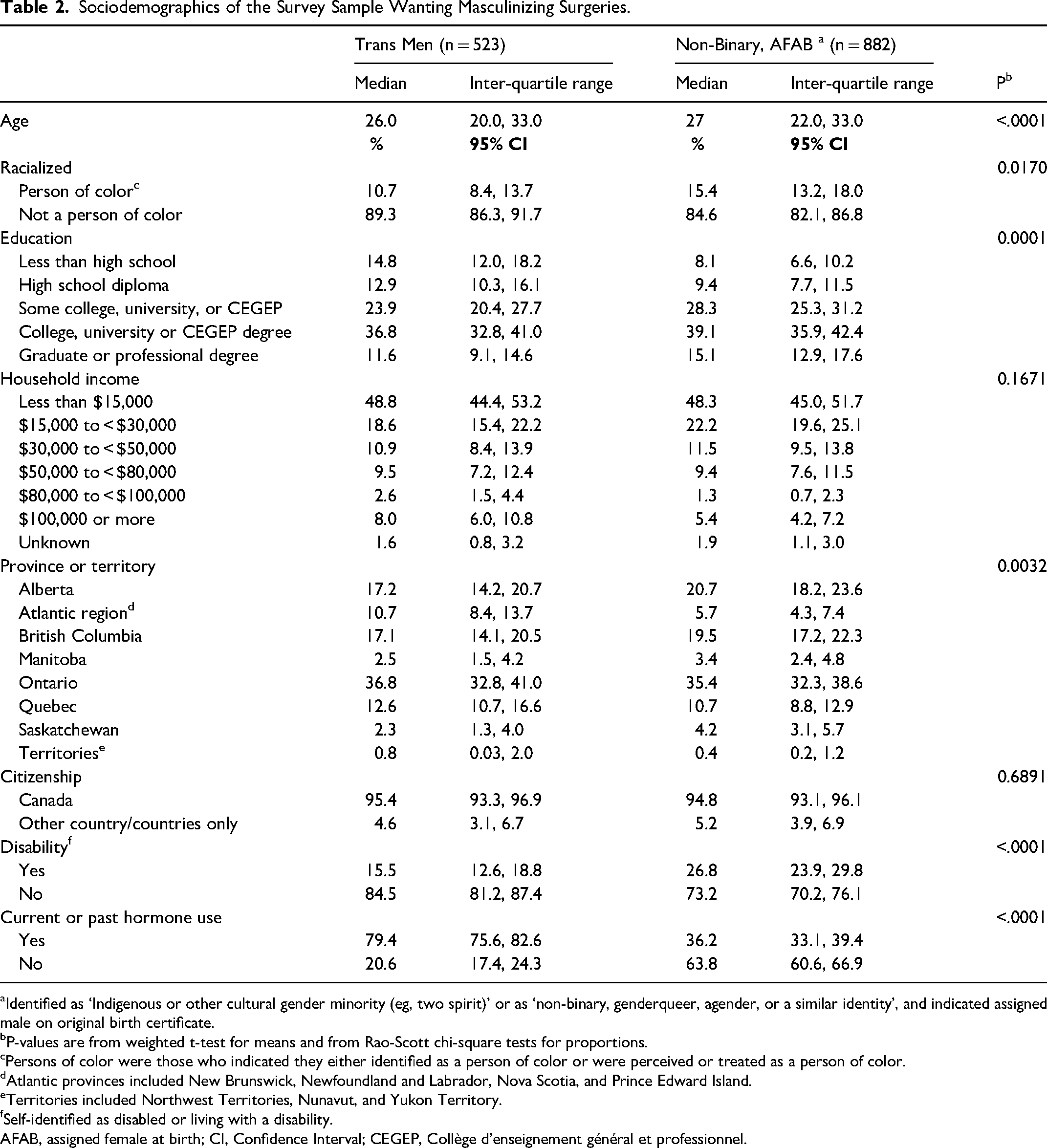
Identified as ‘Indigenous or other cultural gender minority (eg, two spirit)’ or as ‘non-binary, genderqueer, agender, or a similar identity’, and indicated assigned male on original birth certificate.
P-values are from weighted t-test for means and from Rao-Scott chi-square tests for proportions.
Persons of color were those who indicated they either identified as a person of color or were perceived or treated as a person of color.
Atlantic provinces included New Brunswick, Newfoundland and Labrador, Nova Scotia, and Prince Edward Island.
Territories included Northwest Territories, Nunavut, and Yukon Territory.
Self-identified as disabled or living with a disability.
AFAB, assigned female at birth; CI, Confidence Interval; CEGEP, Collège d'enseignement général et professionnel.
Results
Of 2873 full-length survey participants, 2118 answered surgery questions and were included in the analytic sample, including 521 trans women, 182 non-binary individuals AMAB, 533 trans men, and 882 non-binary individuals AFAB. Less than 5% of responses were missing for any question. As it was such a small percentage of missing responses, the missing one was excluded, and the rest of the answered questions were included for analysis.
Feminizing Surgeries
As shown in Figure 1, the most desired procedures for trans women were bottom surgeries including vaginoplasty (84% desired; 26% completed) and orchidectomy (67% desired; 21% completed). Fewer non-binary AMAB individuals desired vaginoplasty (32%) or orchidectomy (35%). Among non-binary AMAB individuals, the most desired procedures were facial surgeries (45%), although a higher proportion of trans women desired facial surgeries (65%).
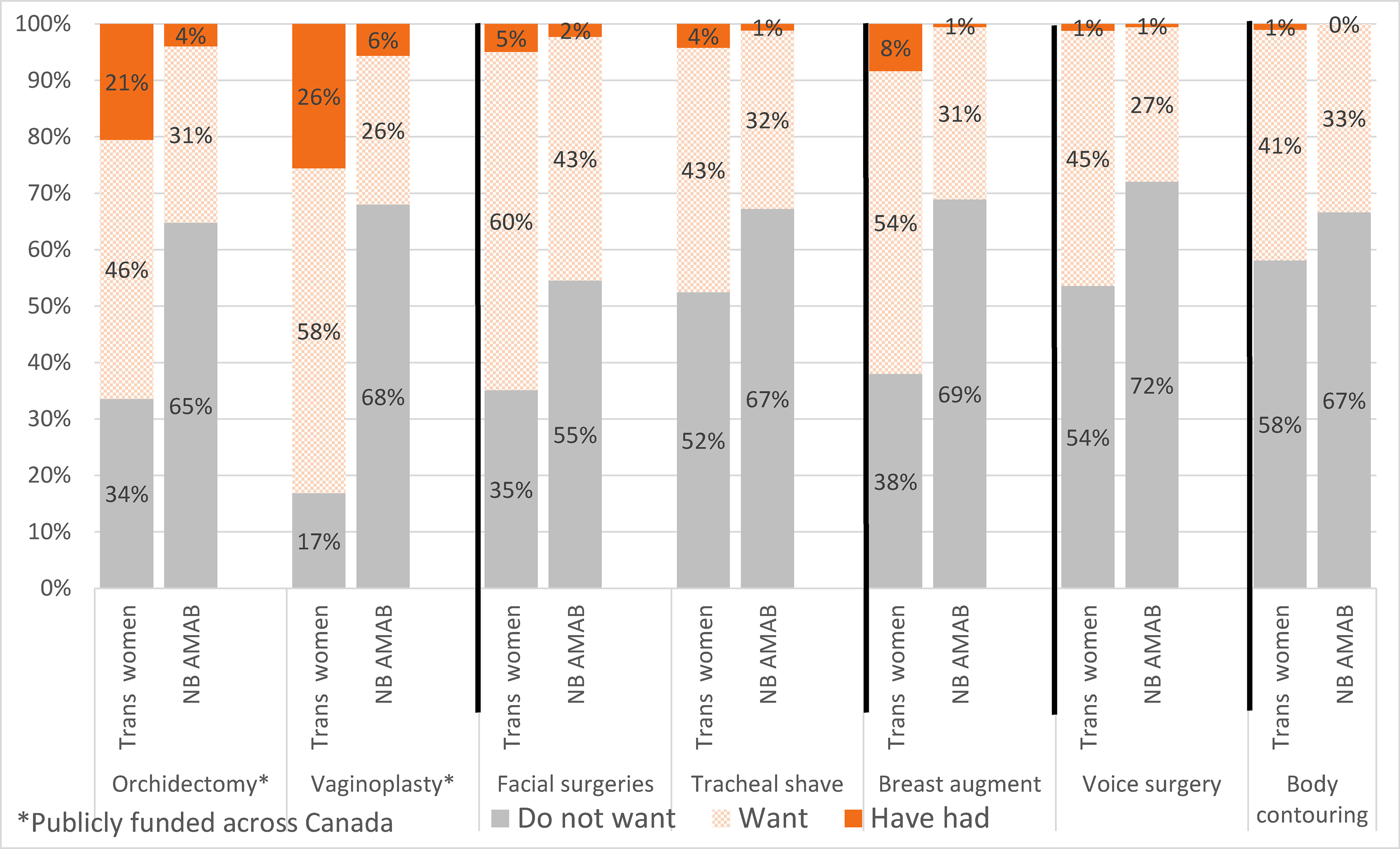
Preferences for Types of Gender-Affirming Surgeries. A. Preferences for Types of Gender-Affirming Surgeries among Trans Women and Non-Binary People who were Assigned Male at Birth (n = 703).
Among trans women, 62% wanted breast augmentation with only 8% having completed surgery. Non-binary AMAB individuals were less likely to want (32%) and complete (1%) the same procedure. In general, non-binary AMAB individuals were less likely to complete all surgical procedures (Figure 1).
Masculinizing Surgeries
As shown in Figure 2, among trans men, 98% wanted mastectomy/chest masculinizing surgery with 48% having accessed surgery. A majority of non-binary AFAB individuals wanted the same procedure (63% wanted, 17% accessed), though proportions were lower than for trans men.
Hysterectomy and oophorectomy were the second and third most wanted GAS respectively, with lower completion percentages for both in the non-binary AFAB population. Among trans men, 75% wanted a hysterectomy and 23% had accessed one. This mirrored desire and access for oophorectomy (71% and 22%, respectively). This compares to only 46% of the non-binary AFAB population wanting hysterectomy and only 7% having accessed one. There was less desire for oophorectomy among non-binary individuals (33%).
For masculinizing bottom surgery, 48% of trans men wanted metoidioplasty and 38% wanted phalloplasty. This compares to 17% and 6% of non-binary AFAB individuals wanting metoidioplasty and phalloplasty, respectively. Completion percentages for both types of masculinizing bottom surgery were extremely low in both groups (range 1%–4%; see Figure 2).
Facial surgeries were the least desired surgeries among trans men; and facial and phalloplasty surgeries were the least desired among non-binary AFAB individuals. See Figure 2.
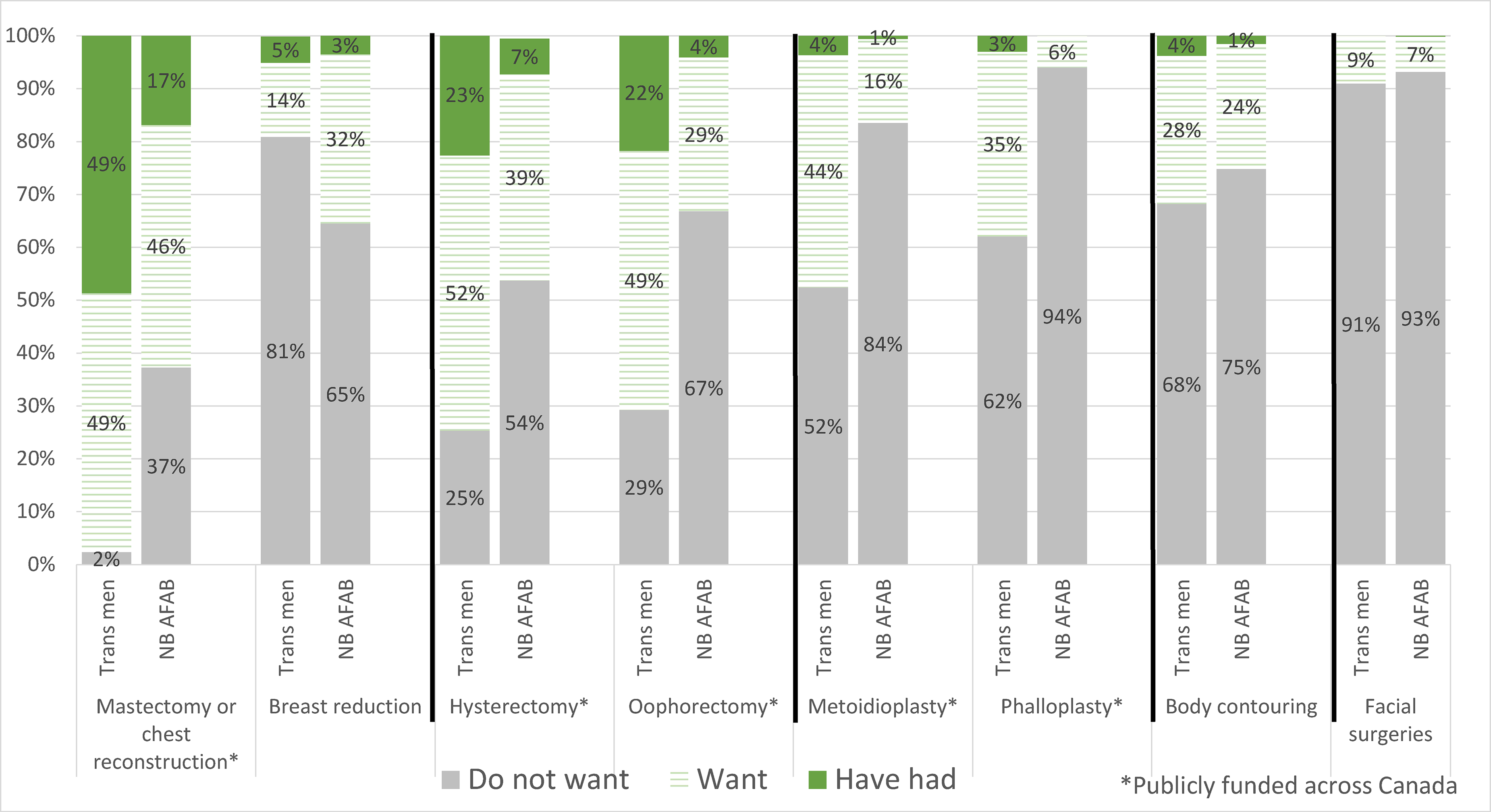
Preferences for Types of Gender-Affirming Surgeries. B. Preferences for Types of Gender-Affirming Surgeries among Trans Men and Non-Binary People who were Assigned Female at Birth (n = 1405).
Discussion
This study reminds us that the population presenting to gender affirming clinics, including surgery clinics, is not fully reflective of the entire transgender and non-binary community. In addition, although gender identity can influence gender-affirming goals, these goals vary substantially even among individuals within the same gender identity group. It also reminds us that a desire or want for surgery does not necessarily mean that an individual would complete all steps to access surgery and be deemed medically fit for surgery. However, it does inform our understanding of the general desires with the TGD community.
This analysis revealed a high demand for both feminizing and masculinizing GAS and overall low rates of access or completion. Desire and completion percentages varied by gender identity and surgery type. The best access was achieved by trans men desiring mastectomy and trans women desiring vaginoplasty. Within these groups, only half of the trans men desiring mastectomy had accessed it, and only one-third of the trans women desiring vaginoplasty had accessed it. These are two procedures deemed medically necessary and covered by all provincial and territorial health insurance across Canada, yet meaningful gaps in completion persist.
It is important to note that these data reflect the Canadian landscape as it existed in 2019. Since that time, significant structural changes have occurred. Two major publicly funded multidisciplinary surgical programs have been developed in British Columbia and Ontario, increasing national capacity for GAS. 6 During the same time period, demand for GAS has also grown, making it difficult to determine the current balance between need and capacity in 2026. In addition, the scope of publicly funded care has expanded: in recent years, both Yukon and Prince Edward Island have broadened their gender-affirming surgical access, now encompassing facial feminization. 6 This aligns with the substantial demand for facial feminization procedures among transgender women and non-binary individuals seen in this study.
Limitations
This study is limited by the self-reported and convenience sampling nature of the data. The TGD community is considered a hidden and vulnerable community that is less likely to engage in research due to mistrust and/or participation risk and/or low perception of benefit from research. A strength of this study is its community based participatory research design, which involves community members throughout all aspects of design, implementation and preparation of final manuscript. 7 In addition, the survey did not capture whether participants who were waiting for surgery had already received consultation or booking date; therefore, we could not distinguish between long surgical waitlist and inability to access a surgical assessment. There was also unequal representation across provinces and territories, limiting inter-regional comparisons.
Conclusion
Access to GAS is limited by a number of barriers well described in the literature. 8 The low surgical completion percentages speak to persistent challenges despite provincial health insurance coverage for some surgeries. This emphasizes the need to address barriers to ensure equitable access to gender-affirming care. Further research is needed to understand how to mitigate these barriers effectively.
Footnotes
Acknowledgements
The Trans PULSE Canada Study Team would like to acknowledge and thank the trans and non-binary people who have generously shared their time and experience with us.
Author Contributions
Kathleen Armstrong: Study design, data analysis, manuscript write-up, manuscript review
Ayden Scheim: Data interpretation, manuscript review
Gioi Tran: Data analysis, data interpretation, manuscript review
Emery Potter: Data interpretation, manuscript review
Adrian Edgar: Data interpretation, manuscript review
Greta Bauer: Study design, data analysis, data interpretation, manuscript review
Availability of Data and Material
As per the participant consent letter, Trans PULSE Canada data can be accessed only by members of the team's Data Analysis Working Group.
Consent for Publication
Not applicable.
Consent to Participate
Informed consent was obtained from all patients for being included in the study. For all age groups, informed consent was implied upon voluntary completion and return of the survey. No additional consents were required for those under the age of 18.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The Trans PULSE Canada 2019 survey was approved by research ethics boards at Western University, Unity Health Toronto, Wilfred Laurier University. This specific sub analysis underwent review by the Trans PULSE Steering Committee and was approved by Women's College Hospital (REB#2023–0043-E). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the WCHAMSG Innovation Fund of the Alternative Funding Plan for the Academic Health Sciences Centres of Ontario, Canadian Institutes of Health Research (grant number WCH 23-006, PJT-159690).