
Abstract
This narrative review provides an in-depth description of gender-affirming breast surgery within the context of publicly funded healthcare systems in the Nordic countries. A comprehensive literature search was conducted in collaboration with two information specialists, focusing on original research, reviews, and clinical guidelines published in English. The prevalence of transgender and non-binary individuals in the Nordic region ranges from 0.04% to 0.6%, depending on the country and study methodology. Gender-affirming treatment, including hormone therapy and surgical interventions such as breast augmentation and mastectomy, plays a critical role in reducing gender dysphoria and improving psychological well-being, with low rates of reported regret. Transfeminine individuals often pursue breast augmentation with implants or autologous fat grafting; procedures tailored to their unique anatomical considerations. These surgeries are associated with improved health-related quality of life and high levels of satisfaction. Surgical planning involves careful consideration of implant type, placement, and incision strategy. Transmasculine individuals commonly undergo chest masculinization, with techniques adapted to breast size, ptosis, skin quality, and individual goals. Both implant-based and mastectomy procedures are generally safe, though complications such as capsular contracture, hematoma, or wound healing disturbances may occur. Although regret is rare, it underscores the need for comprehensive assessment, informed consent, and mental health support throughout the transition process. Breast cancer screening guidelines remain inconsistent, with barriers to access due to legal gender markers and varying levels of provider knowledge While Nordic countries vary in their approaches, all aim to balance medical necessity, individual autonomy, and healthcare equity. Future priorities include refining surgical protocols, expanding research on long-term outcomes, and addressing systemic barriers to ensure inclusive, evidence-based care for all gender-diverse individuals.
Keywords
Terminology
Introduction
The prevalence of transgender and non-binary individuals in the Nordic countries varies according to studies. In Sweden, it is estimated at 0.5% of the population,1,2 while Denmark reports 0.06%. 3 In Finland, 0.6% of adolescents identified with the opposite sex and 3.2% as non-binary or other genders. 4 A 2018 Norwegian student survey found that 0.2% identified as transgender or non-binary. 5 In Iceland, 159 individuals (0.04% of the population) were registered as “non-binary/other” in 2024. 6 These estimates depend on definitions and methodologies used.
Transgender individuals experience incongruence between gender identity and assigned sex at birth, which may cause gender dysphoria. 7 While Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria are used internationally for diagnosis, the International Classification of Diseases (ICD) classification is more commonly applied in the Nordic countries. Studies show that transgender individuals face higher rates of anxiety, depression, and suicide compared with cisgender individuals.8–11
Gender-affirming treatment, including hormone therapy and surgery, aims to reduce dysphoria and improve well-being. Increasing evidence supports improvements in health-related quality of life (HRQoL) and gender congruence after treatment,12–16 with regret being infrequent. Reported regret rates are below 1% in various studies,17–19 with one Swedish study noting a 2.2% rate of detransition. 20
Gender-affirming breast surgery is a key component of gender transition for many individuals. In the publicly funded healthcare systems of the Nordic countries, gender-affirming breast surgery includes breast augmentation with implants, or lipofilling in Finland, for transfeminine individuals and chest masculinization/mastectomy for transmasculine individuals.
Methods
A comprehensive literature search was conducted to identify relevant publications for this overview. The search strategy was developed in collaboration with two information specialists. Searches were performed in selected databases (PubMed, Embase, PsycInfo and Web of Science) using a combination of MeSH terms and relevant keywords related to gender-affirming treatment. Only articles published in English were included, with no restrictions on the year of publication. The selection focused on original research, review articles, and key clinical guidelines.
Gender-affirming breast augmentation
Transfeminine individuals are usually offered gender-affirming surgical care in the form of breast augmentation with implants or fat grafting, 21 that for many is a key component of the gender-affirmation process. The goal of the surgery is to create more feminine appearing breasts. 22
Indications
In the Nordic countries, following a comprehensive evaluation and confirmed diagnosis of transsexualism by a specialized gender team, individuals may be referred to a plastic surgery clinic for gender-affirming breast augmentation. The age requirement is 18 years or older for surgery.
Gender-affirming hormonal therapy alone may lead to sufficient breast tissue development, potentially eliminating the need for surgical augmentation. The effects of hormone therapy on breast tissue development, however, vary considerably.
In Norway, the recommendation is at least 1 year of feminizing hormone treatment before surgery. In Finland, 2–3 years of hormone treatment, and in Denmark, a minimum of 12 months. By contrast, in Iceland, breast augmentation is not funded by the state and individuals seeking gender-affirming breast augmentation must pay for the surgery privately. In Iceland, at least a 1-year hormonal therapy course is recommended before surgery. In Sweden, at least 2 years of consistent hormonal therapy before considering breast augmentation is recommended.
As with other gender-affirming surgeries, coexisting mental or physical health conditions must be adequately managed prior to surgery.
Breast augmentation with implants
Surgical techniques & surgical pearls
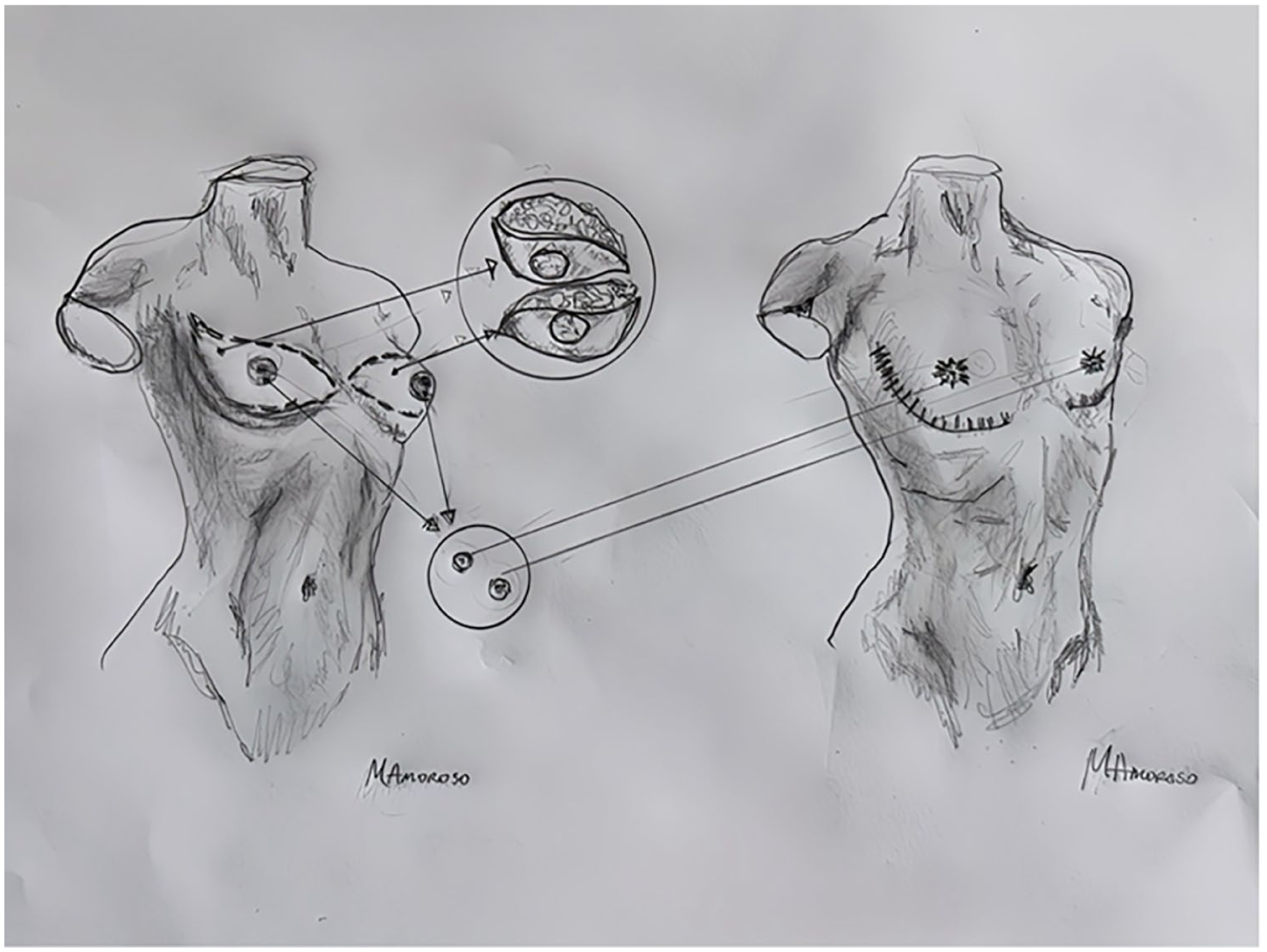
Compared with breast augmentation with implants in cis women, in transfeminine individuals, several specific factors must be taken into consideration. The procedure includes making an incision in the skin, creating a pocket for the implants, and placing them to achieve a more feminine contour of the chest and breasts 22 (Fig. 1). The procedure is performed under general anesthesia, takes about 1 h, and is typically performed as outpatient surgery. Technical considerations in gender-affirming breast augmentation include the following:
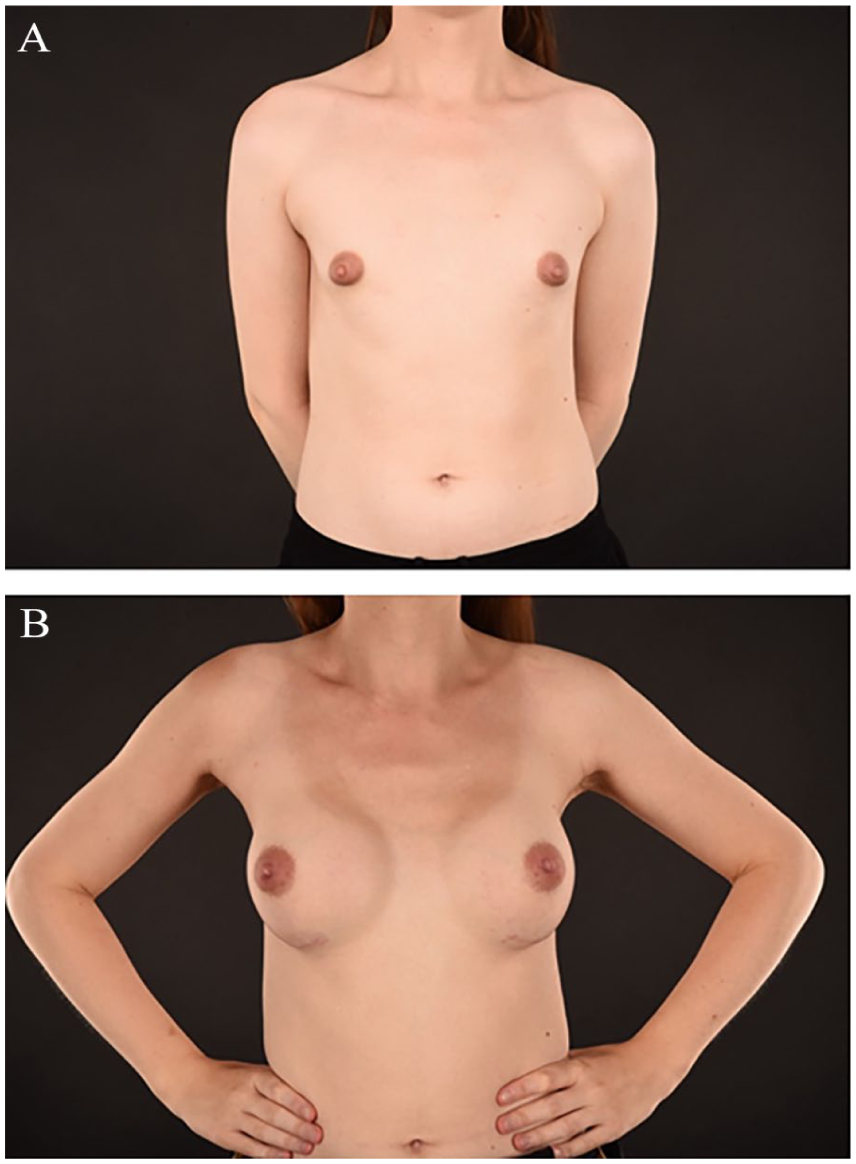
Example of (A) pre- and (B) postoperative images after breast augmentation in a trans woman.
Recovery and postoperative care
Most patients can resume light activities immediately after surgery, and return to normal activity after 4–6 weeks. An elastic breast band is placed cranially to the breasts to press the implants downward. and is combined with a sturdy supportive bra. As with most surgeries, temporary swelling and bruising are common. Pain is usually manageable with oral pain medication. Potential risks and complications include implant rupture, capsular contracture, infection, bleeding/hematoma, changes in sensation of the skin and nipple, and scarring. 32
Breast augmentation with autologous fat grafting
Autologous fat grafting, often called lipofilling, to the breast is commonly used in breast contouring and volume correction in both reconstructive and aesthetic surgery. It can address a wide range of breast issues, from minor shape adjustments to full breast reconstruction. 33 Fat grafting creates a natural-appearing contour with permanent result after the immediate recovery period. Fat retention rate varies from 40% to 82%. 34 In gender-affirming breast surgery autologous fat grafting offers an option for implant augmentation. The ideal candidate has adipose tissue in multiple areas suitable for fat harvesting and supple skin on the chest.
Surgical techniques
Breast augmentation with lipofilling enhances the breast shape and size in a three-dimensional way through a scaffold composed of thin arrays of fat strands. Generally, gender-affirming breast lipofilling does not differ from that in cisgender women. Due to the same specific considerations for transgender women as described for implant augmentation, a greater amount of fat needs to be transferred and typically more than one operation is required.
The donor site for fat grafting is chosen based on the distribution of available fat and individual preferences. The most common sites are the abdomen, the lumbar area, and the thighs. The fat distribution may differ from that in cisgender women and can resemble that in cisgender men. The fat is harvested with liposuction and is separated from fluids and blood, before getting injected into the breasts. The technique used in Helsinki has previously been described in detail.35,36 The procedure can be performed under local or general anesthesia, takes about 2 h, and is typically performed as outpatient surgery.
Recovery and postoperative care
Most patients can resume light activities immediately post-surgery and resume normal activity after 1–2 weeks. The breasts should be kept warm and pressure-free for 1 week. A pressure garment is used on the donor site for 2–3 weeks. Potential risks and complications include infection, subcutaneous hematoma, changes in sensation of the skin and nipple, fat necrosis, oily cyst, donor-site deformity, and radiologic changes. 36
Gender-affirming mastectomy
Gender-affirming mastectomy (GAM), is performed to remove breast tissue and create a more masculine or non-binary chest contour. It is a key component of gender-affirming care for transgender men and some non-binary individuals who experience gender dysphoria related to their chest.12–15
Indications
In all Nordic countries, access to GAM requires a formal diagnosis of gender incongruence, issued by a multidisciplinary team at a specialized gender identity clinic. Treatment eligibility includes a minimum age of 18 years, stable mental health, and capacity to provide informed consent.
In Denmark, only public gender clinics can issue diagnoses, and surgery is offered exclusively within the public system. Mastectomy for non-binary individuals without prior hormone therapy is rare and not available in private clinics. A 6-month course of masculinizing hormone therapy is usually recommended before referral for chest surgery in transgender men.
In Finland, diagnosis and referral are coordinated through centralized psychiatric units. Surgery is restricted to adults aged 18 or older, and while hormone therapy is recommended prior to chest surgery, it is not mandatory for non-binary individuals.
Iceland follows similar criteria. While individuals below 18 have not been approved for surgery to date, hormone therapy is not a prerequisite for chest surgery, especially for non-binary patients.
In Norway, diagnosis must be confirmed by the national gender team at Oslo University Hospital. Though no legal age limit exists for chest surgery, it is in practice performed only on individuals aged 18 or older. Hormone therapy is not a strict requirement.
In Sweden, a formal ICD-10 diagnosis (F64.0 or F64.8) is required. Although hormone therapy is not mandatory before surgery, many opt to begin treatment beforehand. The age threshold is 18 years.
Surgical techniques & surgical pearls
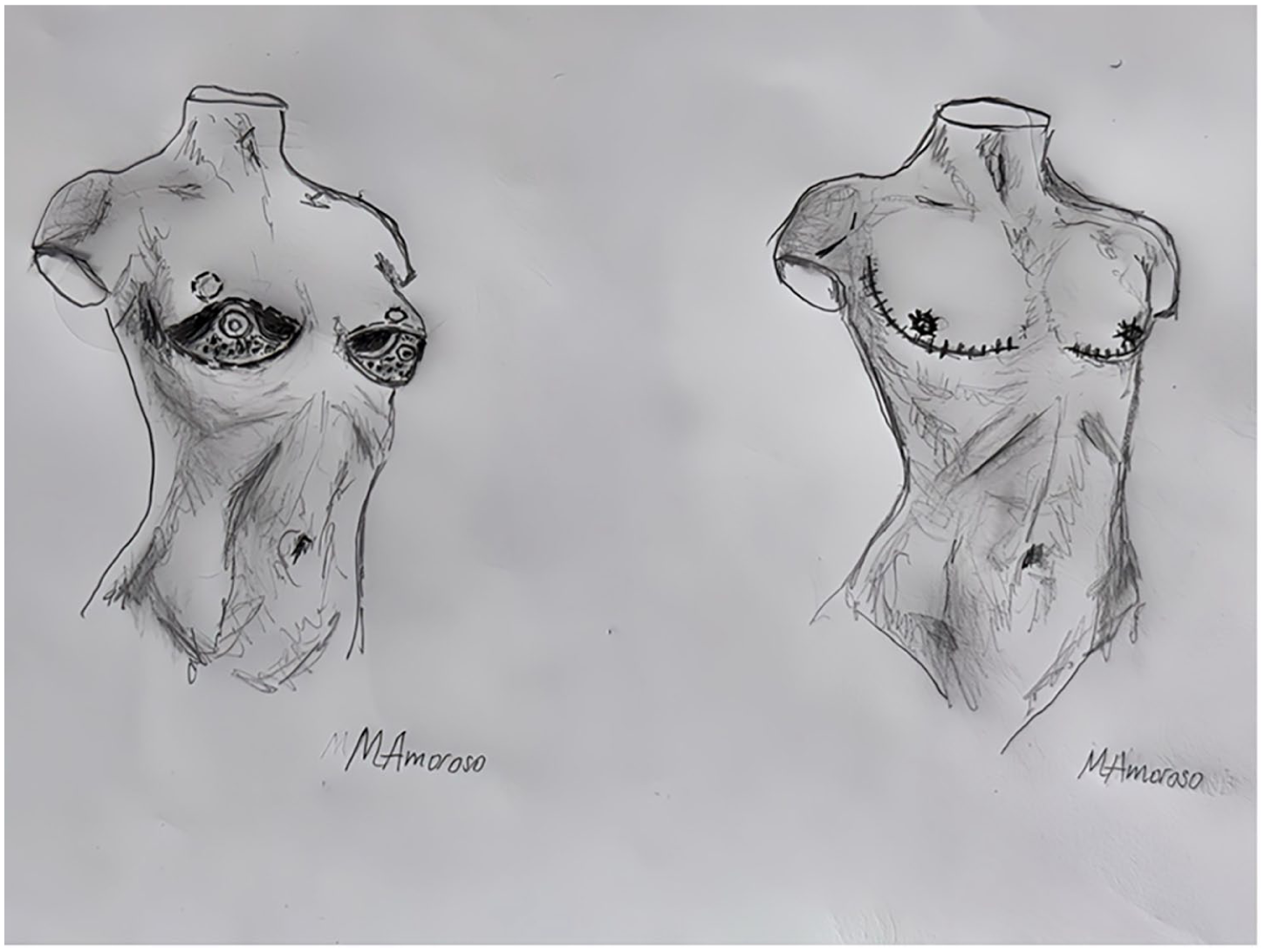
There are several surgical techniques for GAM (Fig. 2), the selection of which is based on factors such as breast volume, skin elasticity and quality, degree of ptosis, and individual preference. Each technique presents advantages and limitations. In general, less invasive techniques yield more discrete scarring but may limit surgical exposure and increase the risk of complications, such as hematoma. Also, less invasive techniques have less effect on skin excess. In a study from 2008 by Monstrey et al., 37 an algorithm for choosing optimal surgical technique based on skin elasticity, breast volume and ptosis is suggested.
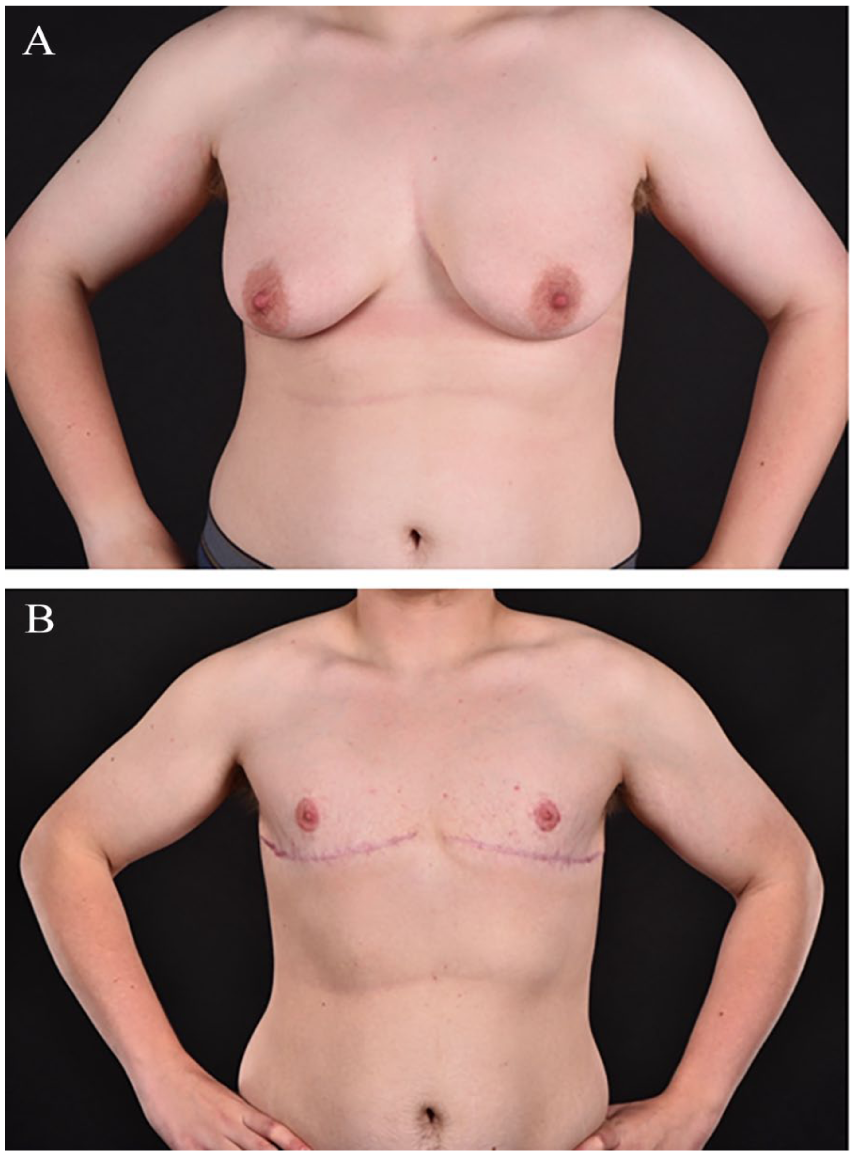
Example of outcome of gender-affirming mastectomy in a trans man. (A) Preoperative and (B) postoperative image.
The most common surgical techniques include the following: 37
It is advised to start by marking the neo-areolar position (where the free NAC graft will be positioned), to prevent high-riding nipples. The nipple should be placed just above the inferior border of the pectoralis major muscle, which can be marked by asking the patient to press their palms together. In a systematic review of anatomical averages of NAC position in cis men, the average sternal notch to nipple distance was 19.3 cm and the average nipple-to-nipple distance was 22.3 cm. 38 However, in trans men, sternal notch to nipple distance is typically shorter than in cis men due to a smaller chest and shorter stature. The distance is usually 16–19 cm, with 18 cm being most common. If the neo-areola is placed higher than 16 cm, the chest will appear odd looking. Timmermans et al. 39 propagate for using an algorithm based on age, weight, chest circumference, and distance axilla-axilla.
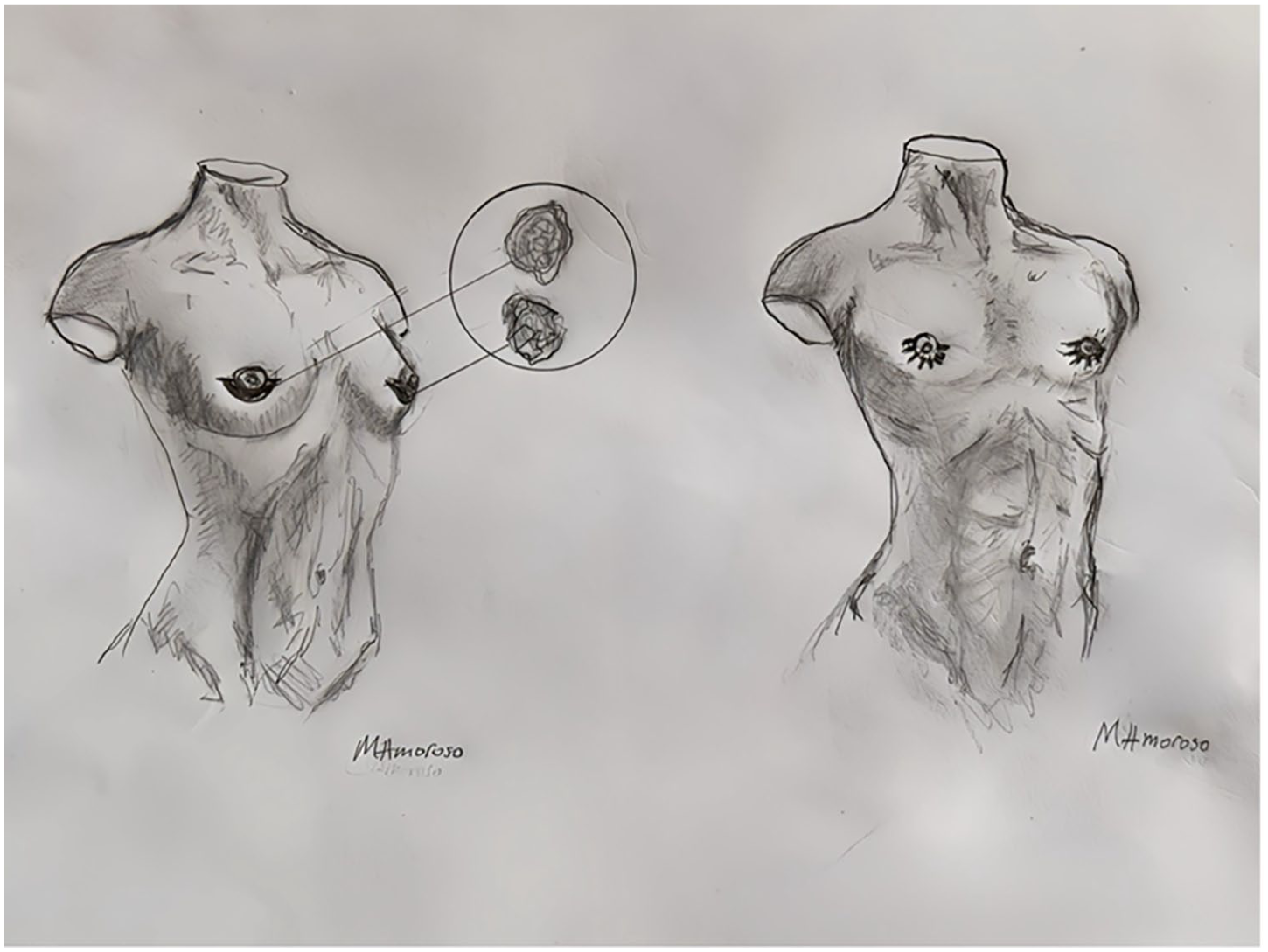
Surgical drawing of subareolar technique.
Surgical drawing of periareolar technique.
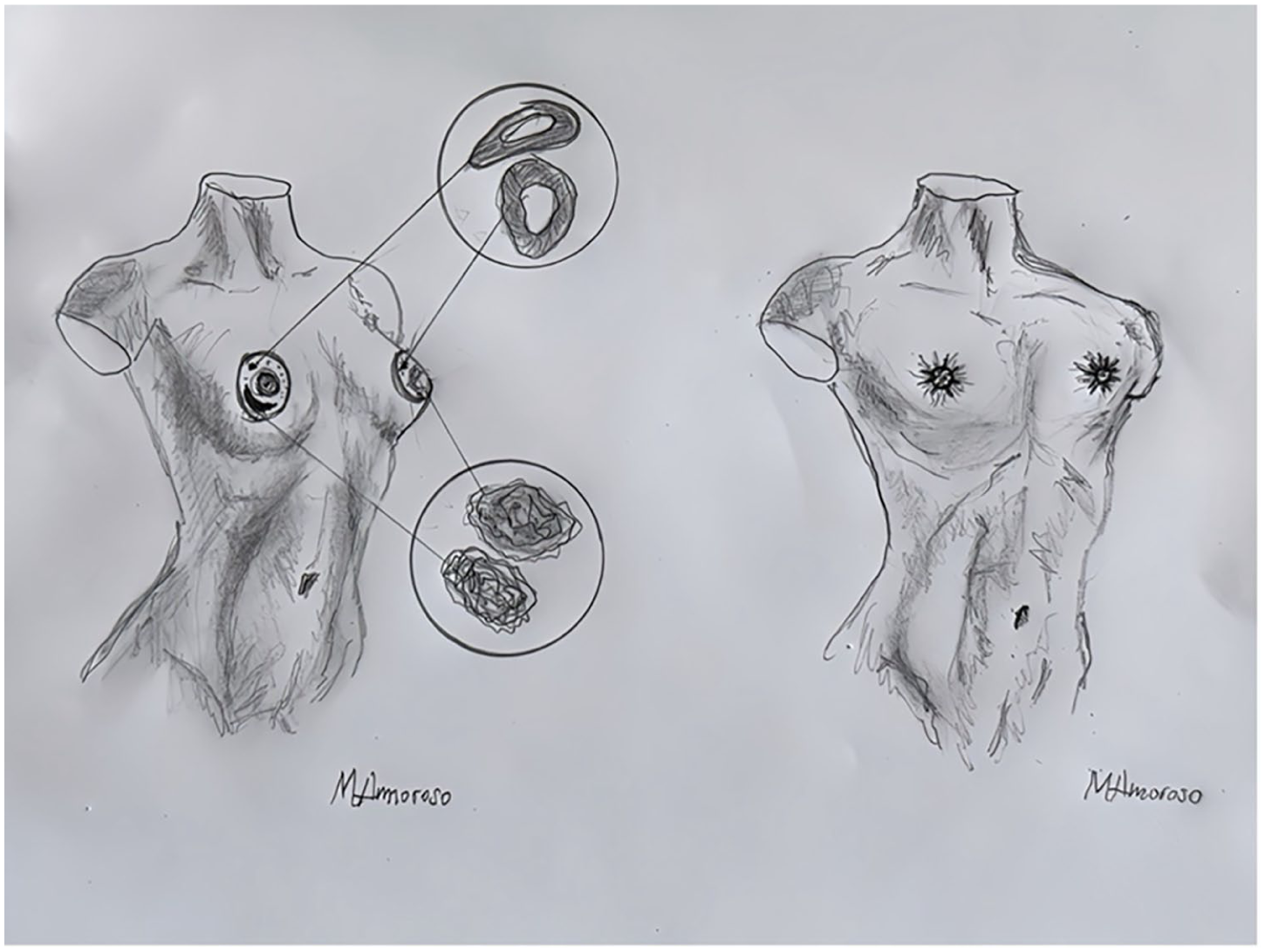
Surgical drawing of double incision with free NAC grafting.
The NAC should be placed more laterally in men than women. The nipple is typically placed 10–11 cm from the midline, just above the pectoral muscle margin, right before it curves laterally toward the axilla. It should sit just medial to the transition between the horizontal and ascending parts of the muscle. This point is typically at the junction of the middle and lateral third of half of the chest wall. 40
Once the nipple position is marked, a 2.5 × 1.5 cm neo-areola is outlined, and the superior excision line drawn 1–1.5 cm below it, depending on remaining skin left to the upper margin of the areola. Previous anatomic studies demonstrate an average male diameter of 2.53 cm. 38
The breast is gently pinched between two fingers to assess where the lower excision line should be placed, typically 1–2 cm above the existing inframammary fold. The incision should not be placed directly in the inframammary fold. Avoiding tension on the incision line results in better cosmetic outcomes in achieving proper wound closure and unsightly scars. 41 The aim should be for the scar to follow the pectoral muscle edge. This means creating an oval incision medially to achieve a horizontal cut, while curving both incisions laterally in a cat-eye shape to create the upward lateral curve following the lateral pectoral muscle border.
The procedure is started by excising the NAC (2.5 × 2.5 cm) as a free graft. Thereafter proceeding with the cranial incision, carefully dissecting just beneath the Scarpa’s fascia. It’s generally advisable to preserve some glandular tissue to avoid excessive thinning of the area. In addition, over-resection laterally toward the axilla should be avoided, as this may lead to postoperative depression in the contour. 41
As the caudal incision is made above the existing inframammary fold, it is important to release the attachment of the fold to prevent retraction below the incision. After closing the incision, the patient should be seated on the operating table with arms alongside the body to mark the position for the neo-areola. A minimum distance of 1 cm between the mastectomy scar and the lower edge of the areola should be ensured. 42 The areola is marked 2.5 × 1.5 cm, as it will always stretch vertically when denuded. 43 To ensure symmetry, a suture can be placed in the jugulum and used to align the sternal notch to nipple distance bilaterally. However, maintaining equal distance to the inferior incision on both sides is more critical, as the human eye is more sensitive to asymmetry in this area than minor discrepancies in the jugulum to nipple distance.
When suturing the areola, an intracutaneous technique is used to prevent stitch marks around the areola. The areola is secured with a bolster, which is typically removed after 1 week.
This technique produces a masculine chest contour but wide, long visible scars. The primary effort should be placing the scars in the pectoral shadow and thereby concealing them as much as possible. Due to the wide incision, this technique provides optimal surgical field of vision, hence low frequency of postoperative hematomas. The radical excision of excess skin and breast tissue enables superior contouring of the chest. This creates a flat chest in one operation with low rate of revision surgeries:
Surgical drawing of pedicled NAC flap technique.
One advantage of this technique is that the NAC retains a more natural appearance. In addition, it allows for the preservation of sensation. This technique is suitable if the nipple-to-inframammary fold distance is ⩽6–8 cm. If the distance exceeds this range, it often results in an excessively bulky and compressed long pedicle, which may require secondary correction, typically with liposuction. Also, the rate of areolar ischemia seems to rise with a pedicle length over 8 cm. 44 As this technique requires a preoperatively relatively short N-IMF distance to prevent excess bulkiness of the new lower pole, it is best suited for medium sized breasts. The key is to make the pedicle thin enough, approximately 5 mm. To ensure optimal blood supply, the base of the pedicle should be wide, typically around 10–12 cm. Apart from the creation of a pedicle to the NAC, this technique applies to the same measurements and surgical technique described above with double incision and free nipple-areola graft.
Recovery and postoperative care
After mastectomy, a wide breast band is applied, compressing the wound cavities, preventing accumulation of blood and fluid. It should be worn around the clock for 2 weeks, followed by wearing it during the day for an additional 2 weeks. Taping the incisions for 3–6 months, changing the tape every 10–14 days is recommended.
The recovery time varies depending on surgical technique and individual healing capacity. Most individuals can resume light activities immediately post-surgery and can resume normal activity after 4–6 weeks. Potential risks and complications include infection, bleeding and wound dehiscence. With free nipple grafting, there is a risk of graft loss. Silicone sheets or creams may be used to reduce and soften scars over time.
Outcomes
Gender-affirming breast augmentation typically helps transgender women alleviate gender dysphoria and improves HRQoL by aligning gender identity with physical appearance. 45 GAM significantly improves mental health, HRQoL and reduces gender dysphoria.14,46,47 Studies show that most individuals report high satisfaction rates post-surgery with minimal regret. 47 However, there is a lack of evidence regarding the long-term effects of gender-affirming breast/chest surgery on HRQoL.47,48 In a prospective long-term follow-up study on transgender women, Lindqvist et al. 16 observed an initial increase in HRQoL post-surgery, followed by a gradual decline over time. 16 This decline was however consistent with the trend observed in the general population, where HRQoL usually decreases naturally with aging.
In a systematic review by Javier et al., 47 long-term HRQoL following various types of gender-affirming surgeries was evaluated. The authors found that transgender men reported moderately high levels of psychological and social functioning after GAM, and concluded that in general, individuals undergoing gender-affirming surgery, reported longer-term satisfaction, with very few expressing regrets.
A small portion of individuals have been reported to experience regret following gender-affirming interventions.17,49 In transgender healthcare, regret is a multifaceted phenomenon. It may arise due to social pressure, lack of acceptance by family or in the workplace, or other external factors. 18 Regret may also arise from complications following interventions or unrealistic expectations.17,18,50 Some individuals report that their gender identity is fluid and can change over time, potentially leading to a misalignment with their physical appearance.51–53 Carefully examining the source of regret is of uttermost importance to be able to provide optimal care.
In a Danish study examining satisfaction after GAM comprising 90 individuals, two reported regret. 54 A Swedish study by Dhejne et al. 20 reported that 2.2% of individuals who underwent gender-affirming surgeries later sought detransition or reversal procedures.
Individuals experiencing regret during their gender-affirming journey may require specific professional psychological support to navigate their feelings and options in detransitioning, such as altering hormone therapy or revising surgical interventions.55,56
Breast cancer screening in transgender individuals
Breast cancer screening is an important aspect of healthcare for transgender individuals. Transfeminine individuals develop substantial breast tissue, and long-term exposure to exogenous estrogens may theoretically increase the risk of breast cancer, although current data remain limited.57–59 Some guidelines recommend considering screening for transfeminine individuals after 5 to 10 years of hormone use, particularly in those over age 40 or with additional risk factors. 60
In addition, transmasculine individuals who have not undergone mastectomy retain breast tissue and may still be at risk for breast cancer. Even after chest masculinization surgery, residual breast tissue often remains, though the risk is likely reduced. It is important to note that chest masculinization is typically performed with aesthetic goals in mind and does not constitute a total mastectomy in the oncologic sense. However, standard screening methods with mammography may not always be feasible or accurate after such surgery, and there is no consensus on optimal screening protocols in this population.
In Norway and Denmark, transmasculine individuals undergoing mastectomy are informed that, although the risk of breast cancer is reduced, it is not eliminated. They are also advised that, following a legal change of gender marker to male, they will no longer receive automatic invitations to the national breast cancer screening program. Consequently, individuals are encouraged to contact their general practitioner should they experience symptoms or have concerns related to breast health.
In the Nordic countries, only those who identify as female in the national registry are automatically invited for breast cancer screening. Transgender men who have changed their legal gender, and transgender women who have not, are therefore not invited for breast cancer screening, regardless of having undergone any gender-affirming medical and/or surgical treatment. A referral for mammography and/or ultrasound, usually from a primary healthcare professional, is needed for transgender individuals with a male legal gender, if screening is deemed warranted. Currently, there are no formal guidelines addressing breast cancer screening in transgender individuals in the Nordic countries.
Moreover, transgender people often face stigma, lack of knowledge among healthcare professionals, and discomfort in gendered healthcare environments, which may further hinder participation in cancer screening programs. 60
Breast implant-associated anaplastic large cell lymphoma
BIA-ALCL is a rare T-cell lymphoma that develops in the capsule surrounding textured breast implants. It has been documented in both cisgender and transgender individuals who have undergone breast augmentation with implants. Transgender women are considered to be at similar risk, although the incidence remains poorly defined due to underreporting and limited long-term data. 61
Symptoms of BIA-ALCL typically include late-onset peri-implant seroma, swelling, or a palpable mass, often occurring years after implantation. Diagnosis is confirmed through cytological analysis. 62 In most cases, BIA-ALCL is effectively treated with surgical removal of the implant and the surrounding capsule. When diagnosed early and treated appropriately, the prognosis is generally favorable. 63
Conclusion and future considerations
Gender-affirming care, including psychological support, medical treatment, and surgical interventions, is a vital component of transgender health and well-being. While societal acceptance has improved over time, continued progress in legal protections and medical research remains essential.
In the Nordic countries, access to gender-affirming care requires individuals to demonstrate maturity, persistent gender dysphoria, and stable mental health. The region is recognized for its progressive legal frameworks concerning gender recognition and bodily autonomy.
Chest masculinization surgery is usually granted with relatively low thresholds, provided the individual’s chest does not appear convincingly masculine. In contrast, breast augmentation for transfeminine individuals is approached with greater caution. This cautious stance is due to the finite lifespan of implants, potential complications requiring long-term follow-up, and resource considerations in public healthcare systems. In addition, many transfeminine individuals develop breast tissue through hormone therapy within the typical female range, prompting debate about equitable access to implant-based augmentation for those with naturally smaller breasts, regardless of gender identity.
Despite shared principles, the Nordic countries face distinct organizational challenges. In Iceland, gender-affirming surgeries were traditionally performed at the national university hospital. However, chest surgery has recently been transferred to a private clinic working in collaboration with the official diagnostic team, while genital surgeries have been outsourced to the Netherlands. These developments reflect broader debates about capacity, specialization, and public–private partnerships in the delivery of gender-affirming care across the region. Continued efforts are needed to ensure care remains accessible, evidence-based, and aligned with the rights and needs of transgender individuals.
In Sweden, protocols for gender-affirming care have changed in recent years. In February 2022, the National Board of Health and Welfare (NBHW) updated their recommendations concerning puberty blockers and gender-affirming hormonal therapy. The updated guidance restricts these interventions to individuals aged 18 and older and recommends their use in minors only in exceptional cases and only to those enrolled in a clinical study. 64 Further legal changes in Sweden are scheduled to take effect in July 2025, aiming to simplify the process of changing legal gender by lowering the age limit to 16 years and increasing individual autonomy. Following these changes, legal gender can be changed after a simplified medical evaluation, without the previously mandatory approval from the NBHW. Moreover, eligibility for gender-affirming genital surgery will no longer require NBHW approval, leaving this decision to specialized gender-affirming healthcare providers and the individual. 65
The approach to gender-affirming interventions in the Nordics should adhere to a commitment to evidence-based practice, individual autonomy, and medical ethics. Advancing transgender health requires not only scientific and medical progress but also a societal commitment to reducing prejudice through education and political reforms. All these factors play pivotal roles in advancing transgender healthcare in a way that is not only scientifically sound but also compassionate. Future advancements in this field must continue to balance the provision of safe, effective, evidence-based medical interventions while maintaining and enforcing all citizens’ right to live in accordance with their gender identity.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.