
Abstract
Introduction
Gender-affirming surgery (GAS) is a cornerstone of transgender healthcare, allowing individuals to align their physical characteristics with their gender identity and significantly improving psychological wellbeing. 1 In recent years, the demand for these procedures has grown, driven by increasing societal acceptance and recognition of their profound mental health benefits.2,3 Despite these benefits, access to GAS remains limited, with these barriers often being significantly more challenging for racial and ethnic minorities.4,5
In the United States, minority populations face persistent healthcare inequities influenced by systemic barriers, financial challenges, and implicit biases within medical systems.6–8 For instance, approximately 13.3% of Black adults and 27.6% of Hispanic adults were uninsured in 2022, compared to 7.4% of White adults, limiting their access to essential medical services. 6 These inequities manifest in reduced access to specialized care, longer wait times, and fewer available healthcare providers in underserved areas.9,10 Such disparities are exacerbated by implicit biases, which can further hinder minority patients from receiving timely and equitable care. 8
For transgender individuals from these communities, the difficulty in obtaining care is further complicated by obstacles unique to gender-affirming procedures. 7 Evidence suggests that transgender people of color are disproportionately affected, with lower access to GAS and additional challenges that may hinder the ability to pursue or complete these procedures.1,11,12 These challenges often stem from systemic barriers such as delayed care, limited access to follow-up services, and provider inexperience with performing GAS in diverse patient populations.13,14 These risks, coupled with inadequate preoperative preparation and inconsistent postoperative care, may discourage patients from seeking surgery or exacerbate systemic inequities by limiting access to affirming care for future procedures. 4
Among the wide range of gender-affirming procedures, top (chest masculinization or breast augmentation) and bottom (genital reconstruction) surgeries are the most frequently performed, as they play a pivotal role in improving both gender presentation and psychological outcomes. 1 Yet, the probability of accessing these procedures varies widely among racial and ethnic groups, pointing to a critical gap in equitable healthcare access. 8 Despite ongoing efforts to reduce disparities, access to GAS remains uneven, particularly for transgender individuals in marginalized communities. 15
Top (chest masculinization or breast augmentation) and bottom (genital reconstruction) surgeries represent some of the most common and sought-after forms of gender-affirming surgery due to their profound impact on gender congruence and mental health.1,16 However, while these procedures are increasingly recognized as medically necessary, there remains limited large-scale, empirical research examining whether access to them differs across racial and ethnic groups. 17 Our study examines the odds of receiving GAS across racial and ethnic groups using an ICD-10 database from multiple hospitals across the United States. By addressing a critical gap in the literature, this study aims to uncover disparities in access to GAS among diverse racial and ethnic populations. Through assessing these odds, we seek to shed light on systemic barriers hindering equitable access to essential gender-affirming care. The findings aim to inform healthcare policies and practices that promote inclusive and equitable care for all transgender individuals, regardless of race or ethnicity, contributing to a broader effort to advance healthcare equity in this vulnerable population.
Methods
Data Source
This retrospective cohort study utilized the TriNetX United States Collaborative Network to identify patients eligible for both top and bottom GAS using ICD-10 and CPT codes. TriNetX is a large database comprising 66 healthcare organizations that performed top and/or bottom GAS across the United States, with 116.2 million patients as of August 1, 2024. The data collection period spanned from August 1, 2014 to August 1, 2024, and included patients meeting the eligibility criteria for top or bottom GAS.
Inclusion Criteria
The cohorts for this study were stratified by race to assess racial disparities in access to GAS. Patients were identified using ICD-10 codes for gender identity diagnoses, such as transsexualism (F64.0), dual role transvestism (F64.1), other gender identity disorders (F64.8), and gender identity disorder (F64.9). These codes were chosen to encompass a broad spectrum of gender identities and ensure the inclusion of individuals potentially seeking GAS, thereby capturing diverse gender identity experiences. Eligible patients were at least 18 years old, had undergone hormone therapy for at least 6 months (ICD-10: Z79.890), and had a prior diagnosis of gender dysphoria (ICD-10: F64.0). These criteria ensured the study population met established clinical guidelines for top or bottom GAS. The study specifically evaluated the odds of patients from different racial groups receiving GAS at 6 months and 1 year after meeting these eligibility criteria, allowing for a detailed analysis of disparities in access and timing across demographic groups.10,12
Variables and Outcomes
The primary outcome of the study was the likelihood of undergoing top or bottom GAS for each racial group at 6 months and 1 year after becoming eligible. To analyze disparities in surgical access, comparisons were conducted between White adults and individual non-White racial groups (eg, African Americans, Asians, Native Hawaiians, and American Indians) rather than across all groups simultaneously. This approach allowed for focused pairwise comparisons to assess differences in access to surgery relative to the White population. Using the CPT codes, the selected surgeries for analysis were as follows:
By comparing each racial group with the White group, this study highlighted specific disparities in access to GAS that may not have been evident in cross-group comparisons. Figure 1 outlines the organization of our data collection for the study.
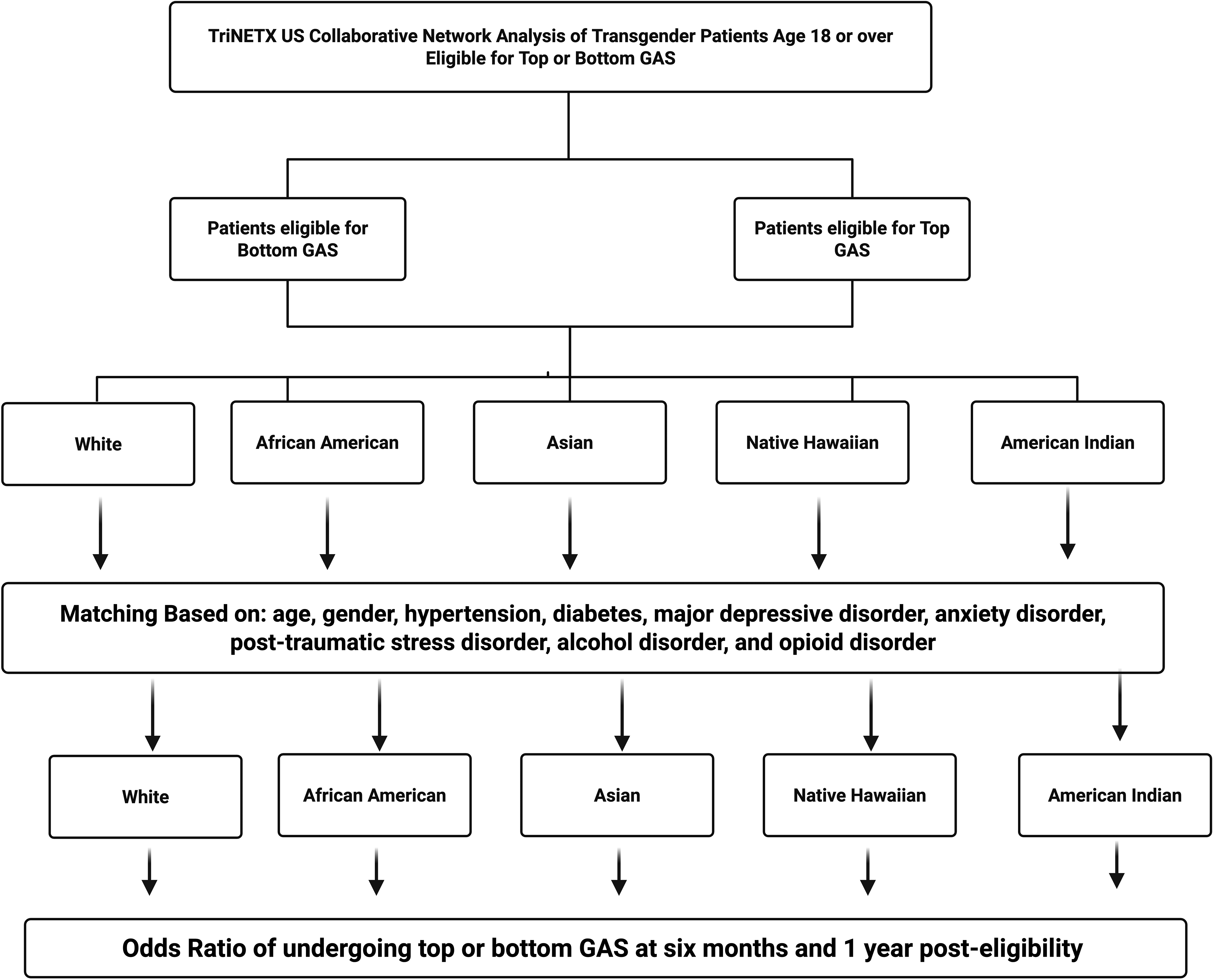
Flowchart of the study design and data collection.
Propensity Score Matching
Propensity score matching (PSM) was employed to adjust for potential confounding factors and ensure comparability between racial groups.9,10,13,14 Patients in each racial group were matched to White patients, the reference group, based on demographic and clinical variables, including age, gender, hypertension (I10), diabetes (E08-E13), major depressive disorder (F33), anxiety disorder (F41.9), post-traumatic stress disorder (F43.10), alcohol dependence (F10), and opioid dependence (F11). This matching process minimized selection bias in the comparisons between racial groups, allowing for more accurate estimates of racial disparities in access to GAS.
Statistical Analysis
We conducted statistical analyses using TriNetX software (TRINETX, LLC, Cambridge, MA), which uses programming languages like JAVA, R, and Python. To assess the relationship between race and the likelihood of undergoing top or bottom GAS, we calculated odds ratios (ORs) with 95% confidence intervals (CIs). A level of P < .05 was used to determine statistical significance. Analyses were conducted at both 6-month and 1-year intervals to evaluate changes over time in GAS utilization across racial groups.
Results
Tables 1 to 5 demonstrates the demographic distributions by race and ethnicity before and after matching. Before propensity score matching, significant differences were observed between White patients and other non-White groups; however, after matching, no significant differences were noted in age, gender, or comorbidities.
Demographics by Race and Ethnicity Before and After Matching White and African American Patients.
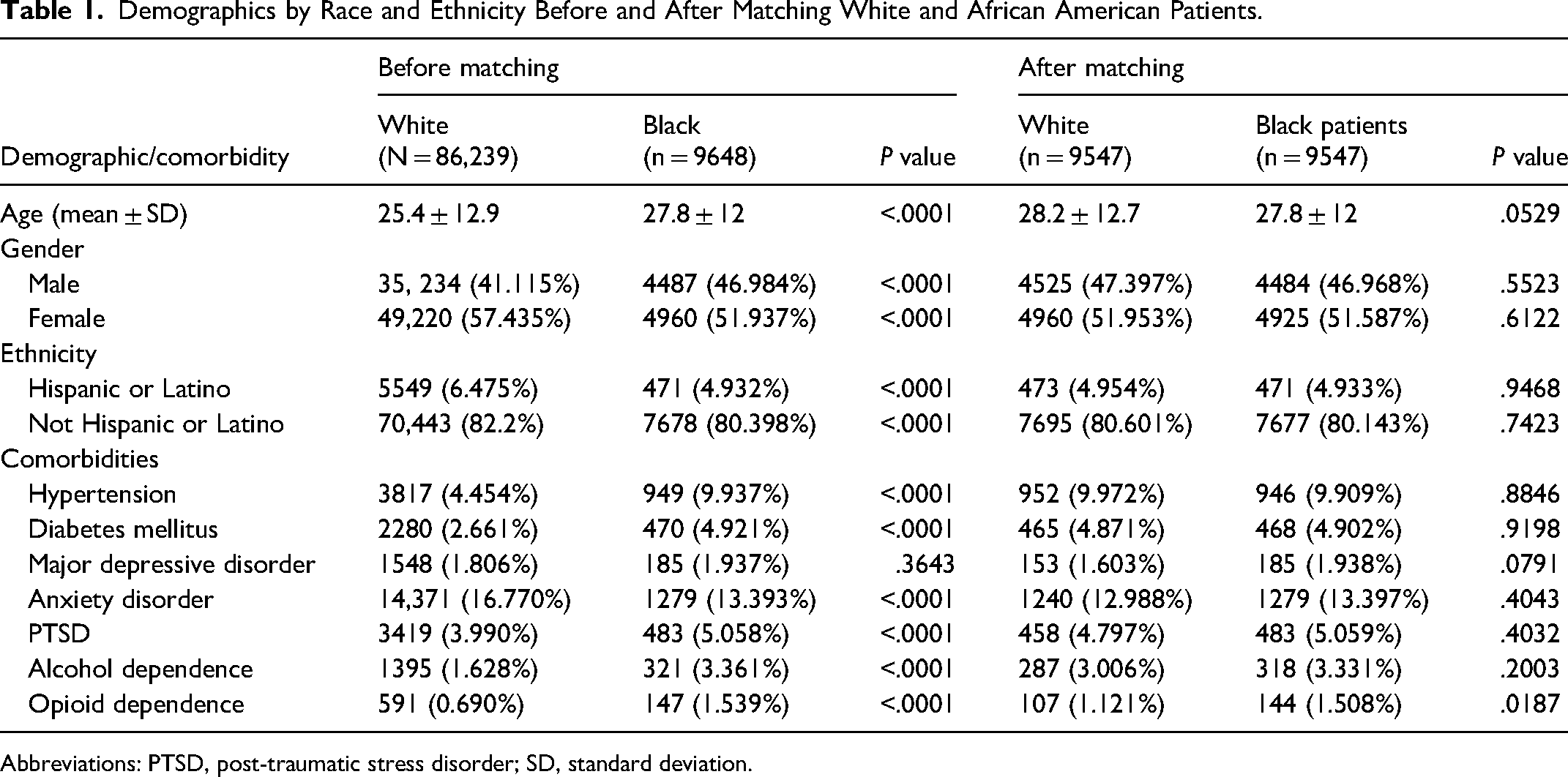
Abbreviations: PTSD, post-traumatic stress disorder; SD, standard deviation.
Demographics by Race and Ethnicity Before and After Matching White and Asian American Patients.
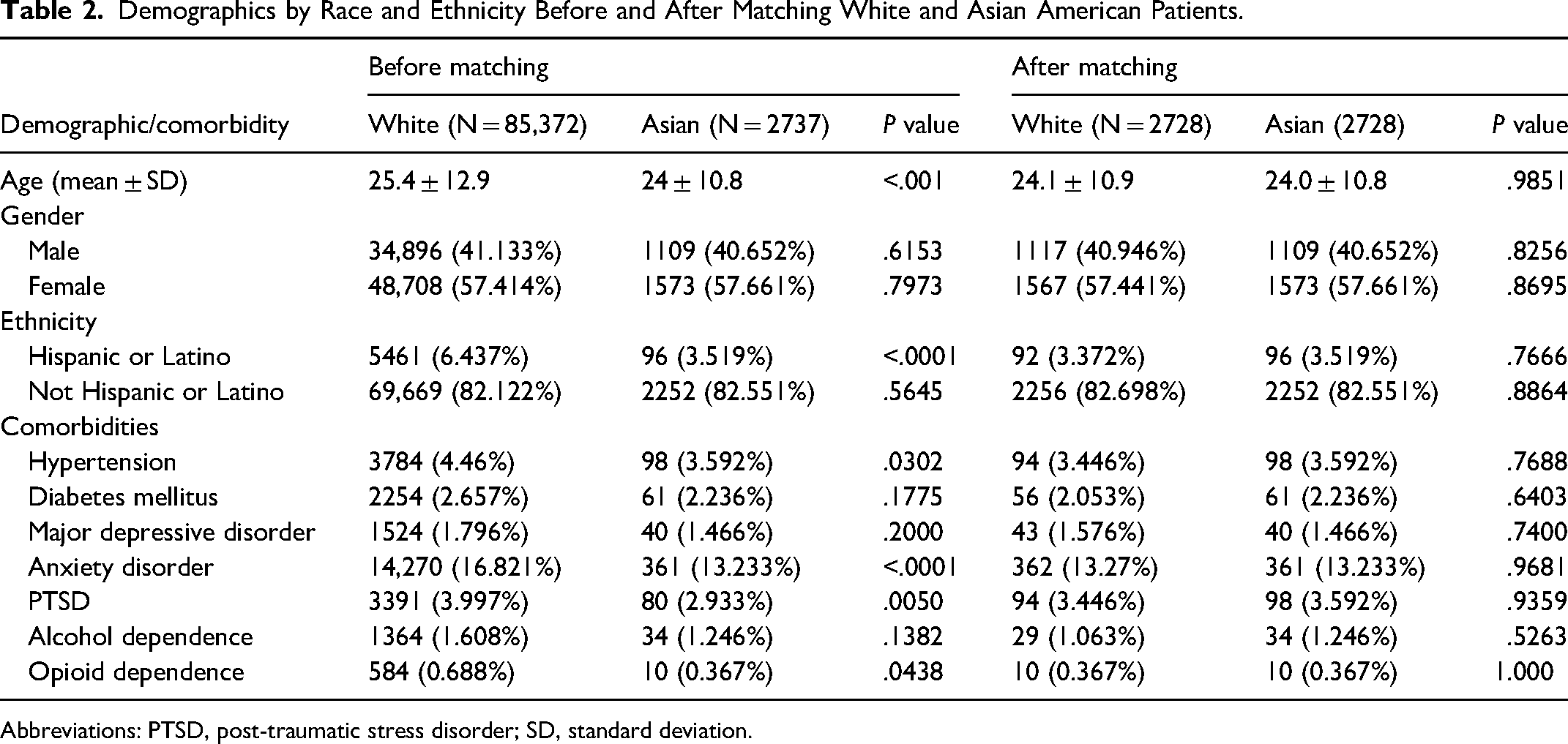
Abbreviations: PTSD, post-traumatic stress disorder; SD, standard deviation.
Demographics by Race and Ethnicity Before and After Matching White and Native Hawaiian Patients.
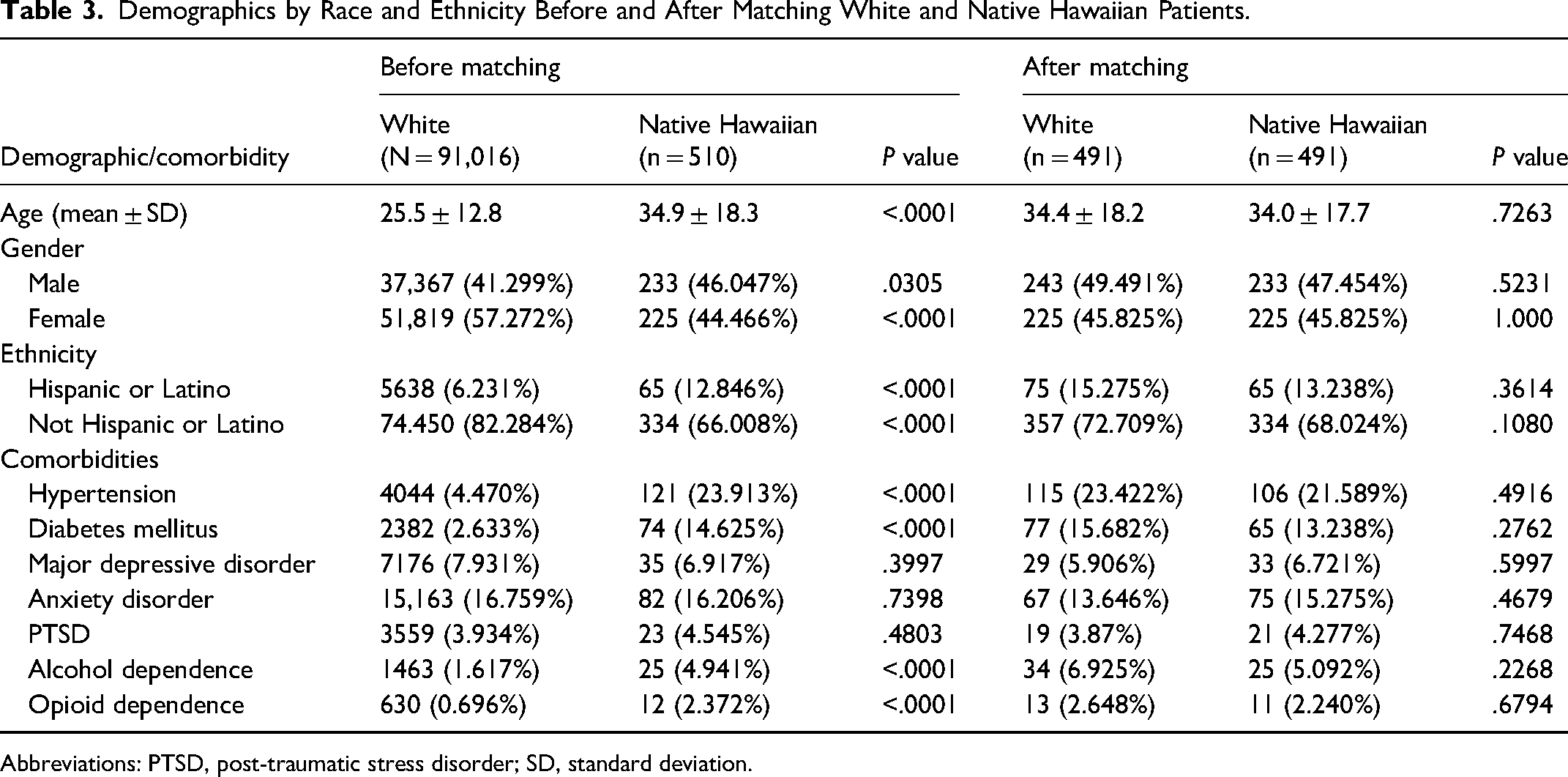
Abbreviations: PTSD, post-traumatic stress disorder; SD, standard deviation.
Demographics by Race and Ethnicity Before and After Matching White and American Indian Patients.
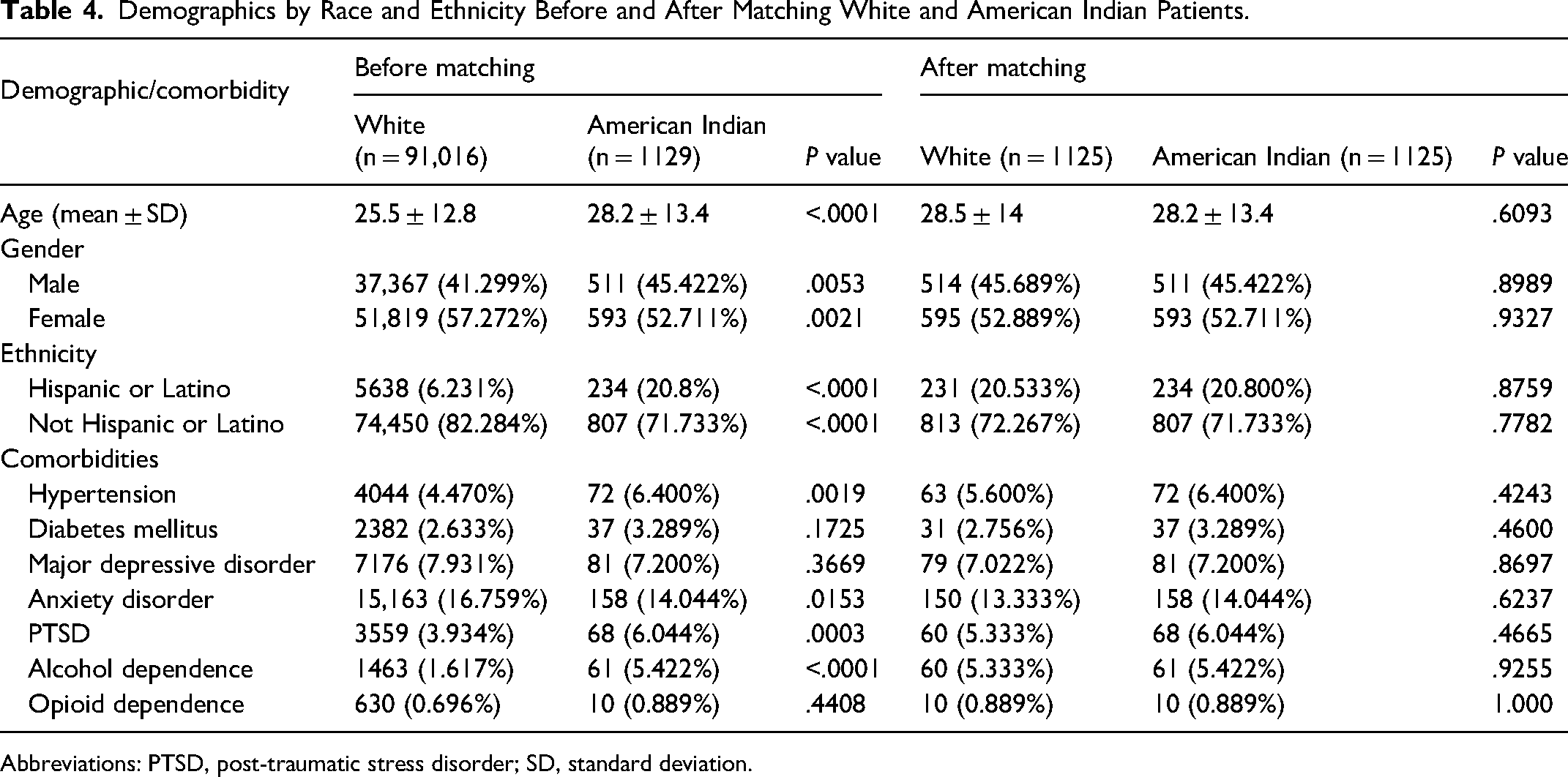
Abbreviations: PTSD, post-traumatic stress disorder; SD, standard deviation.
Demographics by Race and Ethnicity Before and After Matching White and Hispanic Patients.
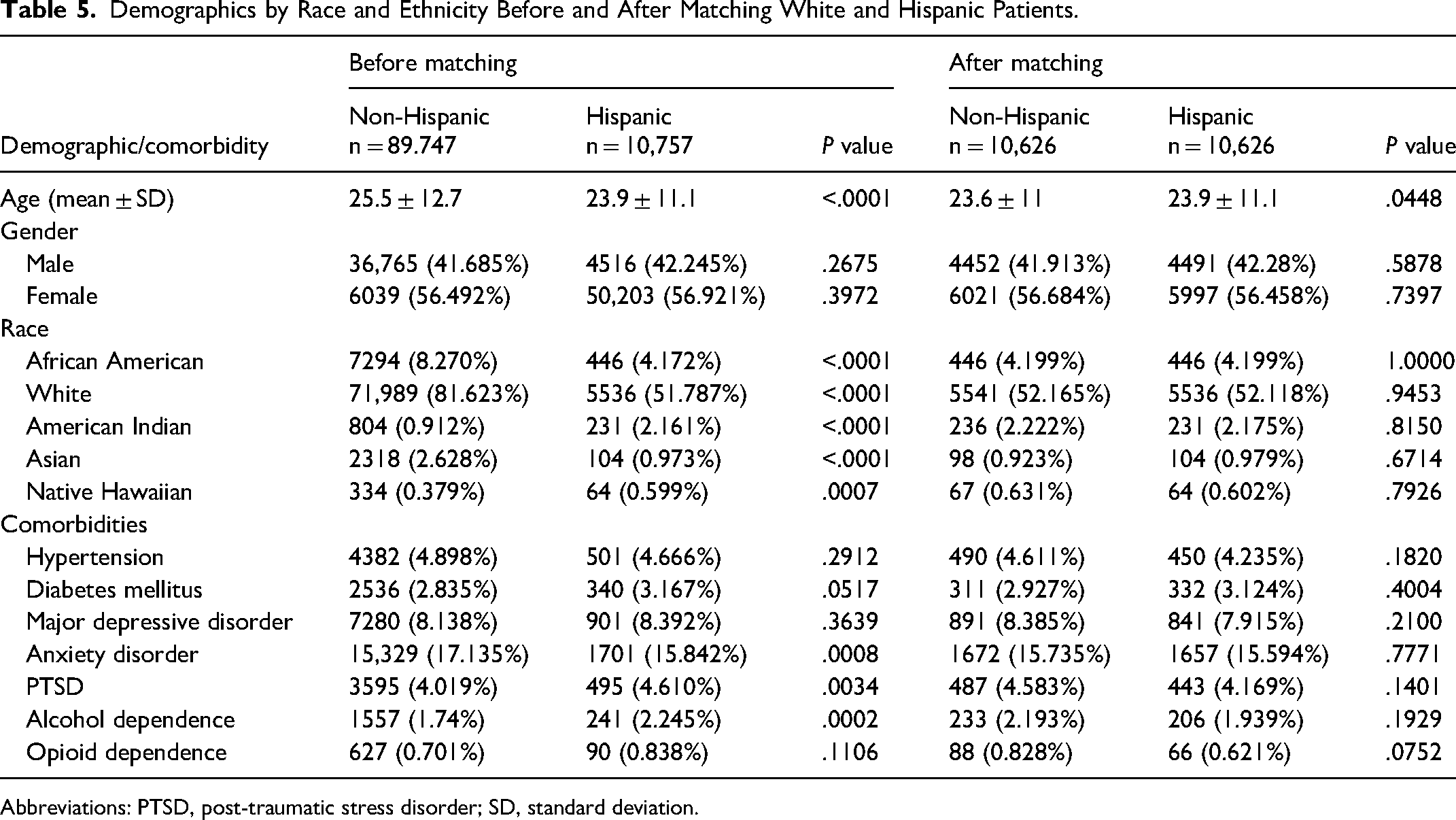
Abbreviations: PTSD, post-traumatic stress disorder; SD, standard deviation.
After matching, the mean age for Black patients (n = 9547) was 27.8 ± 12 years, closely aligned with the reference group. Asian patients (n = 2728) had a mean age of 24 ± 10.8 years, showing no significant difference compared to matched White patients. For Native Hawaiian patients (n = 491), the mean age was 34 ± 17.7 years, and for American Indian patients (n = 1125), it was 28.2 ± 13.4 years, with age disparities balanced after matching. Lastly, Hispanic patients (n = 10,626) had a mean age of 23.8 ± 11.1, showing no significant difference compared to non-Hispanic patients. Gender distributions in each group were similarly aligned with the reference group, and no significant differences in major comorbidities were observed across groups postmatching, highlighting effective demographic balance for comparative analysis.
Six Months
Table 6 presents the odds of receiving top GAS stratified by race after 6 months of being eligible for the surgery. African American patients had lower odds of receiving top GAS compared to White patients (OR = 0.876, P = .0480). Asian patients, however, showed higher odds of receiving top GAS compared to White patients (OR = 1.267, P = .0079). Native Hawaiian and American Indian patients were not statistically different from White patients (OR = 1.086, P = .8479) and (OR = 0.952, P = .8626), respectively. Hispanic patients had lower odds of receiving top GAS than non-Hispanic patients (OR = 0.873, P = .0014).
Odds of Receiving Top Gender-Affirming Surgery (GAS) by Race Within 6 Months.
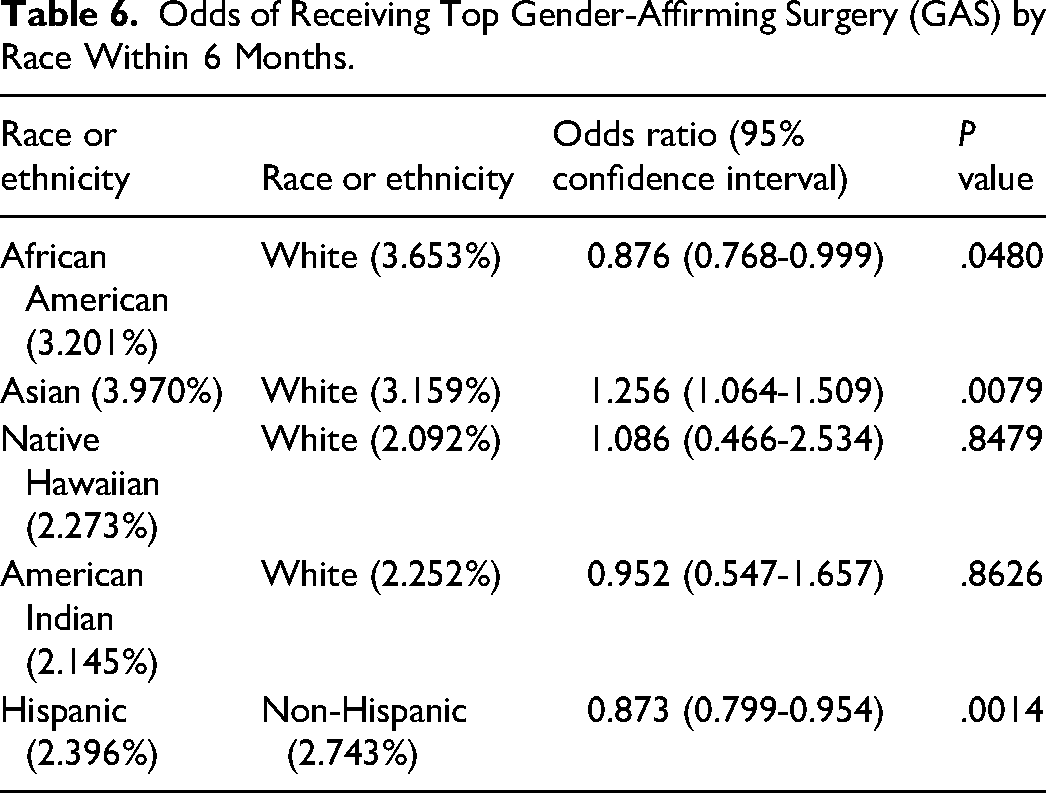
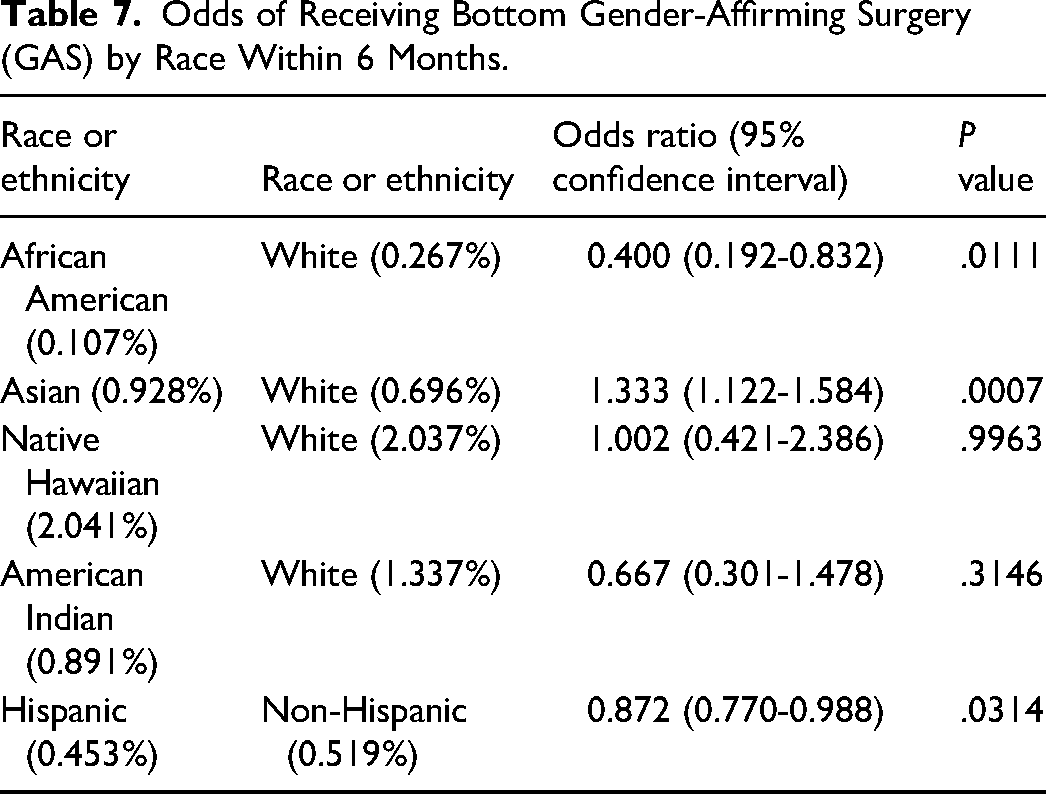
Table 7 outlines the odds of receiving bottom GAS stratified by race after 6 months. African American patients had significantly lower odds of receiving bottom GAS compared to White patients (OR = 0.399, P = .0111). Asian patients had higher odds of receiving bottom GAS compared to White patients (OR = 1.333, P = .0007). Neither Native Hawaiian patients (OR = 1.002, P = .9963) nor American Indian patients (OR = 0.667, P = .3146), had an odds ratio that was statistically significant. Hispanic patients had lower odds of receiving bottom GAS than non-Hispanic patients (OR = 0.872, P = .0314).
Odds of Receiving Bottom Gender-Affirming Surgery (GAS) by Race Within 6 Months.
One Year of Being Eligible
Table 8 shows the odds of receiving top GAS stratified by race after 1 year of being eligible for the surgery. African American patients had significantly lower odds of receiving top GAS compared to White patients (OR = 0.768, P = .0061). Asian patients, however, had higher odds of receiving top GAS compared to White patients (OR = 1.251, P = .0419). Native Hawaiian and American Indian patients had ORs of 0.954 (P = .2283) and 0.863 (P = .4851), respectively, indicating no statistically significant differences from White patients. Hispanic patients had slightly lower odds of receiving top GAS than non-Hispanic patients (OR = 0.913, P = .0005).
Odds of Receiving Top Gender-Affirming Surgery (GAS) by Race Within 1 Year.
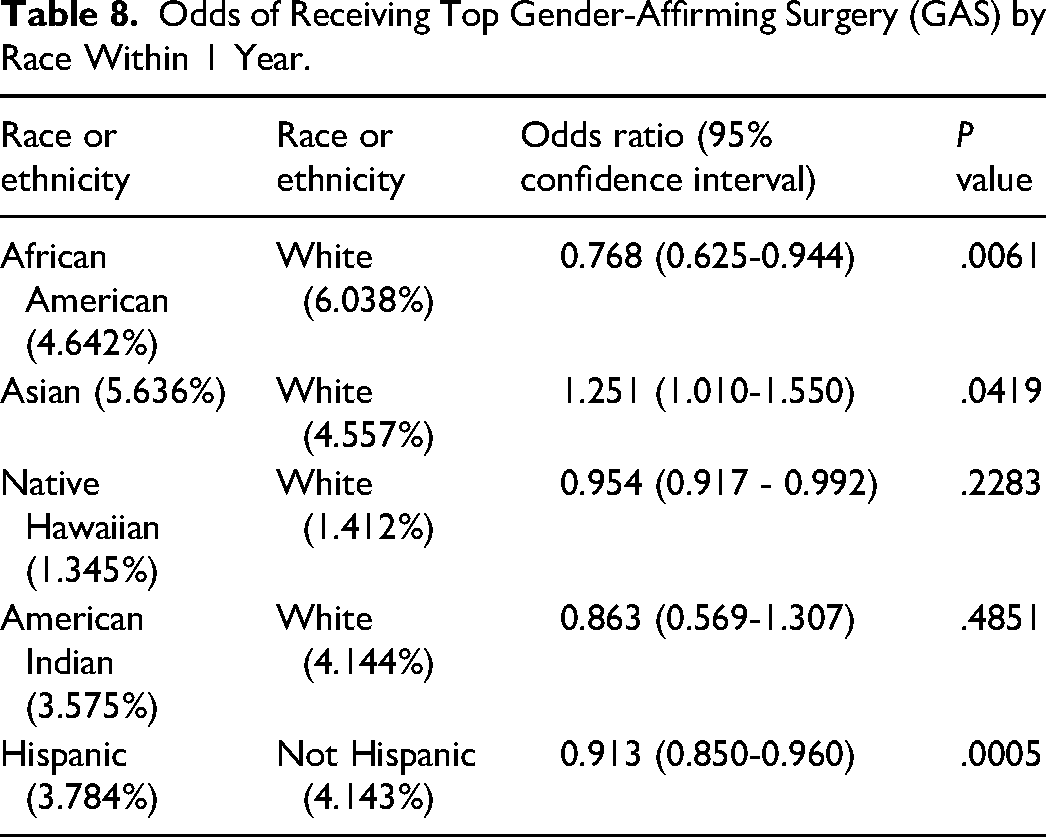
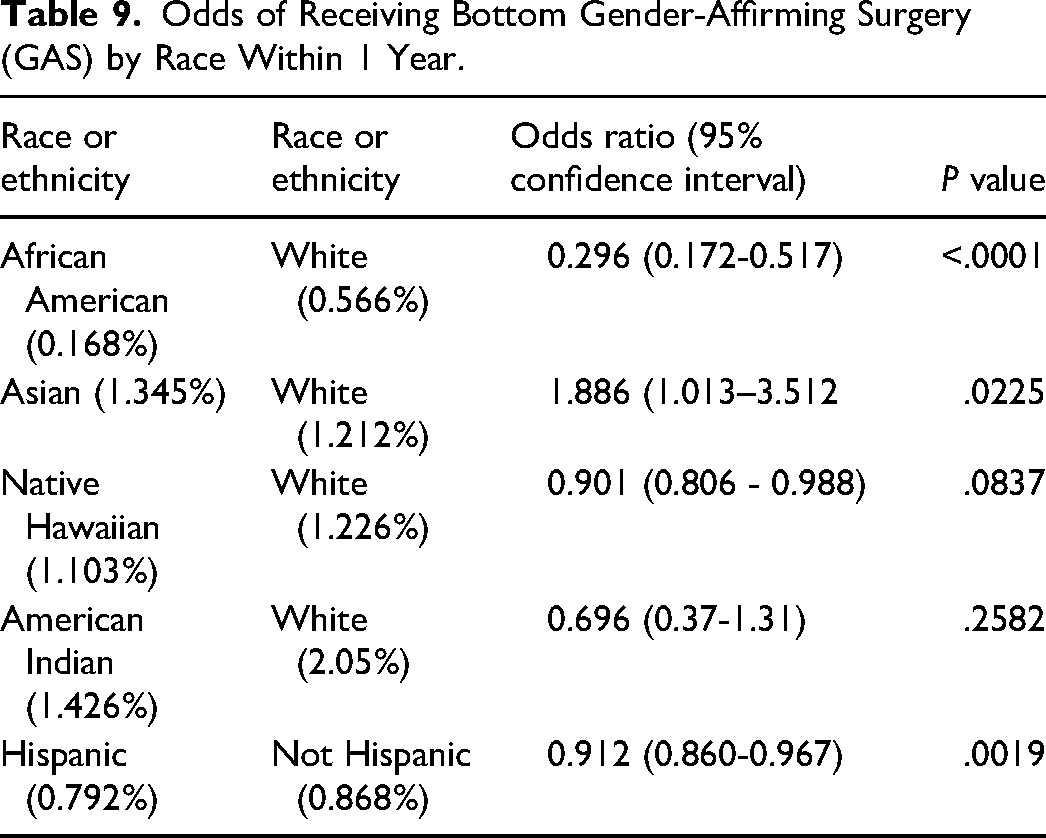
Table 9 presents the odds of receiving bottom GAS stratified by race after 1 year. African American patients had significantly lower odds of receiving bottom GAS compared to White patients (OR = 0.296, P < .0001). Asian patients had higher odds of receiving bottom GAS compared to White patients (OR = 1.886, P = .0225). Native Hawaiian patients (OR = 0.901, P = 0.0837), and American Indian patients (OR = 0.696, P = .2582), were not statistically significant. Hispanic patients had lower odds of receiving bottom GAS than non-Hispanic patients (OR = 0.912, P = .0019).
Odds of Receiving Bottom Gender-Affirming Surgery (GAS) by Race Within 1 Year.
Discussion
This study provides one of the largest national analyses to date examining racial and ethnic differences in the likelihood of receiving GAS after meeting clinical eligibility. By using the TriNetX database and adjusting for relevant clinical variables through propensity score matching, we aimed to describe trends in surgical uptake among transgender individuals of different racial and ethnic backgrounds across US healthcare systems. Our findings demonstrate that, within 1 year of meeting eligibility, African American and Hispanic patients had statistically lower odds of undergoing both top and bottom surgeries compared to White and non-Hispanic patients. Conversely, Asian patients had higher odds of receiving both types of GAS. These results are consistent with earlier research suggesting the presence of racial and ethnic differences in access to or utilization of transgender-related healthcare services.17–20 However, while these disparities are well documented in general healthcare access,3,4 our study adds specificity by focusing on procedural uptake among clinically eligible patients and examining 2 time points (6 months and 1 year) for surgical receipt.
Previous studies examining disparities in gender-affirming care have identified racial and ethnic differences in healthcare utilization, though many have been limited in scope.15,19,21–24 For example, James et al 25 in the US Transgender Survey reported that transgender people of color were significantly more likely to experience denial of coverage for GAS and were less likely to have access to providers with experience in transgender care. Similarly, White Hughto et al 26 found that non-White transgender individuals were less likely to receive gender-affirming surgery compared to White peers, citing structural barriers, provider discrimination, and lack of institutional resources as contributing factors. While these and other studies have been instrumental in identifying disparities, they often rely on self-reported survey data, small regional samples, or aggregate measures of healthcare utilization that do not distinguish between different types of procedures or timing of care.
Our study builds on this existing literature by providing a large-scale, multi-institutional analysis of surgical uptake using a real-world clinical dataset. By examining the odds of undergoing specific GAS at 2 clinically relevant time points, 6 months and 1 year after meeting eligibility, we offer a more granular view of access disparities across racial and ethnic groups. Additionally, our use of propensity score matching to account for demographic and clinical confounders strengthens the internal validity of our comparisons. While we echo previous findings that racial and ethnic disparities exist in gender-affirming care, our study adds to the evidence by quantifying these differences at the procedural level across a national sample, and by demonstrating that these disparities persist even after adjusting for important baseline variables. This reinforces the need to further investigate both structural and individual-level factors that contribute to unequal access, while highlighting the limitations of administrative data in capturing the full complexity of transgender healthcare.
It is important to emphasize that this study identifies associations, not causation. As the trajectory from gender dysphoria diagnosis to GAS is highly individualized, differences in surgical rates may reflect a range of intersecting factors beyond access alone.27–29 Cultural views on gender, variation in transition goals, patient autonomy, perceived risks of surgery, provider recommendations, and systemic barriers such as insurance delays or provider availability could all influence the decision to undergo surgery.30–34 Additionally, some individuals may choose not to pursue GAS for personal or medical reasons, independent of healthcare system constraints.35–39 Given these complexities, our results should not be interpreted as direct evidence that disparities in surgical rates are solely attributable to healthcare inequities. Instead, these trends underscore the need for more nuanced, qualitative, and longitudinal research that can explore how race and ethnicity intersect with gender identity, healthcare access, and surgical decision making.
Study Limitations
While this study's use of propensity score matching allowed for robust analysis, several limitations remain. The reliance on the TriNetX database may introduce selection bias, as it reflects predominantly large healthcare institutions, potentially excluding smaller, rural, or community-based centers where barriers to care may be more pronounced. The use of ICD-10 coding does not fully capture the complexity of gender diversity, including nonbinary identities, and likely excludes patients not undergoing hormone therapy, leading to an underestimation of care needs. Key socioeconomic factors such as income, housing stability, insurance type, and travel costs were not directly measured, despite their critical role in determining access to gender-affirming surgeries. Additionally, cultural and educational influences, which shape attitudes and awareness about gender-affirming care, were not included, leaving gaps in understanding the disparities observed across racial and ethnic groups. Notably, Native Hawaiians and American Indians remain underrepresented in both this study and broader research on gender-affirming care. Future research should prioritize these groups to ensure equitable healthcare delivery and provide deeper insights into the structural, cultural, and economic factors influencing their access to care. Additionally, the ICD-10 codes used to identify gender-diverse patients (eg, “transsexualism” and “dual role transvestism”) reflect outdated terminology as defined by TriNetX and may not align with current affirming clinical language, potentially capturing historic documentation practices or care provided by nonspecialist providers. Furthermore, the lack of self-reported gender identity within TriNetX restricts the ability to accurately identify transgender and gender-expansive individuals, particularly those who may not meet traditional diagnostic or procedural coding criteria. This limitation underscores the urgent need for more inclusive data collection practices across health systems, such as integrating gender identity fields into electronic health records. Improved data granularity would enable future studies to better capture the full spectrum of gender-diverse experiences and healthcare needs. Additionally, while the use of a 6-month duration of hormone therapy aligns with prevailing clinical guidelines, it remains an arbitrary threshold that may not reflect individualized readiness or patient preferences. The restriction to surgeries occurring within 1 year of meeting eligibility criteria likely underestimates true access, as many patients experience delays due to limited surgical provider availability, long institutional waitlists, insurance authorization hurdles, and personal or work-related factors that postpone scheduling. These constraints underscore the need for longitudinal research designs that capture extended care trajectories.
Our study highlights measurable racial and ethnic differences in the odds of receiving GAS within 1 year of eligibility. While causality cannot be established, these findings contribute to the growing body of literature examining disparities in transgender healthcare and reinforce the importance of further research into the multifaceted drivers of these patterns. Future work should prioritize patient-centered investigations, qualitative analyses, and policy-focused studies to better understand and address the complex factors shaping equitable access to gender-affirming care.
Conclusion
As GAS has become an increasingly important aspect of gender-affirming care among transgender individuals, understanding the barriers faced by different racial groups within the transgender community is crucial for reducing healthcare disparities and improving access to care for all transgender individuals. Our results show significant variation in the likelihood of receiving both top and bottom surgeries across various racial groups within the transgender community. Future research should aim to assess interventions to reduce barriers to care for these individuals.
Footnotes
Ethics Approval
This study was IRB exempt from University of Texas Medical Branch Institutional Review Board.
Consent to Publication
Not applicable. This study does not include any individual-level data requiring consent for publication. All authors consent to the study being published.
Authors' Contributions
ARP was involved in conceptualization, data curation, writing—original draft, and writing—review & editing; JEL in conceptualization, writing—original draft, and writing—review & editing; CH, CB, MG, RJH, NH in writing—review & editing; and OI-O in supervision and writing—review & editing. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare that they have no conflicts of interest or competing interests relevant to this work.
Availability of Data
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.