
Abstract
Objective:
To evaluate the effect of different CAD/CAM materials and occlusal thicknesses on the fracture resistance of primary molar crowns.
Methods:
Sixty extracted primary molar teeth were prepared and randomly divided into six experimental groups according to the material and thickness. Primary molar crowns with a central groove thickness of 0.3 and 0.5 mm were fabricated from CAD/CAM zirconia (group Z), zirconia-reinforced lithium silicate (group ZLS), and pre-polymerized composite resin blocks (group C). Each crown was cemented with self-adhesive resin cement on the prepared tooth. All specimens were subjected to fracture tests until fracture. Fracture load values were recorded in Newtons (N). Data were statistically analyzed using a two-way analysis of variance (ANOVA) followed by Tukey multiple comparison test.
Results:
The highest fracture load values were obtained in group Z at 0.5 mm occlusal thickness and were significantly higher compared with the other experimental groups (p < 0.05). Although the lowest fracture load values were obtained in group ZLS at 0.3 mm occlusal thickness, all the tested CAD/CAM primary molar crowns at both thicknesses demonstrated fracture load values exceeding reported chewing force in pediatric patients.
Conclusion:
CAD/CAM primary molar crowns with reduced occlusal thickness may be used for the full-coverage restoration of primary molar teeth.
Introduction
Primary teeth are important for children growth, as they maintaining space for their successors, contribute to phonation and mastication, also guiding on permanent dentition development. Keeping the primary teeth in healthy condition until their successors erupt is significant. 1 Therefore, primary teeth with extensive and multisurface caries lesions, endodontic treatment, fracture, and extensive wear or developmental defects should be restored with full-coverage crowns. 2 For many years, primary teeth with extensive hard tissue loss have been treated with stainless steel crowns (SSCs). 3 SSCs have many advantages, such as durability, adaptability of margins, minimal technique sensitivity and cost-effectiveness.4,5 However, SSCs do not meet the esthetic demands of parents and children. 6
Increasing demands of parents from pediatric dentists to provide more esthetic restorations have resulted in an increase in the usage of tooth-colored restorative material in clinical practice. 7 To overcome the metallic appearance of SSCs, esthetic full-coverage crowns such as pre-veneered SSCs, composite resin strip crowns, and prefabricated zirconia crowns (PZCs) were developed for the primary dentition. Because of their biocompatibility, esthetic, and mechanical features, PZCs are used more widespread in clinical practice. 6 PZCs are highly retentive, biocompatible, providing less plaque accumulation, gingiva-friendly, resistant to fracture, causing less antagonist wear, and well-accepted by parents.8,9 However, PZCs are thicker, can not be crimped or contoured, and require more aggressive tooth preparation, 10 which increases pulp exposure risk.
Restorations fabricated using computer-aided design/computer-aided manufacturing (CAD/CAM) technologies are becoming popular in clinical practice. Currently, CAD/CAM restorations can be fabricated in one session chairside, including full ceramic crowns, inlays, onlays, and veneers. 11 Moreover, they can be used for primary teeth restoration in pediatric dentistry, and can replace SSCs by providing superior esthetics, better marginal adaptation, and parental satisfaction. 12
The durability of crown restorations is equally important as esthetics and can be evaluated by in vitro studies using fracture tests. 13 Fracture resistance refers to the material’s ability to prevent crack growth in regions where stress concentration occurs; this is a significant material’s property because material’s defects are unavoidable in crown processing and fabrication.13,14 These defects have a notch effect promoting stress concentration. Factors including restoration design, tooth preparation, cementation and material thickness affect the fracture resistance of ceramic crowns, and it can be increased by an ideal combination of these factors. 15 However, it is stated that crown material and material thickness are the two most important factors. 16
In various in vitro studies, the fracture resistance of prefabricated or CAD/CAM primary molar crowns were investigated.13,14,17–19 These studies mainly focused on different types of prefabricated primary molar crowns and compared them with each other or pre-veneered SSCs as a control. However, information regarding the effect of different CAD/CAM materials and material’s thickness on fracture resistance in primary molar crowns is insufficient. The fracture resistance of CAD/CAM primary molar crowns with reduced occlusal thickness must be evaluated because preserving tooth structure and making crown restorations durable are both significant.
Therefore, this study aimed to evaluate the fracture resistance of CAD/CAM zirconia, zirconia-reinforced lithium silicate and pre-polymerized composite primary molar crowns with two different occlusal thicknesses.
Methods
Ethical approval was obtained from the Ethics Committee of the Faculty of Medicine, Pamukkale University (No. 60116787-020/50343; 25.08.2020). The sample size was determined using the G*Power 3.1. software (University of Kiel, Kiel, Germany) with a significance level of 5%, power of 80%, and 1.32 effect size. 20 The power calculation indicated that a sample size of at least 10 samples for each group were required.
Specimen collection and preparation
Sixty freshly extracted primary mandibular second molars were used in this study. Extraction was performed due to eruption guidance or ectopic eruption of successors, not based on the purpose of the study. Patients’ parents/legal guardians were informed, and written informed consent was obtained for this study. Caries free, intact crowns with sufficient root length for retention in acrylic resin, and teeth with similar crown dimensions (±1 mm) were included. All the teeth were kept in 0.1% thymol solution at 4°C until testing.
Each tooth was cemented in cylindrical polyethylene blocks (25 mm in diameter and 35 mm high) using autopolymerized acrylic resin (Imicryl, Konya, Turkey) up to 1 mm below the cemento-enamel junction. Then, the teeth were randomly allocated into three groups regarding the type of CAD/CAM restorative materials as follows: (1) CAD/CAM zirconia (inCoris TZI, group Z): 0.3 mm (n: 10)/0.5 mm (n: 10), (2) CAD/CAM zirconia-reinforced lithium silicate (Celtra Duo, group ZLS): 0.3 mm (n: 10)/0.5 mm (n: 10), and (3) CAD/CAM pre-polymerized composite resin (Brilliant Crios, group C): 0.3 mm (n: 10)/0.5 mm (n: 10) (Table 1).
Tested CAD/CAM materials.
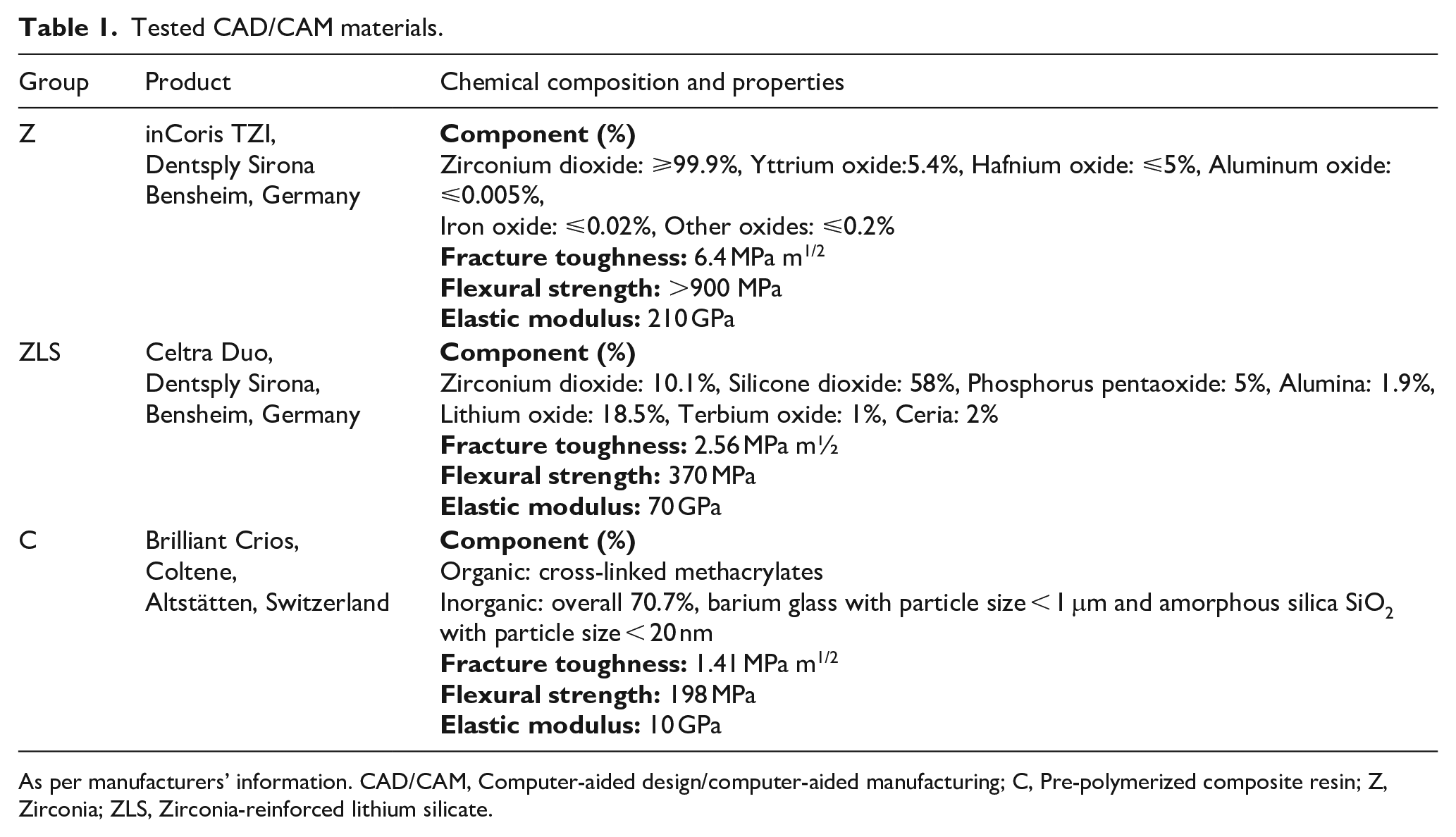
As per manufacturers’ information. CAD/CAM, Computer-aided design/computer-aided manufacturing; C, Pre-polymerized composite resin; Z, Zirconia; ZLS, Zirconia-reinforced lithium silicate.
The specimens were prepared with high-speed diamond burs (Dia-Burs TF-21, ISO 171/016 FG, Mani Inc, Utsunomiya, Japan & Diamond 833 G.FG.023, Jota AG, Rüthi, Switzerland) under water cooling by the same investigator. Tooth preparation was applied to all teeth specimens with 1 mm occlusal and 0.8 mm circumferential reduction, creating 0.5 mm gingival chamfer and a convergence angle of 6°–8° without any undercut remaining.
Fabrication of CAD/CAM primary molar crowns
The prepared teeth were scanned with CEREC Primescan (Sirona Dental Systems GmbH, Bensheim, Germany), and then full-crown restoration designs were made using CEREC AC Acquisition Unit using CEREC 5.2.2 software (Sirona Dental Systems GmbH, Bensheim, Germany). Permanent mandibular first molar forms were referenced because of their similarity to primary second molar forms. Restoration parameters were set to 80 µm for cement space, and all other parameters were set to 0 µm. Then, the occlusal thickness of the CAD/CAM primary molar crowns was determined with software by virtually reducing the occlusal surface in the central groove area until the tested thickness (0.3 or 0.5 mm) was obtained (Figure 1). Each crown was designed according to Tooth DB, Candulor, and Bonartic design technique using CEREC 5.2.2 software (Sirona Dental Systems GmbH, Bensheim, Germany) because of their similarity to primary second molars morphologies.
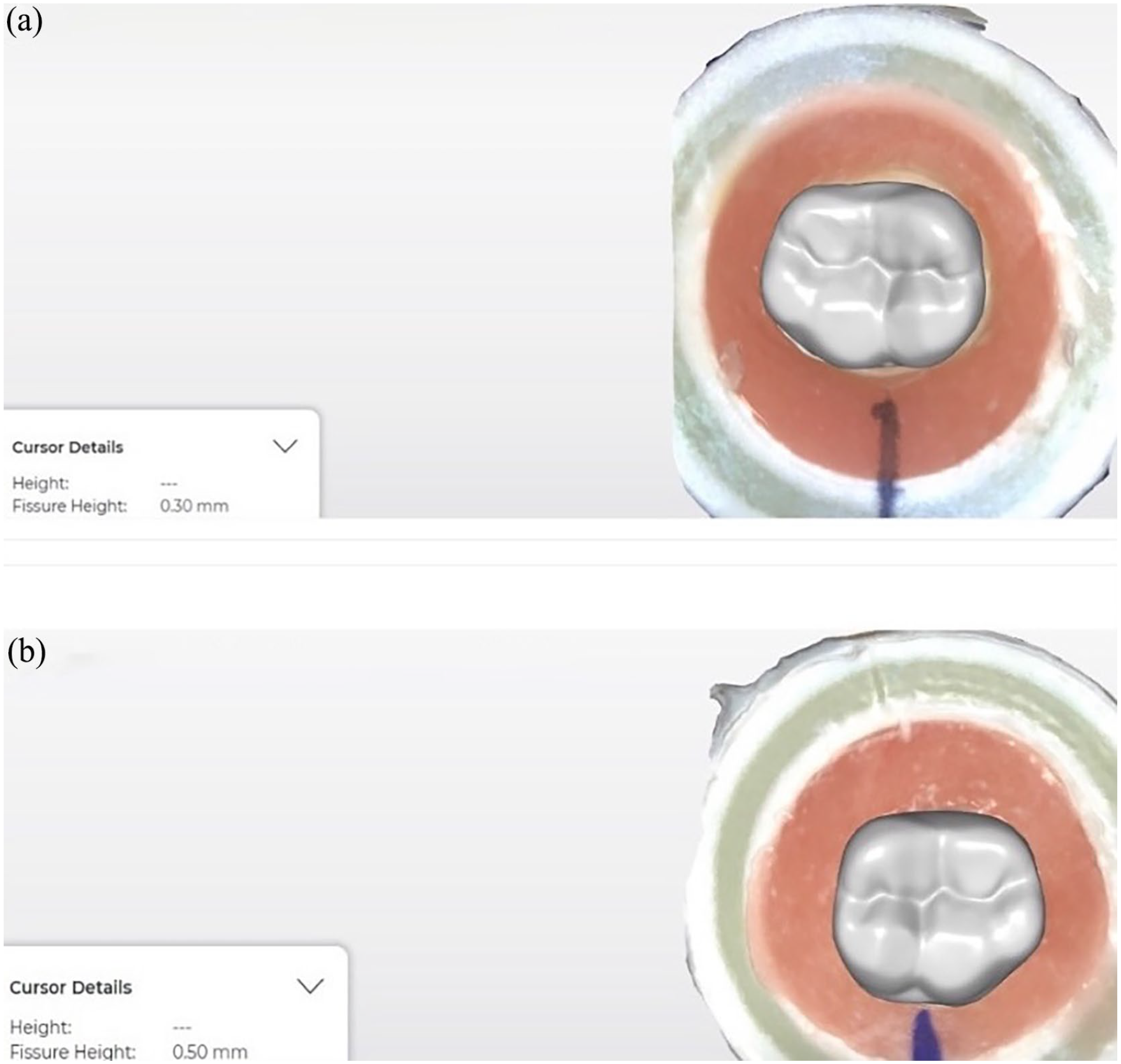
Restoration design: (a) Group Z with 0.3 mm occlusal thickness and (b) Group Z with 0.5 mm occlusal thickness.
After the restoration design was completed, 60 crowns (n: 10, per group) were fabricated from inCoris TZI (Dentsply Sirona, Bensheim, Germany), Celtra Duo (Dentsply Sirona, Bensheim, Germany), and Brilliant Crios (Coltene, Whaledent AG, Altstätten, Switzerland) blocks using a four-axis chairside milling machine (CEREC MC XL; Sirona Dental Systems GmbH, Bensheim, Germany). Following milling procedures, group Z and ZLS crowns were crystallized in a ceramic furnace (CEREC SpeedFire; Sirona Dental Systems GmbH, Bensheim, Germany) in accordance with the manufacturers’ instructions. For group C, the crowns were air-abraded with 50 µm aluminum-oxide powder (Duradent; Erk Dental, İzmir, Turkey) at 2 MPa pressure and ultrasonically cleaned. Before cementation, each crown was checked for proper fit between the crown, prepared tooth, and any defects. In case of discrepancy or any detectable defects, the prepared tooth was rescanned, and a new crown was fabricated.
Cementation of CAD/CAM primary molar crowns
Fabricated crowns were cemented to the corresponding teeth with a self-adhesive resin cement (Calibra Universal; Dentsply Sirona, York, PA, USA) according to manufacturer’s recommendations, then photopolymerized (Elipar Deep Cure-S curing light; 3 M ESPE, St. Paul, MN, USA) for 40 s from each side with 1470 mW/cm2 light intensity. All specimens were kept in distilled water at 37°C until the fracture test.
Fracture load tests
A universal testing machine (Esetron Smart Robotech-nologies, Ankara, Turkey) was used for fracture tests. The load was applied using a 5 mm rounded stainless steel tip placed in the central groove area and subjected to increasing vertical load at 0.5 mm/min crosshead rate (Figure 2). The mechanical test was stopped as fracture occurred, and the corresponding maximum load value was recorded in Newtons (N).
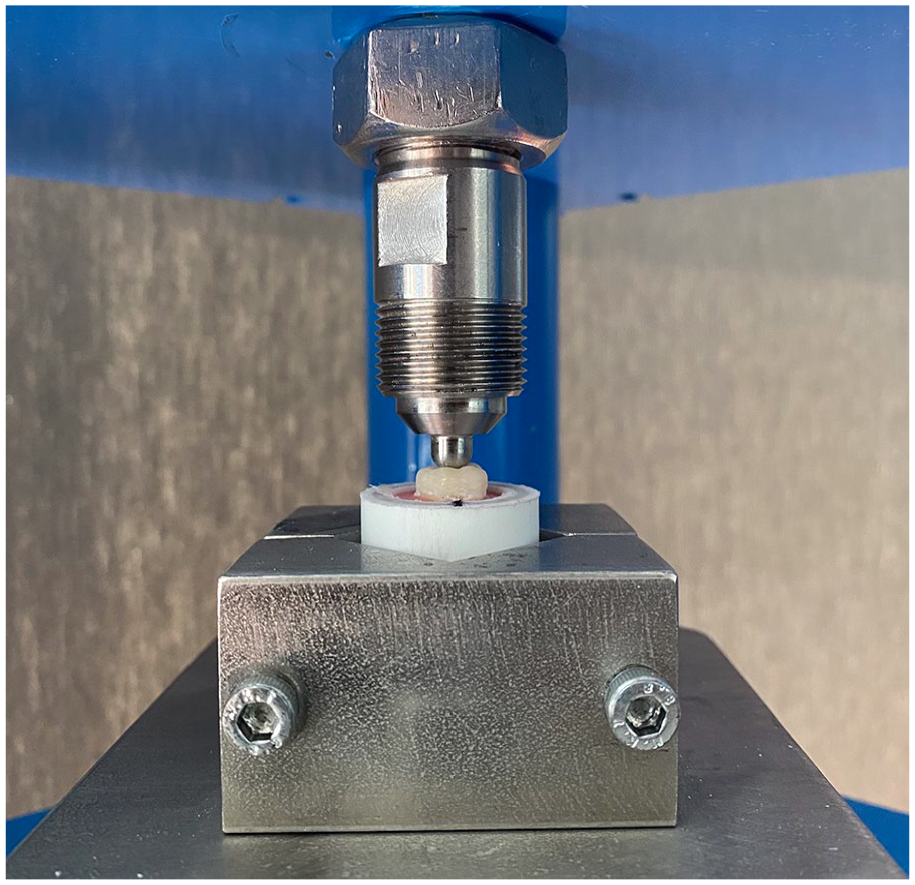
Mounted specimen in the universal testing machine.
Statistical analysis
The obtained data were analyzed with SPSS 15.0 software (SPSS Inc, Chicago, IL, USA). The normality of distribution was tested using the Shapiro-Wilk test. The fracture load values were analyzed considering two parameters (occlusal thickness and material type) using the two-way analysis of variance (ANOVA), then Tukey multiple comparison test was carried out to evaluate differences among the testing groups (significance level 0.05).
Results
Descriptive statistics for the fracture load values in each group are shown in Table 2. For 0.3 mm thickness, a statistically significant difference was observed among the mean fracture load values of groups Z, ZLS, and C (p < 0.001). For materials effect on fracture load, group Z (1315.6 ± 290.8 N) showed higher fracture load values than in group ZLS (686.0 ± 117.0 N) and group C (761.1 ± 208.7 N) (p < 0.001). There was no significant difference in the fracture load values between the groups ZLS and C (p = 0.723).
Load to fracture for each group (N).
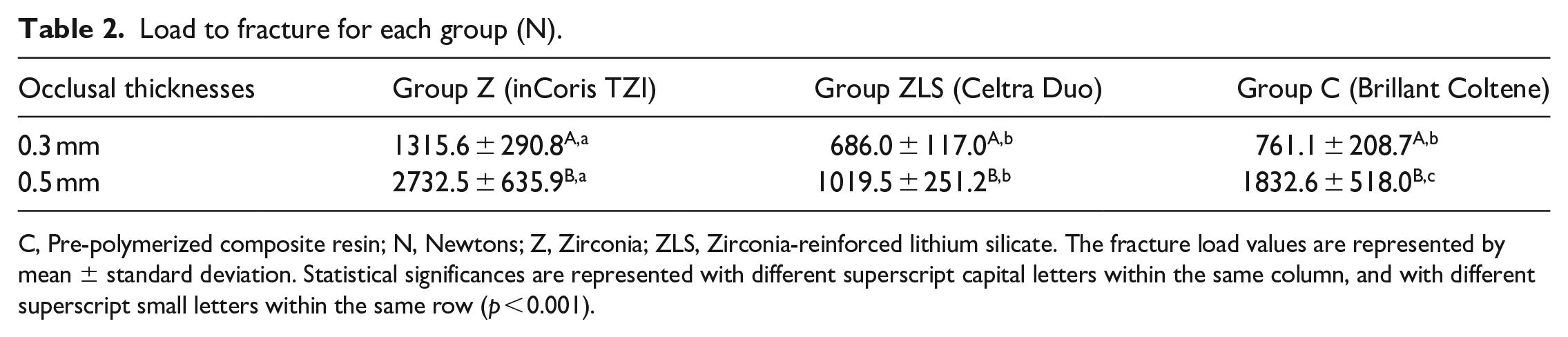
C, Pre-polymerized composite resin; N, Newtons; Z, Zirconia; ZLS, Zirconia-reinforced lithium silicate. The fracture load values are represented by mean ± standard deviation. Statistical significances are represented with different superscript capital letters within the same column, and with different superscript small letters within the same row (p < 0.001).
For 0.5 mm thickness, there were significant differences among the mean fracture load values of groups Z, ZLS, and C (p < 0.001). Group Z showed the highest fracture load values (2732.5 ± 635.9 N) compared with group ZLS (1019.5 ± 251.2 N) and group C (1832.6 ± 518.0 N) (p < 0.001). The mean fracture load values of group C were significantly higher than those of group ZLS (p < 0.05).
For the thickness effect on the fracture loads, all groups showed significantly higher load values to fracture for 0.5 mm than with 0.3 mm occlusal thickness. The two-way ANOVA test indicated that occlusal thickness, material type, and occlusal thickness × material type interaction (p = 0.0001) significantly affect fracture loads.
Discussion
The improvements in computerized dentistry and new adhesive materials have contributed to ultraconservative dentistry development. This allows the fabrication of ultrathin esthetic crown restorations, which provide esthetic and conservative results. 21 CAD/CAM technology is a novel method for primary teeth restorations. In contrast to PZCs which require aggressive tooth preparation for passive fit of the crown to the tooth, no additional tooth preparation is required for CAD/CAM primary molar crown and it may fit better on prepared tooth. 14 Therefore, when the full-coverage restoration is required for pediatric patients, CAD/CAM primary molar crowns can be considered an esthetic and conservative alternative because they require less tooth preparation.
However, crown thickness has a significant effect on restoration stability. 21 Furthermore, reduced thickness of occlusal ceramic may affect the stability, resistance, and longevity of dental restorations.20–22 Therefore, the fracture resistance of CAD/CAM primary molar crowns with reduced occlusal thicknesses needs to be tested because crown material longevity is highly associated with its mechanical properties. 14
There is not enough information in the literature regarding the fracture resistance of primary molar restored with reduced occlusal thickness CAD/CAM crowns. This study included 0.3 and 0.5 mm occlusal thicknesses. The 0.5 mm thickness was chosen because the mean occlusal thickness of the PZCs ranged between 0.5 and 0.73 mm. 23 The 0.3 mm occlusal thickness was chosen to compare with a minimally invasive thickness.
Oğuz et al. 13 investigated the fracture resistance of CAD/CAM zirconia, three different esthetic crowns, and PZCs as a control. According to their results, CAD/CAM zirconia crowns (1126 N) showed significantly higher fracture resistance than PZCs (557 N). They stated that the difference between the fracture loads of CAD/CAM zirconia and PZCs might have derived from the differences in axial and occlusal thicknesses, which were higher for CAD/CAM zirconia crowns compared to PZCs. Townsend et al. 17 investigated the fracture resistance of commercially available PZCs (EZ Pedo, Kinder Krowns, and NuSmile) and pre-veneered SSCs as a control. They reported a significant difference in the highest average occlusal thickness (range between 0.5 and 0.7 mm) of PZCs among three different brands, and Ez Pedo crowns (1091 ± 146.5 N) had the highest fracture load among tested PZCs due to increased crown thickness.
It is stated that the fracture loads of all-ceramic restorations applied in the posterior region determine the success of the treatment to resist chewing forces. 24 Braun et al. 25 reported that the means of maximum chewing force in 6–8 years old children was 78 N and up to 106 N for 10–12 years old children in the primary molar region. Owais et al. 26 reported that the means of maximum chewing force was 433 N in late mixed dentition. This study found that all the investigated CAD/CAM primary molar crowns had higher fracture load values than previously mentioned chewing forces.
A review of the literature did not reveal any studies regarding the effect of different CAD/CAM materials and their thicknesses on the fracture resistance of primary molar crowns. However, the results of the present study were in agreement with previous studies to some extent, which reported that CAD/CAM permanent molar crowns’ fracture resistance are related to their material and/or thicknesses.20,24,27,28 Nakamura et al. 27 evaluated the influence of material thicknesses (0.5, 1, and 1.5 mm) on the fracture resistance of CAD/CAM zirconia permanent molar crowns and compared them with lithium disilicate crowns of a usual thickness (1.5 mm). They found a strong relationship between occlusal thickness and fracture load of zirconia crowns and stated that limiting the occlusal reduction would preserve the sound tooth structure and ensure sufficient height of the axial walls of the abutment tooth, which promote restoration’s retention and resistance. 27 Moreover, for adhesively bonded zirconia crowns without aging, Weigl et al. 20 found a mean fracture load of 1628 ± 174 N with 0.5 mm thickness, and 1164 ± 334 N with 0.2 mm thickness respectively. Choi et al. 24 reported that reduced occlusal thickness influence the fracture load values of zirconia-reinforced lithium disilicate crown, which is the same material (Celta Duo) tested in this study. They found higher fracture load values (1467.1 ± 166.1 N) compared to this study. A possible explanation to that could be the fact that the differences in using supporting die material, test design and material thickness between their study and the present study.
Because different studies have evaluated different preformed crowns or CAD/CAM materials, cement or techniques (supporting die material, thickness of cement space, fracture test device etc.), direct comparison of their results is difficult. This study showed that occlusal thickness and material type had significant effect on the fracture resistance of CAD/CAM primary molar crowns. For the groups with the same thickness (Table 2), fracture load values were significantly higher in group Z than in groups ZLS and C. This can be referred to the zirconia’s superior mechanical properties, such as high fracture toughness (6.4 MPa m1/2) and high flexural strength (>900 MPa), which are superior to the other evaluated materials in the present study (Table 1). 28 A polycrystalline phase transformation system of zirconia gives the material high mechanical strength and enables it to resist chipping or fracture under function.27,28 The results of the present study were in agreement with the previous studies comparing the fracture resistance of CAD/CAM zirconia or composite crowns and noted that crowns fabricated with zirconia showed the highest fracture load values.28,29
Regarding 0.5 mm occlusal thickness, group C (1832.6 ± 518.0 N) showed significantly higher fracture load values than group ZLS (1019.5 ± 251.2 N). Although no statistical significance was observed compared with the group ZLS (686.0 ± 117.0 N), group C (761.1 ± 208.7 N) showed higher fracture load values for 0.3 mm occlusal thickness. Interestingly, group C showed higher fracture load values than group ZLS in spite of its lower flexural strength comparing zirconia-reinforced lithium silicate evaluated in group ZLS (Table 1). According to this result, it can be concluded that the flexural strength value of brittle materials, including glass ceramics, should not be solely relied on to estimate their structural performance because the material’s strength is more “conditional” instead of an inherent property.28,30
CAD/CAM composites have superior mechanical properties than traditional restorative composites because they are polymerized at high pressure and temperatures. Additionally, compared to ceramics, the low elastic modulus may make CAD/CAM resin composites a preferred material under high occlusal loads. 31 Brilliant Crios used in this study is a pre-polymerized composite resin block and has a comparatively low elastic modulus (10 GPa, Table 1) close to that of primary tooth dentin (11.59–17.06 GPa). 32 According to Jassim and Majeed, 28 this allows the materials to plastically deform to the same extent as the underlying dentin, resulting in loads being transferred to the underlying dentin instead of accumulating in the restoration. Moreover, CAD/CAM composite materials exhibit reduced brittleness, increased flexibility, and the ability to absorb stresses caused by the increased loads. 22 Compared to the ZLS group, the higher fracture load values of group C at both occlusal thicknesses could be attributed to these properties of Brilliant Crios.
Previous studies have used different supporting dies such as methacrylate resin, 15 epoxy resin,13,17 Cr-Co metal alloy, 19 or natural teeth14,18,21,28 for evaluating fracture resistance of restorative materials. Yucel et al. stated that elastic modulus of supporting die materials affected the fracture resistance of all-ceramic restorations. 33 If supporting dies exhibit higher elastic modulus than dentin, higher load values can be obtained in in vitro studies than in clinical conditions.33,34 Therefore, natural teeth were used as supporting dies to obtain relevant fracture load values comparable with the clinical conditions in this study.
May et al. 35 stated that cementation method and cement thickness can affect the fracture resistance of CAD/CAM restorations. Adhesive cementation provided increased fracture load values compared to conventional cementation technique20,22 because adhesive cementation allows close contact between dental substrate, cement, and restorative material so that the occlusal loads applied on the restorative material can be distributed through the tooth, periodontal ligament and alveolar bone.36,37 In this study, cement space (80 µm) was standardized for all the investigated CAD/CAM primary molar crowns, and they showed higher fracture load values than reported chewing forces in pediatric patients. These results can be attributed to the adhesive cementation technique, and if this study was performed with the conventional cementation technique, the results could be expected to change. Therefore, further studies comparing adhesive cementation and conventional cementation techniques would be valuable. Moreover, it is acknowledged that the residual strength of sound teeth and restored teeth is reduced by cyclic loading. 38 Gallicchio et al. 38 investigated the fracture resistance and failure modes of endodontically treated maxillary premolars restored with three different fiber posts subjected to cyclic fatigue. Although specimens were not subjected to cyclic loading in this study, the mean fracture load of primary molars restored with CAD/CAM crowns except 0.5 zirconia crowns was lower than sound teeth (1909 ± 177 N) of their study. These differences could be attributed to the methodological differences between their study and the present study.
This study had a few limitations. Although carefully selected, ensuring standardization is difficult because primary molar teeth used as supporting dies might have morphological and hydroxyapatite structure variations. Only axial load was applied to the tested material; however, cyclical or multiaxial loading and lateral forces which occurred in the oral environment were not simulated. In this study, fracture tests were performed without thermo-cycling or cyclic loading. It is stated that aging procedures can affect the fracture resistance of restorative materials. 39 For this reason, further studies are required to evaluate if CAD/CAM ceramic and pre-polymerized composite primary molar crowns can exhibit sufficient fracture resistance following these types of aging procedures. Although the fracture test results obtained in this study are not sufficient to demonstrate the long-term clinical performance, they offer useful knowledge and comparison about the tested dental materials or thicknesses.
Conclusion
CAD/CAM primary molar crowns fabricated with zirconia showed the highest fracture resistance at both thicknesses. Occlusal thickness had a significant impact on the fracture resistance of the tested dental materials. At both thicknesses, the fracture resistance of all the tested CAD/CAM primary molar crowns exceeded the reported chewing force in pediatric patients.
CAD/CAM zirconia, zirconia-reinforced lithium silicate, and pre-polymerized composite primary molar crowns with 0.3 mm occlusal thickness can offer a conservative alternative for primary teeth requiring full coronal coverage. However, further studies are necessary to confirm the clinical success.
Research Data
sj-xlsx-1-jbf-10.1177_22808000241235994 – Supplemental material for Fracture resistance evaluation of CAD/CAM zirconia and composite primary molar crowns with different occlusal thicknesses
sj-xlsx-1-jbf-10.1177_22808000241235994 for Fracture resistance evaluation of CAD/CAM zirconia and composite primary molar crowns with different occlusal thicknesses by Arif Bolaca and Yıldırım Erdoğan in Journal of Applied Biomaterials & Functional Materials
Footnotes
Acknowledgements
The authors would like to thank Dr. Esra Erdoğan for providing the technical support to fabricate the CAD/CAM primary molar crowns used in the present study.
Author contributions
AB and YE researched literature and conceived the study. AB was involved in protocol development, gaining ethical approval, prepared the specimens and performed the experiments, YE fabricated CAD/CAM primary molar crowns, analyzed the data. AB wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Research Projects Coordination Unit of Pamukkale University, Denizli, Turkey (grant number 2020/BSP021).
Guarantor
AB.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.