
Abstract
Objective:
Non-carious cervical lesions (NCCLs) are commonly observed in clinical dentistry, leading to tooth fractures, sensitivity, and compromised pulp vitality. Therefore, their restoration is essential for both the aesthetic and structural integrity of teeth. This study aimed to compare the fracture resistance of NCCLs restored using different materials: an injectable universal composite, flowable bulk-fill composites with or without fiber-reinforcement.
Methods:
Seventy-five double-rooted maxillary premolars were selected for the study. Fifteen teeth were left intact as a control. A wedge-shaped cavity was prepared in the cervical region of the remaining sixty teeth, which were then divided into four groups (n = 15): unrestored, restored with an injectable composite, restored with a flowable bulk-fill composite (SDR® flow+), and restored with a flowable short-fiber-reinforced composite (everX Flow™). All teeth underwent fracture testing under oblique static loading at a 30° angle using a universal testing machine. Fracture patterns were classified as repairable, possibly repairable, or unrepairable. Data were analyzed using one-way analysis of variance, Pearson chi-square, and Tukey HSD post hoc tests (p = 0.05).
Results:
Intact teeth exhibited the highest fracture resistance (743.481 N), while unrestored teeth showed the lowest (371.49 N) (p < 0.001). There was no significant difference in fracture resistance between the injectable composite (553.289 N) and SDR® flow+ (497.368 N) (p = 0.055). The everX Flow™ group displayed significantly higher fracture resistance (673.787 N) (p < 0.001) and a repairability rate of 60% within the restored groups. Unrestored (60%), injectable composite (53.3%), and SDR® flow+ (53.3%) groups were mostly unrepairable.
Conclusion:
The everX Flow™ demonstrated improved fracture resistance and favorable fracture pattern for maxillary premolars with wedge-shaped NCCLs.
Keywords
Introduction
Non-carious cervical lesions (NCCLs) are characterized by the loss of mineralized dental tissue without bacterial involvement. They are typically located at the cementoenamel junction (CEJ) and extend along the tooth surface near the gingival margin. 1 A systematic review reported that NCCLs occur in 40%–60% of adults, depending on age and geographical location. 2 These lesions are frequently observed on the facial surfaces of teeth, particularly maxillary premolars. 3 The development of NCCLs is generally attributed to a combination of factors, such as biocorrosion, abfraction, attrition, and the effects of saliva. 4 NCCLs will continue to progress if left untreated, despite their non-carious nature. 5 These lesions, characterized by the loss of the enamel and dentin structure can lead to tooth sensitivity while lesions can compromise pulp vitality. 6 Restoring deep NCCLs is necessary not only for aesthetic reasons, but also to preserve the tooth’s structural integrity and prevent fractures. 7
NCCLs are classified into categories by their shape – that is, wedge, notched, shallow, concave, and irregular. 8 Wedge-shaped defects form similar to a wedge with its base located in the enamel and its pointed end apex located in the dentin. Research by Jakupović et al. 9 showed that V-shaped wedge defects lead to a four-fold increase in mechanical stress concentration at the cavity floor compared with other shapes under the same load conditions. The mechanical stress that occurs is a crucial factor in restoration failure. In addition, the stiffness tensor of the materials used to restore these lesions considerably influences stress distribution and mechanical integration with the tooth. 10 Due to the complex stress patterns to which NCCL restorations are subjected, there is no consensus on the best material to use for restoring these defects. 11 Therefore, it is still an important issue to select the optimal restorative material for NCCL restorations. There are several options for restoring NCCLS, including direct restorations with glass ionomer cement (GIC), resin-modified glass ionomer cement (RGIC), polyacid-modified resin composites, and conventional resin composites while indirect inlay restorations can be performed.11,12 The indirect technique is more expensive and requires a longer treatment time than direct restorations. Therefore, direct restorations are still the most common technique for restoring NCCLs in clinical practice. Although conventional GICs and RGICs are frequently used materials for direct restorations of NCCLs, these materials have limitations, such as mechanical strength, color stability, and retention. 13
The continuous flexion movement in the cervical region that occurs during chewing can adversely affect conventional resin-based materials. 14 Studies have compared flowable and packable resin composites regarding the efficiency of restoring NCCLs and reported that flowable resins generally offer better marginal adaptation but have issues with polishability and surface irregularities due to lower filler content.15,16 To overcome these disadvantages, a new category of flowable resin composite materials, known as injectable composites, has been developed with improved mechanical properties as well as good marginal adaptability. 17 One of these materials, G-aenial Universal Injectable composite, has shown promising biomechanical properties for dental applications. 18
SDR® flow+ (Dentsply Sirona, Charlotte, NC, USA) is marketed as a low stress flowable base material that can be placed in layers up to 4 mm thick. It contains a proprietary patented modified urethane dimethacrylate (UDMA) monomer of high molecular weight and with embedded photoactive groups, which contributes to reduced shrinkage and a better degree of conversion. 19 SDR® flow+ is reported for its superior cavity wall adaptation, polymerization efficiency, and reduced porosity compared with packable bulk-fill materials, and can be used in Class I, III, and V restorations by the manufacturer. 20
Fiber-reinforced resin composites have been developed for restorations in high-stress bearing areas and for enhancing the fracture resistance of the teeth.21,22 In addition, these materials have good adhesion properties due to their semi-interpenetrating polymer network contents. 23 A flowable bulk-fill resin composite (everX Flow™) that was introduced in 2019, is a flowable short fiber-reinforced composite (SFRC) that can be used as a dentin replacement material. To improve its predecessor’s (everX Posterior) handling issues, everX Flow™ has been developed with shorter and thinner fibers than everX Posterior. 24
The incidence of NCCLs has increased due to the longer life expectancy of the population and the longevity of permanent teeth, therefore, the prevention and treatment of these lesions has gained importance. To the best of our knowledge, no study has compared the effect of G-aenial Universal Injectable resin composite and flowable dentin replacement resin composites with or without fiber reinforcement on the fracture resistance of maxillary premolars with NCCLs. This study aimed to compare the fracture resistance of maxillary premolars with wedge-shaped NCCLs restored with the G-aenial Universal Injectable, everX Flow™ bulk shade, or SDR® flow+ bulk-fill flowable composites. The null hypothesis of this study was that the restorations made with flowable SFRC would increase the fracture resistance and improve the fracture pattern of maxillary premolars with NCCLs.
Methods
The materials used in this study are presented in Table 1.
Materials used in the study.
Tooth selection
Ethical approval of this study was obtained from the Non-Interventional Clinic Research Ethics Committee of Zonguldak Bülent Ecevit University (protocol number: 2024/10). The sample size was calculated using G*Power (version 3.1.9.7, Kiel University, Kiel, Germany) and the one-way analysis of variance (ANOVA) for five groups based on the findings of a previous study. 25 The effect size was 0.4, the type I error was α = 0.05, and the statistical power was 0.8. The required total sample size was 70, and the required sample size for each group was 14.
In this study, 75 maxillary first premolar teeth extracted for orthodontic treatment were obtained from patients with age 18–30 years. The teeth were selected according to coronal and root dimensions (Figure 1(a)). The dimensions were measured using a digital caliper (SC- 6 digital caliper, Mitutoyo Corporation, Tokyo, Japan) and the measurements were statistically analyzed (one-way ANOVA, α = 0.05) to establish five experimental groups (n = 15) that were similar to each other.
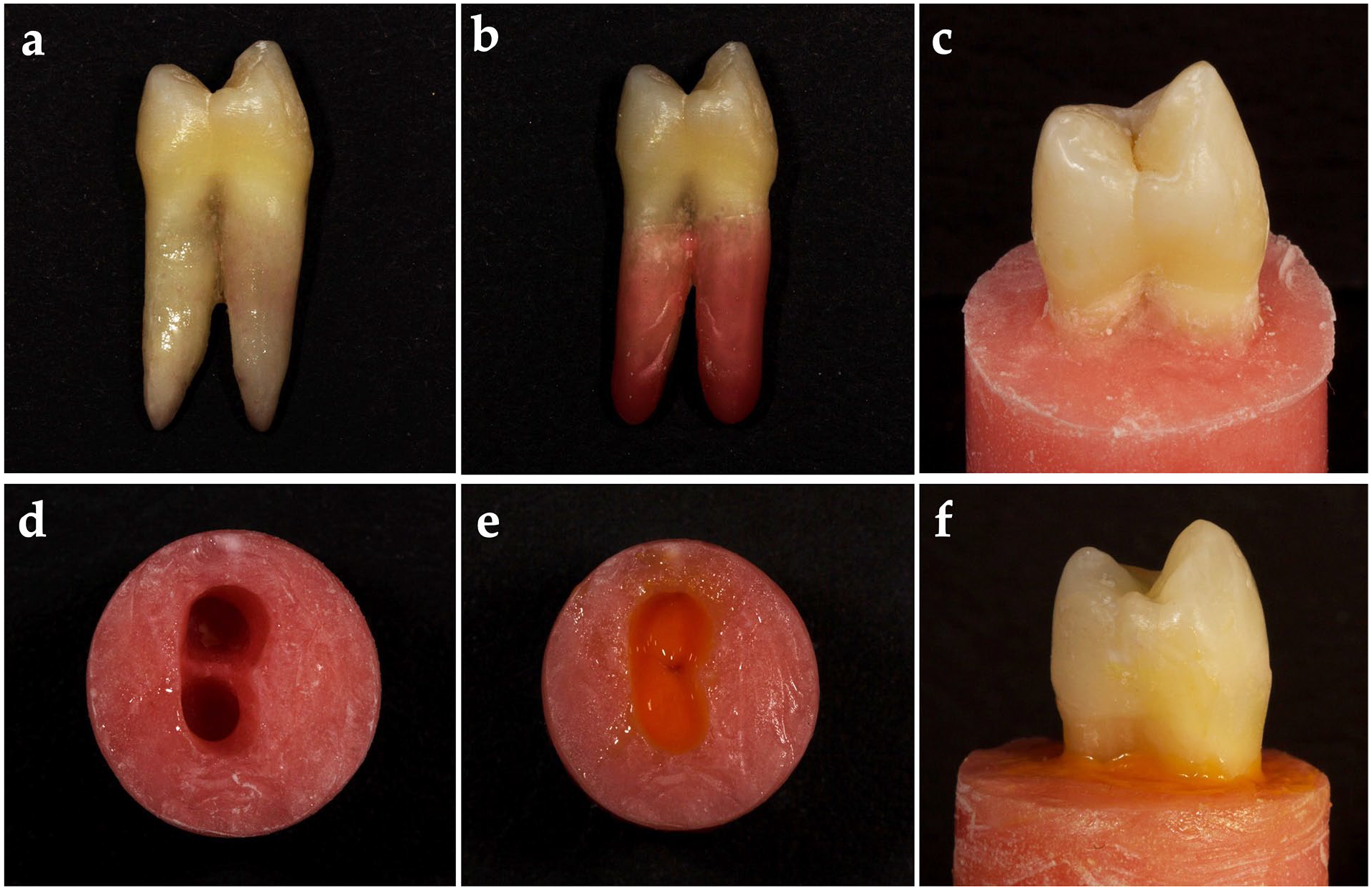
Representative preparation images: (a) Maxillary first premolar teeth extracted for orthodontic treatment were obtained from patients, (b) a wax layer was created by immersing the roots in wax up to 3 mm below the CEJ to create a biological space, (c) teeth were embedded in methacrylate resin up to 3 mm below the CEJ to simulate the alveolar bone limit, (d) the teeth were removed from the methacrylate resin, and the remaining wax removed from the acrylic resin and the root surface using hot water, (e) an elastomeric impression material was placed into the acrylic resin alveolus space, and (f) the teeth were embedded into the space created to simulate the periodontal ligament.
Radiographs were taken from the teeth and those with a buccal enamel and dentin thicknesses of 2.5–3 mm at the CEJ were included. After the removal of debris and soft tissue remnants, teeth were examined under a dental operating microscope (EZ4W, Leica Microsystems, Milton Keynes, UK) to exclude those with cracks or resorptive lesions. The selected teeth were stored in a 0.1% thymol solution at 37°C until use.
Periodontal ligament simulation
The roots of 75 teeth were coated with a base plate wax (Cavex Set Up Regular, Cavex Holland BV, Haarlem, Holland) liquefied at 60°C. A wax layer at approximately 0.3 mm thickness was created by immersing the roots in wax up to 3 mm below the CEJ for 2 s to create a biological space, as reported in previous study (Figure 1(b)). 26 The teeth were then embedded in methacrylate resin (Technovit 4004, Heraeus-Kulzer, Hanau, Germany) up to 3 mm below the CEJ to simulate the alveolar bone limit (Figure 1(c)). Once the polymerization process was complete, the teeth covered in wax were removed from the methacrylate resin, and the remaining wax was removed from the acrylic resin and the root surface using hot water (Figure 1(d)). An elastomeric impression material (Oranwash L, Zhermack, Badia Polesine, Italy) that was mixed with an activator (Indurent gel, Zher-mack) was placed into the acrylic resin alveolus space (Figure 1(e)), then the teeth were embedded into this space to simulate the periodontal ligament (Figure 1(f)). The prepared specimens were stored in distilled water at 37°C until being subjected to the fracture resistance test.
Wedge-shaped lesion preparations
Standardized artificial wedge-shaped NCCLs were prepared on the facial surface of 60 teeth using a fissure diamond bur (G837/018, Dia Tessin, Vanetti, Gordevio, Switzer-land) under water cooling by a single trained operator (EH), while 15 were left unprepared as the intact teeth (positive control group). Diamond burs were not used for more than three cavity preparations. The artificial lesion dimensions were prepared with a height of 4 mm (2 mm above and 2 mm below the CEJ; Figure 2(a)), a 2 mm depth (in the midline of the lesion and at the CEJ level; Figure 2(b)), and with a full mesiodistal width (extending from the mesial line angle to the distal line angle; Figure 2(c)) and checked with a periodontal probe (Hu-Friedy Mfg. Co., Chicago, IL, USA).
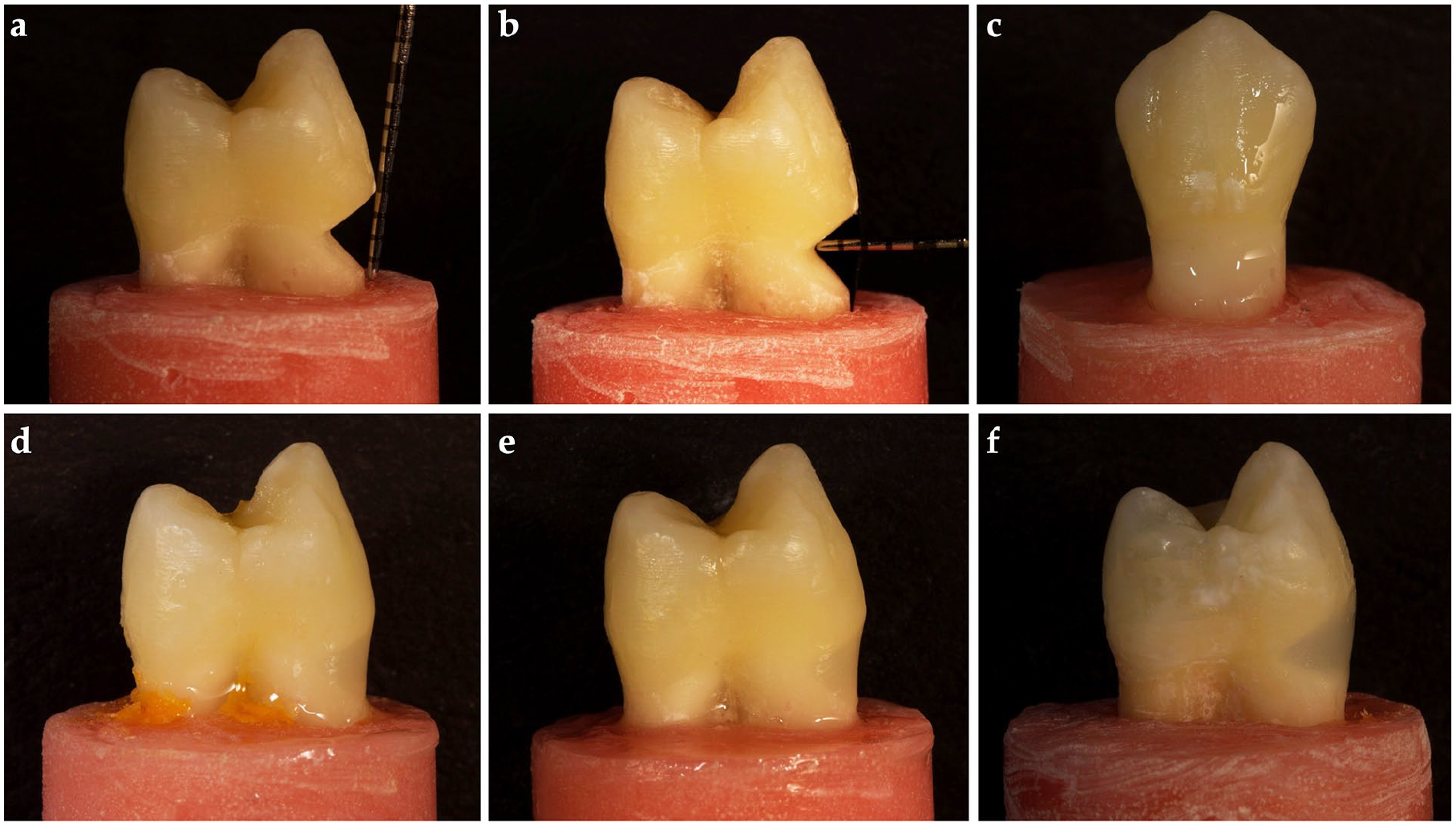
Representative preparation images: (a, b, c) The measurements of the artificial NCCL cavity dimensions were made with a periodontal probe, (d) the cavities were restored with universal injectable composite (G-aenial), (e) the cavities were restored with universal injectable a flowable bulk-fill composite (SDR® flow+), and (f) the cavities were restored with a flowable SFRC (everX Flow™).
Adhesive application
Adhesive application and restoration procedures were performed by a single operator (AH) on 45 teeth, while 15 teeth were left untreated as the negative control group. The enamel was selectively etched with 37% phosphoric acid (RubyEtch, rubydent, Istanbul, Türkiye) for 15 s, rinsed with water, and dried with an air–water spray. The adhesive (Scotchbond Universal Plus Adhesive, 3M Deutschland GmbH, Neuss, Germany) was applied to the dentin, cementum, and enamel walls of the cavity and rubbed in for 20 s. The adhesive was then gently air-dried for 5 s, and light-cured for 10 s using a light-emitting diode (LED) dental curing unit (Elipar S10, 3M ESPE, USA) at 1200 mW/cm². After adhesive application, specimens were divided into three groups based on the materials used for the restoration of the cavities (n = 15).
Restorative procedures
The prepared NCCLs were restored with three different materials: universal injectable composite (G-aenial) on 15 teeth (Figure 2(d)), a flowable bulk-fill composite (SDR® flow+ on 15 teeth (Figure 2(e)), and a flowable SFRC (everX Flow™) on 15 teeth (Figure 2(f)). The restorations were light-cured from the facial surface of the teeth for 20 s using an LED dental curing light. The finishing and polishing procedures were performed using alumina disks (OptiDisc, Kerr, Bioggio, Switzerland).
Fracture resistance test
The specimens were subjected to a fracture resistance test using a universal testing machine (Lloyd LRX; Lloyd Instruments Ltd., Fareham, UK) with a 4-mm-diameter crosshead. A 30° oblique compressive load was applied to the long axis of the tooth and at the inner incline center of the buccal cusp at a constant speed of 0.5 mm/min (Figure 3(a)). The fracture patterns were inspected visually with a dental operating microscope (EZ4W, Leica Microsystems, Milton Keynes, UK) at ×40 magnification by a single operator (AH) to categorize them as repairable (fractures not extending below the CEJ; Figure 3(b)), possibly repairable (fractures extending below the CEJ, but not below the acrylic line; Figure 3(c)), or unrepairable (fractures extending below the acrylic line; Figure 3(d)). The frequency percentages of the identified fracture patterns were recorded as described.
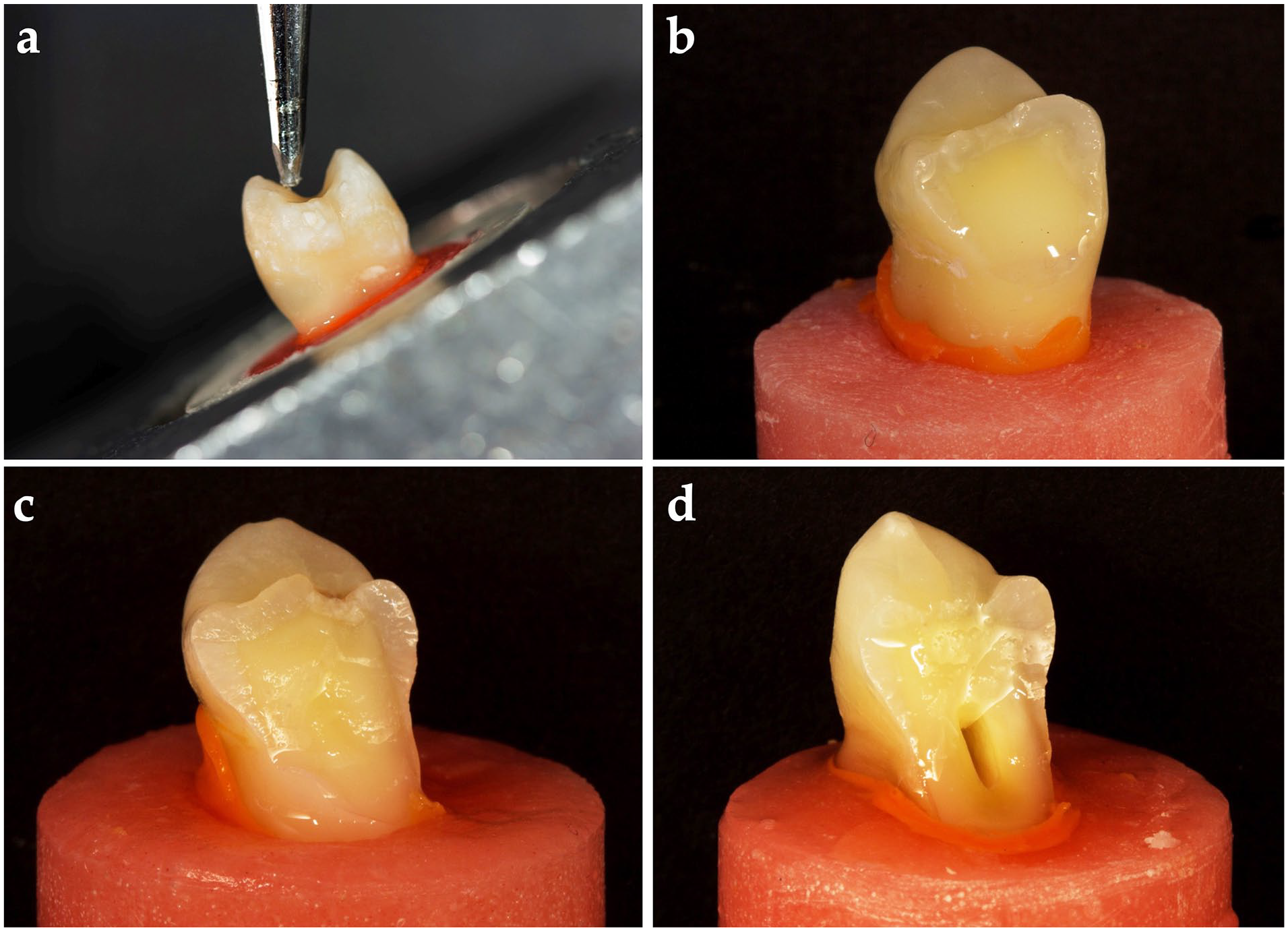
(a) Fracture resistance test, (b) representative image of the repairable fracture pattern (fractures not extending below the CEJ), (c) representative image of the possibly repairable fracture pattern (fractures extending below the CEJ but not below the acrylic line), and (d) representative image of the unrepairable fracture pattern (fractures extending below the acrylic line).
Statistical analyses
IBM SPSS (V23, Chicago, IL, USA) software was used to analyze the data. The Shapiro–Wilk test was used to confirm if the data had a normal distribution according to the groups. One-way ANOVA was used to compare the fracture resistance values of the groups and the difference between them was analyzed with Tukey’s honest significant difference post-hoc test. The frequency percentages of the fracture patterns between the groups were compared using Pearson’s chi-squared test. The level of statistical significance was 0.05.
Results
Figure 4 presents the mean and standard deviation values of the groups tested in this study. Considering the one-way ANOVA results, there was a significant difference between the fracture resistance values of the groups (p < 0.001). According to Tukey’s honest significant difference, the highest fracture resistance values were found in the positive control/intact teeth group (743.481 N), followed by the everX Flow™ (673.787 N), G-aenial Universal Injectable composite (553.289 N), SDR® flow+ (497.368 N), and the negative control (unrestored cavities; 371.49 N) groups (p < 0.001). The mean fracture resistance values of the SDR® flow+ and the G-aenial Universal Injectable composite groups were not significantly different (p = 0.055).
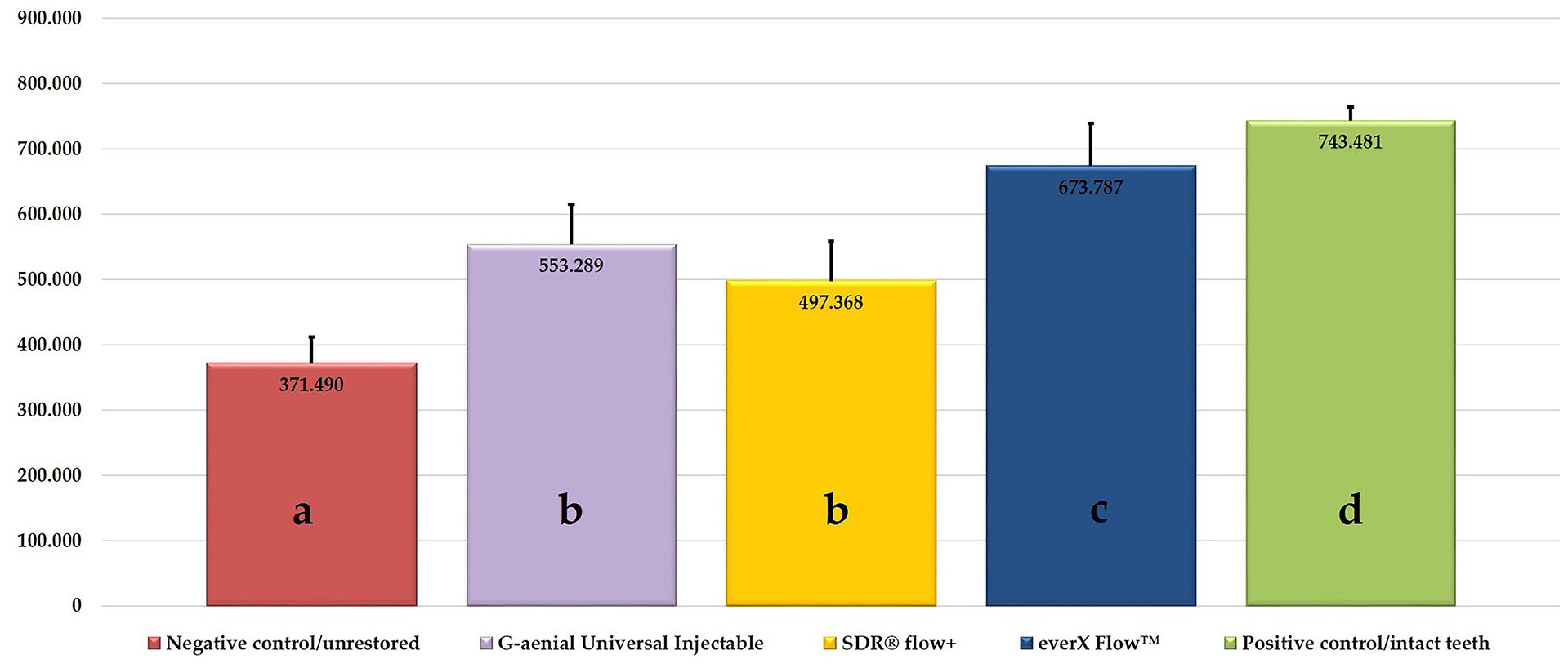
The mean and standard deviation fracture resistance values of the groups (one-way ANOVA/Test statistic: 135.383/p < 0.001).
Figure 5 illustrates the fracture pattern distributions of the groups. The type of restorative material used significantly affected the repairability of the fractures (p < 0.001). The positive control/intact teeth group had the highest repairability rate at 100%, followed by the everX Flow™ group with 60%. In contrast, the negative control group had the lowest repairability rate at 13.3% and the highest percentage of unrepairable (60%) and possibly repairable (26%) fractures. The fracture pattern in G-aenial Universal Injectable composite (53.3%) and SDR® flow+ (53.3%) groups was mostly unrepairable.
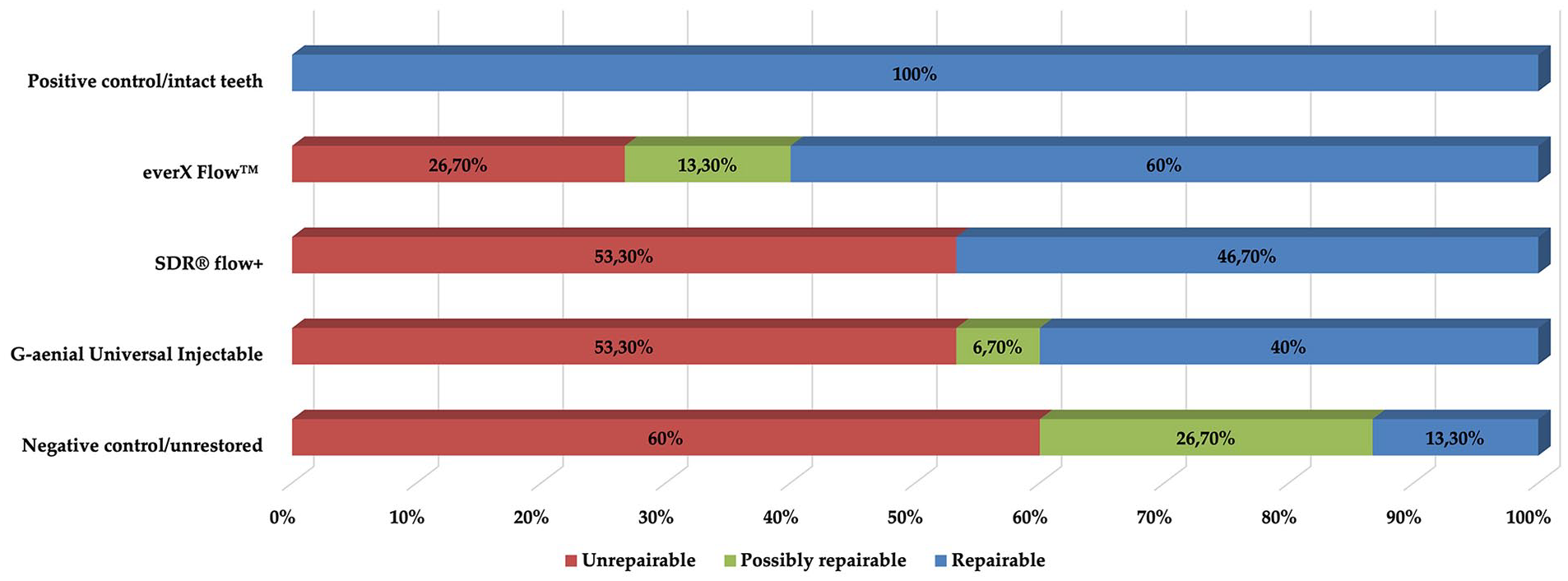
The fracture pattern distributions of the groups.
Discussion
The fracture resistance of maxillary first premolars with artificial NCCLs restored using different materials was evaluated in this study. NCCLs are dental defects with a prevalence of 53%–72%, most commonly affecting maxillary premolars. These teeth have a thin dentin volume in the cervical region and sharp cusp inclinations that make them vulnerable to compressive and shear bite forces during chewing, thus, are susceptible to NCCLs and tooth fractures.6,27 Therefore, maxillary first premolars were subjected to oblique compressive load for fracture resistance tests in this study.
It is reported that the standardization of artificially prepared NCCLs can be challenging for extracted teeth due to morphological variations. 28 In this study, maxillary first premolars that were extracted due to orthodontic reasons from patients between age 18–30 years were used to minimize the dimensional variation in teeth selection. In addition, for standardization, the mesiodistal and buccopalatal dimensions in both the coronal and cervical parts of the teeth were measured and statistically analyzed to establish whether the teeth dimensions were similar or not.
Periodontal ligaments establish a functional connection between the alveolar bone and the cementum structure of teeth, enabling minor teeth movements in the alveolar space. Thus, bone and the periodontal ligaments can influence the fracture pattern by affecting the force transmission to the tooth. 26 In the experimental model, the absence of simulating periodontal ligament results in the tooth root being fully attached to the model, thereby replicates the characteristics of an ankylotic tooth. It can be predicted that this situation will create a difference in force transmission from the teeth to the alveolar bone and reduce clinical mimicking. In this study, elastomeric impression material was used to simulate the periodontal ligament and acrylic resin was used to simulate the alveolar bone to obtain more accurate results.
There are several morphological shapes of NCCLs. 8 In maxillary premolars, wedge-shaped lesions are more prevalent on the facial surface of the cervical area due to the tensile stress of occlusal forces. Therefore, artificial wedge-shaped NCCLs were prepared on the facial surfaces of the cervical area for this study.
Dynamic loading is designed to simulate the functional mastication forces and is informative in determining how materials behave under normal occlusal forces. Static loading mimics the parafunctional forces that occur when biting hard foods (i.e. nuts), or bruxism for which approximately one of ten adults is likely to suffer as reported in an epidemiological study. 29 Psychological factors, such as depression and anxiety, are associated with bruxism and with the increase in cases worldwide, the simulation of traumatic forces is becoming increasingly important. 30 The fracture resistance of the restorative material when exposed to occlusal forces and its ability to strengthen the remaining tooth structures are important factors for a successful restoration. It is possible that NCLLs, which often occur because of exposure to parafunctional forces, can still be exposed to higher-than-normal occlusal forces after restorative treatment. Therefore, static force was applied in this study to establish the maximum resistance of different materials used to treat these lesions.
The negative control/unrestored group had significantly lower fracture resistance values while the intact teeth/positive control group had significantly higher values than the restored groups, which is consistent with previous studies.31,32 Zeola et al. 32 reported that NCCLs evaluated with Finite Element Analysis increased stress concentration around the cervical region even if as shallow as 0.5 mm, and that the stress magnitude increased with the lesion size. This data shows that restoring the NCCL with resin-based materials adds strength by providing a more homogeneous distribution of functional loads within the tooth structure, among other requirements (i.e. prevention of sensitivity and plaque retention or aesthetic requirements). This data indicates the importance of NCCL restorations as they can replace lost dental tissues and restore strength. In addition to the findings mentioned earlier, Zeola et al. 32 reported that the fracture resistance of composite-restored NCCLs increased almost to the fracture resistance level of intact teeth. However, none of the restored groups showed as much fracture resistance as the intact tooth in the current study. Discordance in the findings might be due to these methodological differences. It is stated that the depth of NCCLs affects the strain distribution. 33 Natural dentin is reinforced by collagen fibers that can stop and deflect cracks initiated in enamel thus larger NCCLs make the teeth more prone to fracture. The reason why the fracture resistance of the restored groups was not as high as the fracture resistance of the intact tooth may be due to the larger NCCLs prepared in this study. In the study by Zeola et al., 32 a packable composite was used and the cavity depth was prepared at 1.5 mm at most. In our study, both flowable restorative materials were used and the prepared cavities were deeper (2 mm) and higher (4 mm). Therefore, further studies are needed for extended NCCL restorations made with different materials with properties similar to healthy teeth and resist physiological or parafunctional forces.
In this study, there was no significant difference in the fracture resistance of the teeth restored with the G-aenial Universal Injectable composite (553.289 N) and the SDR® flow+ bulk-fill composite (497.368 N). There are several studies contrary to our results showing that bulk-fill resin composites have better fracture resistance compared with conventional resin composites in different cavity types.34,35 The polymerization shrinkage and depth cure of bulk-fill resin composites play a crucial role in the fracture resistance of restorations. 36 The reduced polymerization shrinkage and increased depth cure properties of these materials give them an advantage over conventional resin composites when restoring cavities with high C-factor by improving the overall quality and durability of the restorations. 37 NCCL cavities have a smaller C-factor that minimizes the effect of bulk-fill materials’ advantages, such as polymerization shrinkage due to the cavity shape. Therefore, the success of NCCL restorations is mostly dependent on the material’s bonding capability and strength properties. 38 Thus, the reason that there were no differences in fracture resistance between the conventional composite and bulk-fill composite without fiber-reinforcement could depend on the cavity shape that we tested in this study. de Abreu et al. 31 compared the effect of nanohybrid and bulk-fill resin composites on the fracture resistance of artificial NCCLs with similar dimensions to those prepared in this study and found no significant difference between the fracture resistance of materials tested, which was consistent with our study results.
In this study, the everX Flow™ group had significantly higher fracture resistance values among the restored groups. It is known that inorganic filler ratios and resin types affect the mechanical properties of materials. 39 In this study, the inorganic filler ratios and resin types of the materials tested were similar, therefore, it is possible that the difference between the fracture resistance of the materials was due to the fiber content of everX Flow™.
The flexural modulus influences stress distribution; higher stiffness materials increase stress in cervical regions, while lower stiffness materials reduce stress effectively in the lesion area. 40 In a current study, Szczesio-Wlodarczyk et al. 41 reported that there was no difference between the flexural modulus of the materials tested in this study. Therefore, the difference in fracture resistance of restorations made with these materials may be due to whether they contain fibers or not.
It is reported that everX Flow™ has increased fracture toughness and fatigue strength than resin composites, since the fibers within are oriented randomly and are three-dimensionally isotropic in all directions. 42 In addition, the inclusion of short fibers in a semi-IPN resin matrix led to substantial improvements in this mechanical property. The behavior of E-glass fiber’s behavior in resin matrix provides a crack-stopping therefore, a small crack propagating through the material cannot grow any further when it encounters these fibers. 22 Conversely, dentin replacement material containing modified UDMA or injectable nanohybrid universal composite consists of small filling particles and does not contain particles that can prevent crack formation. 43 Furthermore, randomly orientated E-glass fibers can dissipate energy, which improves their mechanical performance. Due to the different materials and preparation techniques used, no study can be directly compared with the results of this study. However, these results are consistent with previous studies evaluating fracture resistance in different cavity types, such as mesio-occlusal-distal cavities.21,24,44
In terms of fracture pattern, in teeth restored with everX Flow™, more repairable fractures were observed when compared with G-aenial Universal Injectable composite, SDR® flow+ bulk-fill composite, and unrestored teeth. It is reported that short-glass fibers in fiber-reinforced resin composites break gradually to reduce the stress energy at the crack tip by upscaling the crack deflection mechanism to macrometric events under the stress load. 45 Therefore, consistent with previous studies, the observation of dominantly repairable fracture patterns in everX Flow™ group was not unexpected.21,42 The null hypothesis that the NCCL restorations made using a flowable SFRC in maxillary premolars would increase the fracture resistance and improve the fracture pattern of the restorations was accepted.
One of the limitations of this study was the inability to create in the laboratory, cervical lesions occurring under natural process. Another limitation is static load-to-fracture testing was used without fatigue testing and multiple directions of actual biting force. Furthermore, clinically these types of restorations are frequently exposed to abrasive wear or acidic erosion. The limitation of SFRC may be the degradation of its surface and exposure of fibers due to these factors. Further studies are needed to include the wear resistance, surface roughness, and discoloration of these materials, and the effect of thermal aging should also be investigated.
Consclusion
Within the limitations of this study:
- Wedge-shaped NCCLs reduced the fracture resistance of maxillary first premolar teeth, while direct restoration of these lesions increased the fracture resistance of teeth.
- everX Flow™ provided teeth with NCCL higher fracture resistance than SDR® flow+ and G-aenial Universal Injectable.
- Flowable short-fiber-reinforced composite restorations demonstrated a more favorable fracture pattern on teeth with wedge-shaped NCCLs than restorations without fiber reinforcement.
Footnotes
Author contributions
AH and EH researched the literature and conceived the study. AH was involved in protocol development, prepared the specimens, and performed the experiments. AH analyzed the data. AH wrote the first draft of the manuscript. AH and EH reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.